Borrelia burgdorferi: Lyme Disease — Tick Bites, Bull's-Eye Rash, and Chronic Symptoms
Symptoms Overview
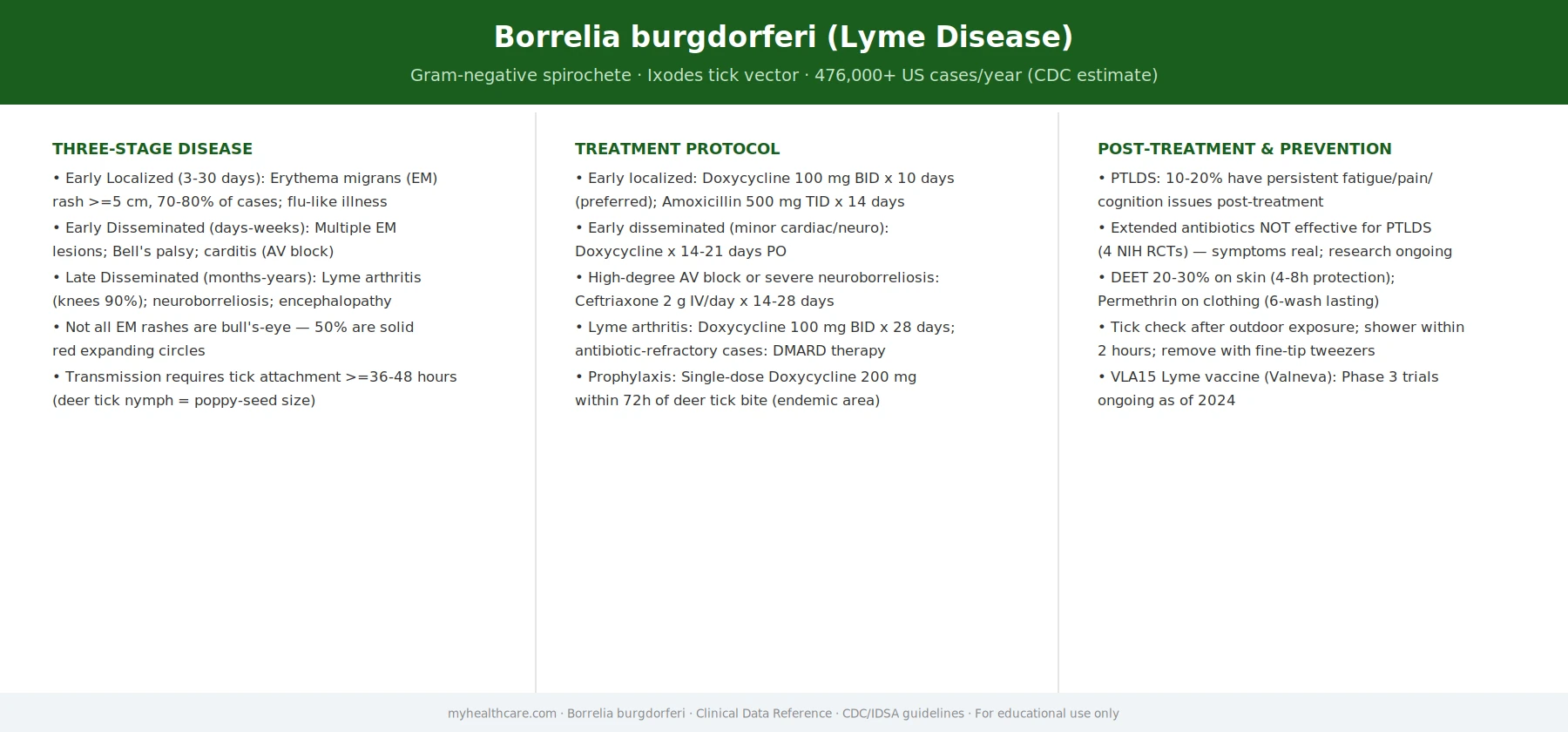
Three-stage Lyme disease: early localized, early disseminated, and late chronic manifestations.
