Lyme Disease Prevention — Tick Repellents, Safe Removal, Yard Control, and the Lyme Vaccine
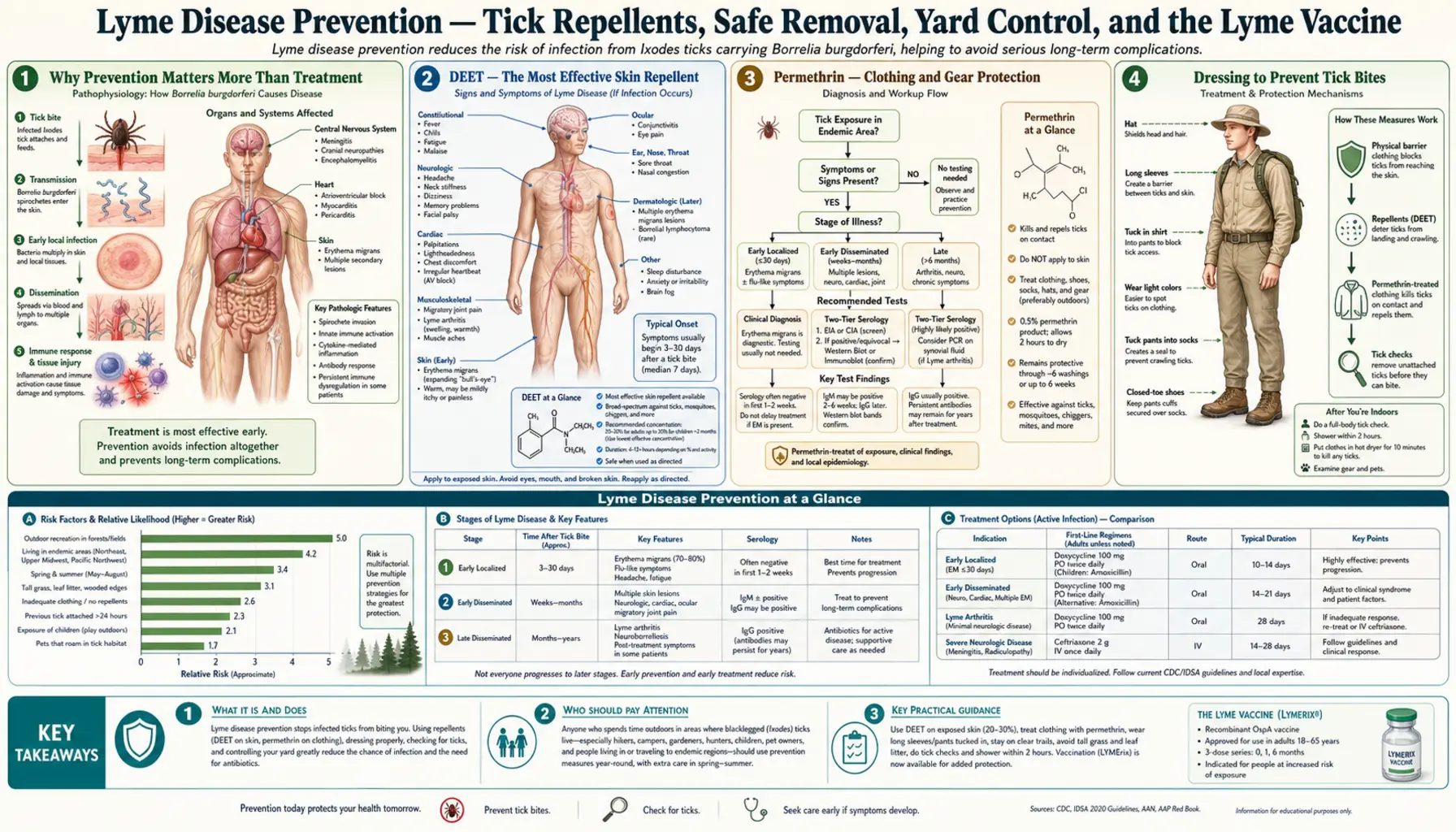
Table of Contents
- Why Prevention Matters More Than Treatment
- DEET — The Most Effective Skin Repellent
- Permethrin — Clothing and Gear Protection
- Dressing to Prevent Tick Bites
- Daily Tick Checks — The Most Important Habit
- Safe Tick Removal Step by Step
- Yard and Landscape Management
- Tick Identification — Know Your Enemy
- The Lyme Vaccine — Past, Present, and Future
- After a Bite — When to See a Doctor
- Research Papers
- Connections
- Featured Videos
Why Prevention Matters More Than Treatment
The most important thing to understand about Lyme disease is that it is largely preventable. While antibiotics are highly effective when the disease is caught early, prevention eliminates the need for treatment entirely and avoids the small but real risk that early symptoms will be missed or misattributed to something else.
