Deep Vein Thrombosis: History and Discovery
Deep vein thrombosis (DVT) is a blood clot that forms in one of the deep veins of the body, most often in the leg or pelvis. Its great danger is that a piece of the clot can break loose, travel through the heart, and lodge in the lungs — a pulmonary embolism. The story of how physicians came to understand this condition stretches from a frightening swelling of the leg called “milk leg,” first described in the 16th century, through the laboratory of Rudolf Virchow in the 1850s — who coined the very words thrombosis and embolism and proved that leg clots could travel to the lungs — to the accidental discoveries of heparin (1916) and warfarin (1940s), and finally to today’s blood tests, ultrasound scans, and direct oral anticoagulants. This page traces that history with care to separate what was actually observed from what was later inferred, and to credit discoverers honestly.
Table of Contents
- What Deep Vein Thrombosis Is
- Milk Leg: Phlegmasia Alba Dolens
- John Hunter and the Idea of Phlebitis
- Rudolf Virchow: Thrombosis and Embolism
- Virchow’s Triad — An Honest Account
- The Discovery of Heparin (1916)
- Spoiled Sweet Clover and Warfarin
- Seeing the Clot: Venography, Ultrasound, and D-Dimer
- The Modern Era of Treatment
- Research Papers and References
- Connections
- Featured Videos
What Deep Vein Thrombosis Is
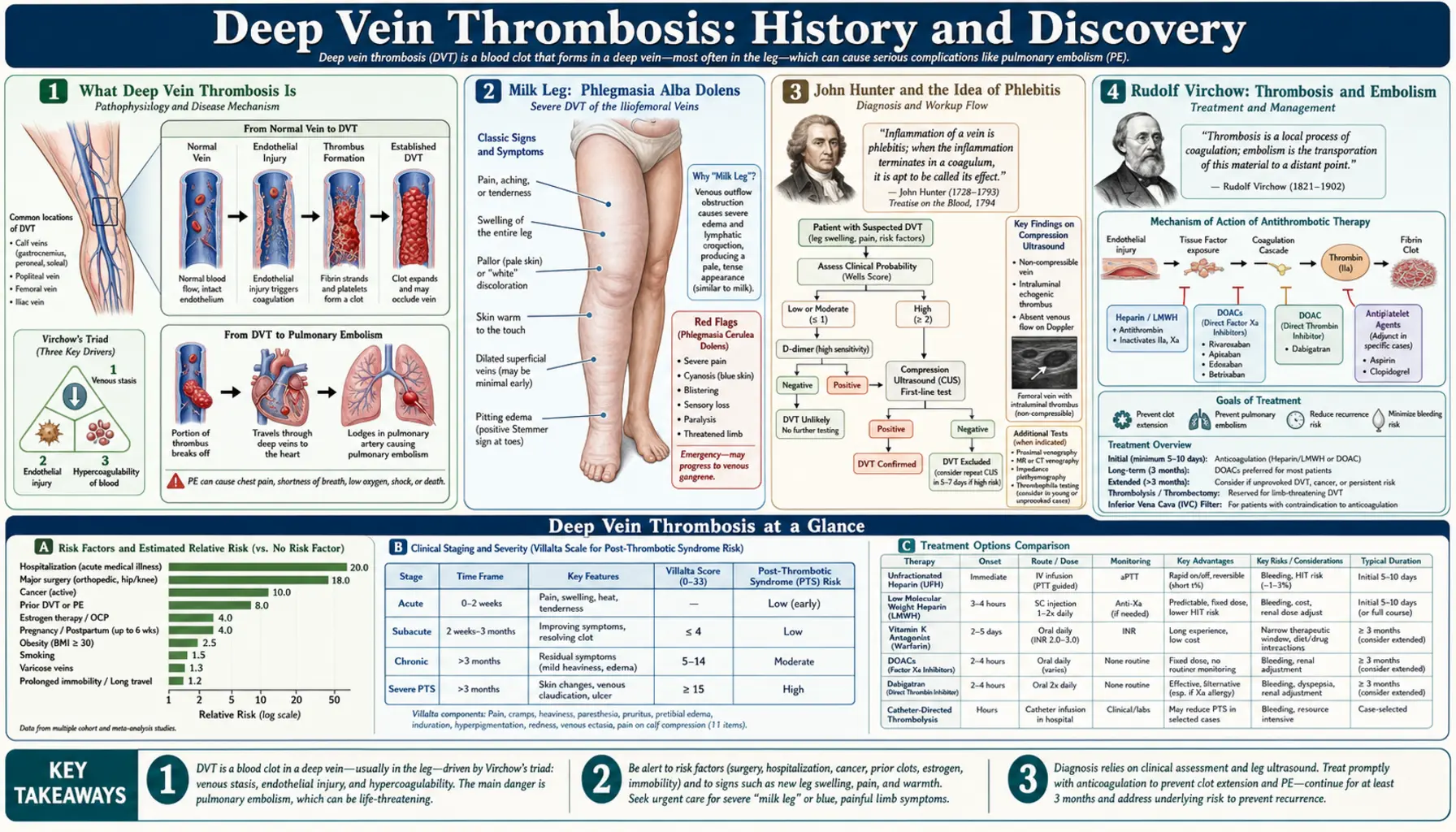
A deep vein thrombosis is a clot that forms inside one of the deep veins that carry blood back toward the heart — most commonly the large veins of the calf, thigh, and pelvis. Unlike the harmless clotting that seals a cut, a clot inside an intact vein partly or wholly blocks the flow of blood, causing the classic signs of pain, swelling, warmth, and sometimes a reddish or bluish color in the affected leg. Many clots, however, cause few or no symptoms at all, which is part of what makes the condition dangerous.