Early Lyme & Erythema Migrans
The bull's-eye rash, flu-like illness, and early dissemination signs.
Late Lyme, Neuroborreliosis & Arthritis
Lyme arthritis, Bell's palsy, Lyme carditis, and neuroborreliosis complications.
Diagnosis & Controversies
Two-tier ELISA/Western blot testing, its limitations, and the "chronic Lyme" debate.
Treatments Overview
Antibiotic protocols, tick removal, and post-treatment symptom management.
Antibiotic Treatment
Doxycycline, amoxicillin, cefuroxime protocols by stage and manifestation.
Tick Prevention
Personal protective measures, repellents, tick checks, landscaping, and vaccine prospects.
Post-Treatment Lyme Disease Syndrome
PTLDS: persistent symptoms after treatment, evidence base, and management strategies.
Lyme disease, caused by the bacterium Borrelia burgdorferi and spread by Ixodes (deer) ticks, is the most common vector-borne disease in the United States — with over 476,000 cases estimated each year by the CDC, a figure that includes the large number of cases that go undiagnosed or unreported. Most people who are treated promptly do very well: a short course of doxycycline started early clears the infection in the great majority of cases. Delayed diagnosis, however, can allow the bacterium to spread through the bloodstream and seed the joints, heart, and nervous system, sometimes causing problems that take months to resolve. A subset of patients experience persistent symptoms after treatment — a condition often called "long Lyme" or Post-Treatment Lyme Disease Syndrome (PTLDS) — whose cause is genuinely contested in the medical literature but whose reality as a patient experience is not.
Table of Contents
- What Borrelia burgdorferi Is
- The Deer Tick Life Cycle
- The Bull's-Eye Rash — and When It's Absent
- Early Localized, Early Disseminated, and Late Lyme
- Lyme Carditis and Neurological Lyme
- Diagnosis: Two-Tier Serology and Its Limitations
- Treatment: Doxycycline, Amoxicillin, and Ceftriaxone
- Post-Treatment Lyme Disease Syndrome
- Research Papers
- Connections
- Featured Videos
What Borrelia burgdorferi Is
Borrelia burgdorferi is a spiral-shaped bacterium (a spirochete) belonging to the same bacterial class as the agents of syphilis and leptospirosis. It was first isolated in 1982 by researcher Willy Burgdorfer, who identified it in the midguts of Ixodes scapularis ticks — earning it his surname. The bacterium is uniquely adapted to life inside ticks and in the bodies of mammalian hosts: it cycles naturally between reservoir animals (mainly white-footed mice and certain other small mammals) and the hard-bodied black-legged ticks that feed on them.
What makes B. burgdorferi unusual is its minimal genome — it carries almost no genes for making its own nutrients and depends almost entirely on its host. It also has an unusually large number of surface proteins (called outer-surface proteins, or Osps) that it switches between as it moves from tick to host, helping it evade immune detection in both environments. OspA is dominant in the tick gut; OspC appears as the bacterium migrates to the tick's salivary glands and is injected into the host — a biological shift that takes time, which is why prompt tick removal prevents most infections.
The Deer Tick Life Cycle
Understanding how Lyme disease spreads means understanding the two-year life cycle of the black-legged tick (Ixodes scapularis in the eastern and central US; Ixodes pacificus on the West Coast).
Tick eggs hatch in spring as tiny, six-legged larvae. These larvae are not yet infected; they pick up B. burgdorferi when they take their first blood meal, almost always from a white-footed mouse (Peromyscus leucopus), which is an excellent reservoir host that carries the bacterium without becoming ill. After feeding, larvae molt into eight-legged nymphs the following spring. Nymphs are responsible for the majority of human Lyme disease cases — they are poppy-seed sized and therefore very easy to miss on skin, and they peak in late spring and early summer when people spend the most time outdoors. After feeding on a second host (which may be a deer, a dog, or a human), nymphs molt into adults. Adult female ticks are more visible but are less often the cause of transmission because they feed mainly in fall and early winter when people wear more protective clothing.