A critical biological fact makes prevention unusually tractable for Lyme disease: Borrelia burgdorferi transmission from an infected deer tick to a human requires the tick to be attached and feeding for at least 36 to 48 hours. This is because Borrelia spirochetes live in the tick's midgut and must migrate to the salivary glands — a process that takes roughly two days of feeding to complete. This means that a tick discovered and removed within 24 hours almost never transmits Lyme disease, even if the tick was infected.
This 36–48 hour window transforms prevention from a passive hope into an active strategy: if you can find and remove a tick before that window closes, you are protected. Daily tick checks, combined with repellents and protective clothing to prevent attachment in the first place, reduce your risk by more than 80% in endemic areas. No treatment can offer that level of certainty after the fact.
Prevention is also particularly important because early Lyme disease is easily missed: the EM rash is absent in 20–30% of patients, the early flu-like symptoms are nonspecific, and serological tests are negative in the first 2 weeks of infection. Preventing the bite is more reliable than catching the disease early.
DEET — The Most Effective Skin Repellent
DEET (N,N-diethyl-meta-toluamide) has been the gold-standard tick and insect repellent since its development by the US Army in 1944. Decades of use and extensive safety research support its effectiveness and safety when used as directed.
How it works: DEET interferes with chemoreceptors on arthropod sensory organs (particularly the antennae and palps), disrupting the ability of ticks and insects to detect carbon dioxide, lactic acid, and other chemical signals emitted by human skin. Ticks exposed to DEET-treated skin typically detach and move away rather than biting. DEET does not kill ticks — it repels them.
Concentration guide: The concentration of DEET affects how long the product remains effective, not how intensely it works. Higher concentrations are not more repellent — they provide longer duration of protection:
- 10% DEET: approximately 2 hours of protection
- 20–30% DEET: 4–8 hours of protection (the recommended range for tick exposure)
- 50% DEET: up to 12 hours but no stronger repellent effect than 30%; not necessary for most situations
- 100% DEET: no additional benefit for most users; reserved for extreme exposure conditions
Application: Apply DEET to all exposed skin surfaces, avoiding eyes, mouth, and open cuts. Do not apply under clothing (it has no protective effect there and can cause skin irritation under occlusion). Apply before going outdoors; reapply after swimming, heavy sweating, or when protection duration expires. DEET is safe for use on children 2 months of age and older; products formulated for children typically contain 10–20% concentrations. Avoid applying DEET to an infant's hands, as infants put their hands in their mouths. Wash DEET off with soap and water when returning indoors.
Safety profile: DEET is one of the most extensively tested chemicals used on human skin. It is considered safe when used as directed. Rare skin irritation occurs in some individuals, particularly with repeated application to the same area. Neurological toxicity (seizures, encephalopathy) has been reported only with extreme overexposure — ingestion or application of large quantities to broken skin. There is no evidence of cancer risk or systemic harm from normal use. The risk-benefit calculation overwhelmingly favors using DEET in Lyme-endemic areas during tick season.
Alternatives: Picaridin (20%) and IR3535 (20%) are effective alternatives with somewhat different odor profiles. Oil of lemon eucalyptus (OLE) and its active synthetic analog PMD (para-menthane-3,8-diol) provide reasonable protection and are acceptable for adults and children over 3 years. "Natural" repellents based on essential oils (citronella, lavender, tea tree) have poor evidence for tick repellency and are not recommended as primary protection in Lyme-endemic areas.
Permethrin — Clothing and Gear Protection
Permethrin is a synthetic pyrethroid insecticide that, when applied to clothing and gear rather than skin, provides a layer of tick protection that is fundamentally different from DEET. It does not repel ticks — it kills them on contact.
Mechanism: Permethrin works by disrupting sodium channel function in insect and arachnid nerve cells, causing prolonged nerve depolarization, paralysis, and death. A tick walking across permethrin-treated fabric typically shows excitation and then knockdown within seconds of contact. This contact-kill effect means ticks are incapacitated or killed before they can crawl to exposed skin to bite.