The gravest complication is pulmonary embolism. A fragment of the leg or pelvic clot can detach, ride the venous bloodstream up through the right side of the heart, and become wedged in the arteries of the lungs, where it can be sudden and fatal. Because the two events are really two ends of a single process, modern medicine groups them under one umbrella term, venous thromboembolism (VTE). Understanding that a clot in the leg and a clot in the lung are the same disease in two places was, as we will see, one of the central historical breakthroughs — and it belongs above all to Rudolf Virchow.
The remaining sections of this page follow how that understanding was built: first the long pre-scientific era of careful bedside observation, then the 19th-century laboratory work that explained the mechanism, and finally the 20th- and 21st-century tools that let physicians detect and treat clots before they kill. For the clinical picture, risk factors, and present-day management, see the main Deep Vein Thrombosis article.
Milk Leg: Phlegmasia Alba Dolens
Long before anyone understood blood clots, physicians recognized a dramatic and frightening condition of the leg: a sudden, painful, tense swelling in which the limb turned strikingly pale and white. The Latin name that came to describe it, phlegmasia alba dolens, translates roughly as “painful white inflammation.” The condition is generally traced in the medical literature to a description by the surgeon Guilielmus Fabricius Hildanus (Wilhelm Fabry) in the 16th century, and it was noted especially — and most memorably — in women in the days and weeks after childbirth.
Because it appeared so often in new mothers, the condition acquired the folk name “milk leg” (and the Latin phlegmatia lactea). The name reflected a now-discarded theory: 18th-century clinicians such as Anthony Puzos (1759) and André Levret (1766) connected the swelling to the puerperal period and supposed that the white, swollen limb was caused by milk being somehow diverted or “driven down” into the leg instead of going to the breasts. This is an important place to be honest about history: the observation — a painful, pale, swollen postpartum leg — was accurate and is exactly what we would now recognize as a severe iliofemoral deep vein thrombosis. The explanation — displaced milk — was wrong. The true cause is obstruction of the deep veins by clot, often where the enlarged uterus of late pregnancy and the changes of childbirth slow and stress the pelvic veins.
It is worth keeping the two layers separate whenever reading old medical accounts. Careful observers across centuries described real and reproducible patterns of disease; the theories they attached to those patterns were limited by the science of their day. “Milk leg” survived as a lay term well into the 20th century, but the milk theory did not survive contact with the microscope and the autopsy table. (In its most extreme modern form, a massively swollen, blue, and threatened limb from near-total venous outflow obstruction is still called phlegmasia cerulea dolens — the painful blue swelling — a vascular emergency.)
John Hunter and the Idea of Phlebitis
The bridge from pure description toward mechanism was built in part by the great Scottish surgeon-anatomist John Hunter in the late 18th century. Hunter, working in London and writing in the 1780s and 1790s, paid close attention to inflammation of the veins — phlebitis — and observed that inflamed veins frequently contained clotted blood. He recognized a connection between the inflamed, diseased vein wall and the formation of a clot within it, and he is often credited with early efforts to tie the swollen limb to a problem in the vein itself rather than to displaced milk or vague “humors.”
For much of the early 19th century, the prevailing view — later championed forcefully on the European continent — held that clotting was essentially a consequence of inflammation of the vessel wall, a doctrine sometimes summarized under the heading of “phlebitis.” This was a reasonable inference from the bedside: inflamed veins and clots did appear together. But it put the causal arrow in a particular direction — inflammation first, clot second — and it would take careful pathological work to test whether that order was always correct, or whether clots could form and then provoke the surrounding reaction.