A crucial practical fact: the tick must be attached and feeding for roughly 36 to 48 hours before it transmits enough spirochetes to cause infection. This is why daily tick checks and prompt removal remain the single most effective preventive measure.
The Bull's-Eye Rash — and When It's Absent
The textbook sign of early Lyme disease is erythema migrans (EM) — a slowly expanding red rash that appears at the site of the tick bite, usually within 3 to 30 days. The rash is at least 5 cm (about 2 inches) in diameter at its widest and expands over days to weeks. In some cases it develops central clearing, producing the classic "bull's-eye" or target pattern, but this is actually less common than a uniformly red, expanding oval. The rash is usually not painful or itchy, but the surrounding skin may feel warm.
EM is highly specific for Lyme disease — if a patient who lives in or has traveled through a Lyme-endemic region develops a classic expanding rash, clinical diagnosis is appropriate and treatment should begin without waiting for lab confirmation. However, there are several important caveats:
- Only 70–80% of patients with Lyme disease recall a rash at all. Many tick bites go unnoticed (especially nymph bites in skin folds, the scalp, or behind the knees), and the rash may occur in places the patient cannot easily see.
- The rash may be hidden by dark skin tone, where it presents as a darkening or discoloration rather than redness.
- A much smaller, non-expanding red bump at the site of a tick bite is normal and represents a local hypersensitivity reaction — it is not erythema migrans and does not indicate Lyme disease.
- Other symptoms early in infection may include fatigue, muscle aches, joint pain, headache, fever, and chills — a flu-like illness that is easy to attribute to other causes, especially if no rash is noticed.
Early Localized, Early Disseminated, and Late Lyme
Physicians traditionally divide Lyme disease into three overlapping stages that reflect where the bacterium has spread in the body. These stages are not strict; some patients move through them quickly while others never progress beyond the first.
Early localized Lyme disease (days to weeks after the tick bite) is characterized by the erythema migrans rash at the bite site, with or without mild flu-like symptoms. At this stage the infection is confined to the skin and the bacterium has not yet spread through the bloodstream. Oral antibiotics taken for 10 to 21 days are almost always curative.
Early disseminated Lyme disease (weeks to months after infection) occurs when B. burgdorferi enters the bloodstream and spreads. Signs include multiple erythema migrans lesions in different body areas (secondary rashes away from the original bite), Lyme carditis (see next section), neurological symptoms (facial palsy, meningitis, radiculopathy), and migratory joint aches. If the original infection was missed, this may be when patients first seek care.
Late Lyme disease (months to years after infection, if untreated) most commonly presents as Lyme arthritis — intermittent or persistent swelling of one or a few large joints, most often the knee, without much warmth or redness. The swelling can be dramatic, with the knee ballooning up with fluid. This stage is the most common form of late Lyme in the US and is highly treatable with oral or intravenous antibiotics, though a small minority of patients develop antibiotic-refractory arthritis driven by post-infectious immune activity that may persist even after the bacteria are cleared.
Lyme Carditis and Neurological Lyme
Lyme carditis occurs in roughly 1 in 100 patients with untreated Lyme disease. The bacterium infects cardiac tissue and interferes with the electrical conduction system of the heart, most often causing atrioventricular (AV) block — a slowing or interruption of the electrical signal between the upper and lower chambers. Most cases are mild and temporary, resolving with antibiotics alone. However, high-degree AV block can be severe enough to require temporary cardiac pacing while antibiotics take effect. Symptoms may include palpitations, dizziness, light-headedness, shortness of breath, fainting, or chest pain. Lyme carditis has been identified as a cause of sudden cardiac death in a small number of cases, which is why it warrants prompt diagnosis and treatment.