Application to clothing: Permethrin should be sprayed onto clothing and allowed to dry completely (several hours in well-ventilated conditions) before wearing. Once dried and bound to fabric, permethrin is odorless, invisible, and resistant to washing — studies show effective protection persisting through 6 or more washes. Products labeled for clothing treatment should be used at the concentrations specified (typically 0.5% permethrin for consumer products).
Target items: Socks and shoes are the highest priority, as most tick encounters begin at ground level with nymph ticks crawling up from leaf litter. Pants, shirts, hats, and backpacks also benefit significantly. Commercially pre-treated clothing (Insect Shield, ExOfficio, L.L.Bean) is available in a range of outdoor gear and provides protection rated for 70 or more washes, making it more durable than home application.
Critical safety rule: Permethrin is NOT for application to skin. When applied to skin, it is rapidly metabolized by cutaneous enzymes and loses its effectiveness within minutes. It can also cause skin irritation in higher concentrations. Permethrin is for fabric only.
Combined strategy: The combination of DEET on skin and permethrin on clothing provides the highest available level of personal tick protection. Studies from the US military found that this combination reduced tick bites to near zero in highly endemic environments.
Dressing to Prevent Tick Bites
Clothing choices can substantially reduce tick exposure by creating physical barriers that prevent ticks from reaching skin. While not a substitute for repellents, proper clothing dramatically improves the effectiveness of other prevention measures and makes tick checks more productive.
Long pants: Wear full-length trousers when walking through grass, brush, or wooded areas. Tuck pants into socks at the ankle — this is the single most effective clothing maneuver because it blocks the primary entry route of nymph ticks (which are tiny, poppy-seed-sized, and crawl upward from the ground). The appearance may be unfashionable but the protection is real.
Long-sleeved shirts: Reduces exposed arm and torso skin surface available for tick attachment. Tuck shirt into pants.
Light-colored clothing: Ticks are dark brown to black, making them far easier to spot on light-colored clothing before they reach skin. This simple choice makes tick checks more effective during the day.
Closed-toe shoes: Sandals leave the feet and ankles exposed. Closed shoes with socks create a much better surface for permethrin application and prevent direct tick contact with skin.
Path discipline: When possible, walk in the center of trails — ticks perch on the tips of grass blades and leaf edges at the trail margins and transfer to passing hosts by a behavior called questing (holding onto vegetation with rear legs while extending front legs). Avoiding the brushy margins significantly reduces contact.
Post-exposure clothing management: Change out of outdoor clothes promptly after returning indoors. Place clothes in a dryer on high heat for 10 minutes before washing — heat kills ticks faster than washing alone (ticks can survive a cold-water wash cycle but not heat). Shower within 2 hours of returning from tick habitat; a shower does not eliminate attached ticks but can wash off unattached nymphs that have not yet found a bite site.
Daily Tick Checks — The Most Important Habit
Given the 36–48 hour transmission window, systematic tick checks performed every day after potential outdoor exposure in endemic areas are one of the highest-yield prevention behaviors available. A tick found and removed within 24 hours is almost certainly harmless, regardless of whether it was infected.
When to check: After any time outdoors in or near wooded areas, tall grass, gardens, or leaf piles during tick season (peak activity: May through July for nymphs; fall for adult deer ticks, which are also active on warm winter days). Check before showering — warm running water can dislodge ticks, but checking first allows you to find and remove them properly.
Where to look — priority areas: Deer tick nymphs are small enough to hide in inconspicuous locations. Systematic checking of these areas is essential:
- Scalp — run fingers through hair systematically; use a fine-tooth comb on thick hair
- Behind the ears and in the ear canal
- Neck and hairline at the nape
- Armpits
- Groin and around the waist (where waistbands contact skin)
- Behind the knees
- Between the toes and around the ankles
- In the navel (belly button)
Technique: Use a hand-held mirror for the back of the neck, back, and posterior legs. Use a full-length mirror for overall inspection. A second person checking the scalp and back is ideal. Feel for small bumps that weren't there before — nymph ticks are the size of poppy seeds and can be mistaken for freckles or dirt.
Checking children and pets: Children playing outdoors in endemic areas should be checked daily, paying particular attention to the scalp. Dogs and cats can bring ticks indoors and serve as tick transport vehicles; check pets regularly and use veterinarian-recommended tick prevention products. Pets can also develop Lyme disease themselves.