This is the intellectual stage onto which Rudolf Virchow stepped. The question was no longer simply “what is this swollen white leg?” but “what exactly is a clot, where does it come from, where does it go, and what makes it form?” Answering those questions rigorously, with experiments and autopsies rather than theory alone, transformed the subject from descriptive medicine into pathophysiology.
Rudolf Virchow: Thrombosis and Embolism
The decisive figure in this history is Rudolf Ludwig Carl Virchow (1821–1902), the German physician widely regarded as the founder of modern cellular pathology. In a series of investigations published in the mid-1850s — with his landmark work on this subject appearing in 1856 — Virchow gave the field two of its most fundamental words. He introduced the term thrombosis for the process by which a solid clot (a thrombus) forms within a blood vessel, and he coined embolism for the event in which a fragment breaks off and is carried by the bloodstream to lodge somewhere distant. These terms are so basic to medicine today that it is easy to forget they had to be invented.
Virchow’s most important demonstration was experimental and anatomical. Through meticulous postmortem study he noticed that clots in the lungs and clots in the leg veins tended to occur together, and that a lung clot was often shaped as though it had broken off a larger clot elsewhere — the pieces, in effect, could be fitted back together. To test the idea that material from the peripheral veins could travel to the lungs, he introduced foreign bodies (including fragments of clot and other materials) into the jugular veins of animals and showed that they consistently ended up lodged in the pulmonary vessels. This was direct evidence that a clot in the body’s veins could detach and embolize to the lung — precisely the leg-to-lung pathway that defines venous thromboembolism. Crucially, Virchow also argued against the older “phlebitis-first” doctrine, contending that thrombus formation was not merely a downstream result of vessel inflammation.
With this work, the central fact of the disease snapped into focus: a clot in a deep vein and a clot in the lung are not two unrelated misfortunes but two stages of one event. That single insight underlies essentially everything that follows in the prevention and treatment of DVT and pulmonary embolism. It is the reason a swollen calf is taken seriously, why hospitalized patients receive clot prophylaxis, and why the two conditions share a name today.
Virchow’s Triad — An Honest Account
Every medical student learns “Virchow’s triad”: the three broad categories of factors that promote clotting — slowed blood flow (stasis), a tendency of the blood itself to clot too readily (hypercoagulability), and injury to the vessel wall / its inner lining (endothelial injury). Together these still organize how clinicians think about why a clot forms: a long flight (stasis), an inherited clotting disorder or cancer or pregnancy (hypercoagulability), and surgery or trauma to a vein (vessel injury). The framework is genuinely useful, and it genuinely descends from Virchow’s thinking. But the familiar packaged “triad” deserves an honest footnote, because the history is more tangled than the textbook suggests.
Here is the nuance, well documented by historians of medicine. Virchow did discuss the categories of factors that contribute to thrombosis, and his work is the legitimate root of the concept. However, scholars who have gone back to his original writings point out two things. First, the neat name “Virchow’s triad,” as a fixed three-part formulation, does not appear in Virchow’s own work and seems not to have entered the literature until long after his death — one frequently cited estimate places the phrase’s emergence around the early 1950s, roughly a century after his 1856 publication. Second, the modern triad as usually listed — particularly the explicit inclusion of endothelial (vessel-wall) injury as one of the three pillars — does not map cleanly onto Virchow’s own categories; by several accounts he did not frame endothelial injury as one of three co-equal elements in the way the eponymous triad implies.
So the careful, accurate statement is this: Virchow described the components and the mechanism; the three-part “triad” as a named, codified formula was assembled and attached to his name later, as the 20th century accumulated experimental evidence for the roles of stasis, blood composition, and the vessel wall. None of this diminishes Virchow — if anything it shows how productive his ideas were. But on a health-information page accuracy matters, and it would be wrong to claim that Virchow himself wrote down “the triad.” He laid the foundation; later generations built the tidy structure that bears his name.
The Discovery of Heparin (1916)
Understanding clots is one thing; being able to prevent or dissolve them is another, and for that, medicine needed drugs. The first great anticoagulant arrived, as so many discoveries do, partly by accident. In 1916, a second-year medical student at Johns Hopkins named Jay McLean, working in the physiology laboratory of Professor William Henry Howell, was investigating substances thought to promote clotting. While studying fatty extracts (phosphatides) from tissues, McLean isolated a fat-soluble substance that did the opposite of what he was looking for: instead of speeding clotting, it powerfully prevented the blood from clotting. The anticoagulant was subsequently obtained from liver tissue, and because hepar is the Greek word for liver, the substance was given the name heparin — a name first applied around 1918.