Neurological Lyme disease (Lyme neuroborreliosis) can involve the peripheral or central nervous system. The most common peripheral manifestation in the US is unilateral or bilateral facial palsy (Lyme-related Bell's palsy) — a drooping or weakness of one side of the face. Other peripheral findings include a painful inflammation of the nerve roots (radiculopathy), causing shooting pain, numbness, or weakness in the arms, legs, or trunk. Central nervous system involvement (Lyme meningitis, encephalopathy) is less common in North America than in Europe but can include confusion, memory and concentration difficulties, and brain inflammation. Most neurological manifestations respond well to antibiotics, though recovery from some nerve injury may take weeks to months.
Diagnosis: Two-Tier Serology and Its Limitations
Diagnosing Lyme disease is straightforward when a patient presents with a classic expanding rash in an endemic area — testing is not needed and treatment should begin right away. In all other situations, or when a patient presents with vague symptoms and no recalled rash, laboratory testing becomes necessary. The standard approach recommended by the CDC is two-tier serological testing:
- First tier: ELISA (enzyme-linked immunosorbent assay). This test measures antibodies (IgM and IgG) to B. burgdorferi proteins. It is sensitive — it catches most true cases — but not specific, meaning it can produce false positives in people with other infections (such as viral illnesses, autoimmune conditions, or tick-borne co-infections like babesiosis or anaplasmosis).
- Second tier: Western blot. Only performed if the ELISA is positive or borderline. The Western blot identifies antibodies to specific individual proteins of the bacterium, and requires a defined number of bands to be positive to count as confirmatory. This two-step system dramatically reduces false positives compared to either test alone.
Critical limitations:
- Serology is negative in the first few weeks of infection. Antibodies take 2 to 6 weeks to develop after a tick bite. A patient tested in the first week with a bull's-eye rash will likely test negative — the rash is the diagnosis, not the antibody test.
- Antibodies can persist for years after successful treatment, so a positive test does not prove active infection. It means the patient was infected at some point; it cannot confirm whether they still are.
- Antibodies do not develop normally in patients treated very early. Those who receive antibiotics in the first days after infection may not mount a full antibody response and can test negative even though they did have early Lyme.
- PCR testing (detecting bacterial DNA) is available and useful for diagnosing Lyme arthritis from joint fluid, but is unreliable in blood and not routinely recommended for other presentations.
These limitations mean that Lyme disease remains a clinical diagnosis in many situations, interpreted in context with the patient's symptoms, exposure history, and geographic location.
Treatment: Doxycycline, Amoxicillin, and Ceftriaxone
Lyme disease is highly treatable with antibiotics. The choice of drug, route, and duration depends on the stage of disease and which body system is involved.
Early localized disease (rash alone, no other involvement):
- Doxycycline 100 mg twice daily for 10–21 days is the preferred first-line option in adults and children over 8 years. It has the additional advantage of also treating co-infections like anaplasmosis, which share the same tick vector. Common side effects include sun sensitivity, nausea, and esophageal irritation (take with a full glass of water and do not lie down immediately after).
- Amoxicillin 500 mg three times daily for 14–21 days is the preferred option in young children, pregnant women, and those who cannot tolerate doxycycline.
- Cefuroxime axetil 500 mg twice daily is an alternative for adults who cannot take either of the above.
Lyme carditis: Mild AV block (first-degree) can be treated with oral antibiotics. Higher-degree AV block warrants hospitalization and intravenous ceftriaxone 2 g daily until the block resolves, at which point patients can be switched to oral antibiotics to complete 14–21 days of total treatment.
Neurological Lyme (meningitis, radiculopathy, encephalitis): Intravenous ceftriaxone for 14–28 days is standard. Facial palsy alone (without meningitis) can be treated with oral doxycycline.
Lyme arthritis: Oral doxycycline or amoxicillin for 28 days. If arthritis does not respond, a second 28-day oral course or a 14–28 day course of intravenous ceftriaxone may be used. Antibiotic-refractory arthritis that persists after two courses may require anti-inflammatory treatment (NSAIDs, hydroxychloroquine) as the driver is post-infectious immune activity rather than ongoing bacterial infection.