Honesty about credit matters here, because the discovery of heparin became one of medicine’s long-running attribution disputes. Both Howell, the laboratory’s director, and McLean, the student who made the key observation, are tied to the discovery, and the relative share each deserves has been debated for over a century. McLean himself, decades later, pressed his claim to priority, and his account gradually gained wide acceptance. The fair summary is that McLean made the pivotal initial observation of the anticoagulant activity in 1916 while a student in Howell’s laboratory, and that Howell’s laboratory continued the work that characterized and named the substance. We present both names because the record genuinely involves both.
Whatever the precise apportioning of credit, the consequences were enormous. After considerable further work over the following decades to purify heparin and make it safe and reliable, it became — and remains — a frontline drug for preventing and treating venous thromboembolism. Heparin acts quickly and is given by injection or infusion, making it the workhorse for hospitalized patients, for the initial treatment of an acute clot, and for clot prevention during surgery. The 1916 observation in a student’s laboratory notebook ultimately saved, and continues to save, countless lives.
Spoiled Sweet Clover and Warfarin
The second landmark anticoagulant has an even stranger origin, beginning not in a hospital but on the cattle farms of the northern plains. In the 1920s, veterinarians in the United States and Canada described a mysterious and deadly bleeding disease in cattle. The Canadian veterinary pathologist Frank Schofield reported in 1924 that the culprit was spoiled sweet clover hay: when the sweet clover used as fodder became moldy, cattle that ate it suffered uncontrollable internal bleeding — “sweet clover disease.” Something in the spoiled hay was acting as a potent anticoagulant.
The decisive chapter belongs to the biochemist Karl Paul Link at the University of Wisconsin. The well-known and well-documented turning point came during a 1933 winter blizzard, when a desperate Wisconsin farmer named Ed Carlson drove some 200 miles to Link’s laboratory in Madison carrying a dead cow, a milk can of unclotting blood, and a load of the spoiled hay that had killed his herd. Spurred by this, Link and his students worked to identify the responsible agent. Over the following years his laboratory crystallized and identified the anticoagulant compound — a coumarin derivative they named dicoumarol — which then entered clinical use as one of the first oral anticoagulants and was studied at institutions including the Mayo Clinic.
From that research program Link’s group went on to synthesize a more potent related compound, patented in 1945 and named warfarin — the name combining the acronym WARF (the Wisconsin Alumni Research Foundation, which funded and held the patent) with the “-arin” ending of coumarin. Warfarin was first marketed in the late 1940s and 1950s as a rat poison (a rodent that ate it bled to death), and only afterward was it embraced as a human medicine. As an oral pill, warfarin transformed the long-term prevention of clots: unlike injected heparin, it could be taken at home for months or years. It dominated outpatient anticoagulation for half a century — though it requires regular blood-test monitoring and careful attention to diet and drug interactions, limitations that eventually motivated the search for simpler agents.
Seeing the Clot: Venography, Ultrasound, and D-Dimer
For most of medical history, a deep vein clot could only be inferred from symptoms or confirmed at autopsy. The first way to actually see a clot in a living patient was contrast venography (also called phlebography): a dye opaque to X-rays is injected into a vein, and a clot shows up as a gap or filling defect in the image. Venography became the diagnostic reference standard of the 20th century and was genuinely informative, but it is invasive, uncomfortable, exposes the patient to radiation and contrast dye, and can itself irritate the vein. Clinicians wanted something safer.
The transformation came with compression ultrasound. Ultrasound creates images using harmless sound waves, and the technique for veins is elegantly simple in principle: a normal vein collapses flat when the probe presses on it, but a vein packed with clot will not compress. From the late 20th century onward, duplex/compression ultrasonography proved highly sensitive and specific for clots in the proximal leg veins, and because it is non-invasive, radiation-free, repeatable, and increasingly portable, it largely replaced venography as the first-line test for suspected DVT. Today a leg ultrasound is the standard confirmatory study.
The third modern pillar is a blood test, the D-dimer. D-dimer is a fragment released when the body breaks down a clot; a raised level signals that clotting and clot breakdown are occurring somewhere. Its real power, recognized and refined over roughly the last few decades, is as a rule-out test: in a patient judged to be at low or moderate risk by a clinical scoring system, a normal D-dimer makes a clot very unlikely and can spare that patient an ultrasound altogether. Combined into structured diagnostic algorithms — clinical probability score, then D-dimer, then ultrasound only if needed — these tools let physicians diagnose or confidently exclude DVT quickly, safely, and without the older invasive imaging.
The Modern Era of Treatment
For decades, the standard treatment of a deep vein clot followed a familiar two-drug rhythm: start fast-acting injectable heparin (later, conveniently, low-molecular-weight heparin given as a once- or twice-daily subcutaneous injection) to halt the immediate threat, then transition to oral warfarin for months of ongoing protection. This regimen worked and saved lives, but warfarin’s narrow safety margin, its need for frequent blood-test monitoring to keep the dose in range, and its many food and drug interactions made it burdensome for patients and clinicians alike.
The most recent revolution is the arrival of the direct oral anticoagulants (DOACs) — sometimes called NOACs. These pills block a single specific clotting factor: dabigatran, a direct thrombin (factor IIa) inhibitor, was first approved in 2008; the direct factor Xa inhibitors rivaroxaban (2011) and apixaban (2012), with edoxaban following, arrived shortly after. In large trials they proved at least as effective as the old heparin-plus-warfarin approach for treating and preventing venous thromboembolism, generally with less serious bleeding, and — the practical breakthrough for patients — they are taken at fixed doses by mouth without the routine blood-test monitoring warfarin demands. For many people with DVT today, treatment is now simply a pill.
Seen whole, the arc is remarkable. A baffling white swelling once blamed on displaced milk became, through Virchow’s laboratory, a clearly understood clot that travels from leg to lung; two accidental discoveries — from a student’s extract and from spoiled cattle feed — gave medicine its first anticoagulants; ultrasound and a blood test made the clot visible and excludable in minutes; and modern pills made treatment safer and simpler than ever. For how DVT is recognized, prevented, and managed today, continue to the main Deep Vein Thrombosis article, and to the closely related Pulmonary Embolism page.
Research Papers and References
The references below combine peer-reviewed historical and clinical reviews — with DOIs or PMIDs where a specific source is cited confidently — with curated PubMed topic-search links for further reading. Where the historical record is genuinely contested (for example, the precise attribution of heparin’s discovery, or the post-mortem assembly of “Virchow’s triad”), the article above marks the nuance rather than overstating certainty. Each external link opens in a new tab.
- Bagot CN, Arya R. Virchow and his triad: a question of attribution. British Journal of Haematology. 2008;143(2):180-190. — doi:10.1111/j.1365-2141.2008.07323.x
- Cervantes J, Rojas G. Virchow’s Legacy: Deep Vein Thrombosis and Pulmonary Embolism. World Journal of Surgery. 2005;29(Suppl 1):S30-S34. — doi:10.1007/s00268-004-2056-0
- Kumar DR, Hanlin E, Glurich I, et al. Virchow’s contribution to the understanding of thrombosis and cellular biology. Clinical Medicine & Research. 2010;8(3-4):168-172. — doi:10.3121/cmr.2009.866
- Wardrop D, Keeling D. The story of the discovery of heparin and warfarin. British Journal of Haematology. 2008;141(6):757-763. — doi:10.1111/j.1365-2141.2008.07119.x
- Mueller RL, Scheidt S. History of drugs for thrombotic disease: discovery, development, and directions for the future. Circulation. 1994;89(1):432-449. — doi:10.1161/01.CIR.89.1.432
- Link KP. The discovery of dicumarol and its sequels. Circulation. 1959;19(1):97-107. — doi:10.1161/01.CIR.19.1.97
- Best CH. Preparation of heparin and its use in the first clinical cases. Circulation. 1959;19(1):79-86. — doi:10.1161/01.CIR.19.1.79
- Heparin, the miracle drug: a brief history of its discovery. Journal of Laboratory and Clinical Medicine / historical review. — Search PubMed
- Jay McLean and the discovery of heparin — historical accounts PubMed: McLean, Howell and the discovery of heparin
- Phlegmasia alba dolens — history and “milk leg” PubMed: phlegmasia alba dolens history
- Rudolf Virchow — thrombosis, embolism, and venous thromboembolism PubMed: Virchow thrombosis and embolism
- Karl Paul Link, sweet clover disease, dicoumarol and warfarin PubMed: Link, sweet clover, dicoumarol and warfarin
- D-dimer in the diagnosis of venous thromboembolism PubMed: D-dimer for VTE diagnosis
- Compression ultrasonography vs venography for deep vein thrombosis PubMed: compression ultrasound vs venography for DVT
External Authoritative Resources
- StatPearls — Virchow Triad (NCBI Bookshelf)
- CDC — Blood Clots (Venous Thromboembolism)
- PubMed — History of DVT and anticoagulation
Connections
- Hematology
- Deep Vein Thrombosis (main article)
- Pulmonary Embolism
- Hemophilia
- Polycythemia Vera
- Von Willebrand Disease
- Disseminated Intravascular Coagulation
- Thrombocytopenia
- All Conditions