Post-Treatment Lyme Disease Syndrome
A genuinely important and genuinely contested area of Lyme disease medicine involves patients who complete an appropriate course of antibiotic therapy, test positive by serology, and yet continue to experience symptoms for months or longer — most commonly fatigue, musculoskeletal pain, and difficulty with memory and concentration. This is referred to in the medical literature as Post-Treatment Lyme Disease Syndrome (PTLDS), though patients and advocacy communities often call it "chronic Lyme disease" or "long Lyme."
What is well-established:
- PTLDS is real as a clinical phenomenon. Randomized controlled trials have documented that a meaningful minority of treated Lyme patients — estimated at 5–15% in different studies — have lingering symptoms 6 months or more after treatment.
- Multiple large randomized trials have found that prolonged additional antibiotic courses do not improve outcomes in PTLDS and expose patients to significant risks (including serious infections from long intravenous lines, and antibiotic-related complications). Giving more antibiotics to treat PTLDS is not supported by current evidence.
What remains contested:
- Whether lingering symptoms are caused by persistent viable bacteria, persistent non-viable bacterial fragments triggering inflammation, permanent structural damage, an autoimmune process, or a combination of factors.
- Whether PTLDS is pathologically distinct from similar post-infectious syndromes seen after other infections (such as Q fever or glandular fever), or a manifestation of a more general post-infection process.
Current evidence-based guidance is to treat PTLDS supportively — managing symptoms (fatigue, pain, sleep) while avoiding repeated or prolonged antibiotic courses that carry real risks without proven benefit. Research into the mechanism of PTLDS is ongoing and is a priority area for the NIH.
Research Papers
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43(9):1089–1134. doi:10.1086/508667 — The foundational IDSA clinical practice guidelines covering the full spectrum of Lyme disease diagnosis, staging, treatment, and co-infections; sets standards for two-tier serology and antibiotic selection.
- Shapiro ED. Lyme disease. N Engl J Med. 2014;370(18):1724–1731. doi:10.1056/NEJMcp1314325 — A landmark NEJM clinical practice review summarizing the epidemiology, clinical presentations, diagnostic challenges, and treatment evidence for Lyme disease, including a detailed discussion of erythema migrans and serology limitations.
- Klempner MS, Hu LT, Evans J, et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001;345(2):85–92. doi:10.1056/NEJM200107123450202 — Definitive randomized trials showing that prolonged additional antibiotic therapy (90 days) did not improve outcomes in patients with persistent symptoms after treated Lyme disease, shaping current guidelines against extended antibiotic retreatment.
- Nadelman RB, Nowakowski J, Fish D, et al. Prophylaxis with single-dose doxycycline for the prevention of Lyme disease after an Ixodes scapularis tick bite. N Engl J Med. 2001;345(2):79–84. PubMed: 11450675 — Randomized trial establishing that a single 200 mg dose of doxycycline given within 72 hours of a high-risk tick bite reduced the risk of developing Lyme disease by 87%, supporting post-exposure prophylaxis in endemic areas. (DOI not resolved via Crossref; PubMed link provided.)
- Steere AC, Schoen RT, Taylor E. The clinical evolution of Lyme arthritis. Ann Intern Med. 1987;107(5):725–731. PubMed: 3662285 — Classic longitudinal study defining the natural history of Lyme arthritis — intermittent swelling of large joints, predominantly the knee, in untreated Lyme disease — and establishing that antibiotics curtail the arthritic course. (DOI not resolved via Crossref; PubMed link provided.)
Connections
- Lyme Disease (Infectious Disease)
- Arthritis
- Fibromyalgia
- Bell's Palsy
- Peripheral Neuropathy
- Chronic Fatigue Syndrome
- Arrhythmia
- Myocarditis
- Alpha-Gal Syndrome
- Rheumatology Conditions
- Neurology Conditions
- All Conditions