Safe Tick Removal Step by Step
Prompt, correct tick removal is critical. Incorrect techniques — including popular folklore approaches — can increase transmission risk by causing the tick to regurgitate midgut contents into the bite site.
What you need: Fine-tipped pointed tweezers (the pointed tip is important for grasping the mouthparts close to the skin without crushing the tick body). Standard household tweezers with broad, flat tips are not ideal.
Step-by-step removal:
- Grasp the tick with tweezers as close to the skin surface as possible — ideally gripping the mouthparts (capitulum) where they enter the skin, not the body of the tick.
- Pull upward with steady, even pressure — do not twist, jerk, or wiggle. Twisting can cause the mouthparts to break off and remain in the skin.
- If mouthparts break off and remain in the skin, leave them alone — they will eventually be expelled naturally. Digging for them with a needle creates more tissue trauma than letting them come out on their own.
- After removal, clean the bite site thoroughly with rubbing alcohol, iodine scrub, or soap and water.
- Dispose of the tick: place it in a sealed plastic bag, submerse it in alcohol, or flush it down the toilet. Do not crush it with your fingers (the hemolymph is infectious).
What NOT to do: Do not apply petroleum jelly (Vaseline), nail polish remover, gasoline, lighter fluid, or heat from a match or cigarette to the tick. These methods are based on the idea of "forcing" the tick to detach, but ticks do not respond this way — they simply die in place. Worse, these techniques can cause the tick to regurgitate its gut contents, potentially increasing transmission risk. They are also associated with burns and skin damage.
After removal — monitoring: Mark the calendar with the date of removal. Watch the bite site for 30 days. The two things to watch for: (1) an expanding red rash at or around the bite site (EM rash — note that a small red bump immediately after removal is normal and is a local skin reaction, not Lyme; Lyme rash typically expands over 3–30 days); (2) systemic symptoms within 30 days — fever, chills, fatigue, joint or muscle aches, headache. Seek medical attention promptly if either develops.
Yard and Landscape Management
For households in Lyme-endemic areas, environmental management of the yard can substantially reduce tick populations and the risk of tick exposure during everyday outdoor activities — gardening, playing, and walking the dog near home.
Habitat modification: Deer ticks require humid, shaded conditions to survive — they desiccate and die rapidly in warm, sunny, dry environments. Landscaping choices that eliminate favorable tick habitat can reduce tick densities by 50–80%:
- Clear leaf litter from lawn areas, especially at property margins bordering woods or brush — this eliminates the cool, moist layer where ticks and their hosts (mice, voles) live
- Mow lawns regularly and keep grass short
- Trim shrubs and overhanging branches to increase sun exposure and air circulation in yard areas
- Remove woodpiles near the house (they harbor mice that are primary tick hosts)
- Create a 3-foot wide barrier of wood chips, gravel, or mulch between the lawn and any adjacent wooded areas — ticks rarely cross dry, sun-exposed barriers, and this perimeter provides a visual reminder of the risk zone
Playground and furniture placement: Place children's play equipment, decks, and patio furniture in sunny, central lawn areas away from tree lines and brush borders. Ticks are significantly less abundant in open, dry, sunny areas.
Deer management: White-tailed deer are the primary reproductive host for adult deer ticks (larvae and nymphs feed on small mammals, especially white-footed mice, but adults feed on deer). Deer fencing (8-foot height is effective; 4-foot fencing is insufficient) dramatically reduces deer tick populations in enclosed areas. This option is expensive and practical only for smaller properties.
Tick tubes: Permethrin-impregnated cotton balls placed in cardboard tubes are distributed around the yard. Mice, which are primary hosts for larval and nymphal ticks, take the cotton for nesting material; permethrin on the cotton kills ticks feeding on the mice. Studies in suburban northeastern US settings show tick tube programs reduce tick populations by 50–90% when applied in spring and early fall. This approach targets the white-footed mouse reservoir directly.
Acaricide (tick pesticide) spraying: Professional application of bifenthrin or cyfluthrin to wooded margins and ornamental plantings in spring and fall can reduce tick populations by 70–90% on treated properties. This approach is effective but uses pesticides; choose licensed professionals who apply targeted, minimal-coverage treatments. Timing in May (before peak nymph activity) and September (before adult activity) provides the best coverage.
Tick Identification — Know Your Enemy
Not all ticks transmit Lyme disease. Correctly identifying the tick species found on your skin or clothing can help guide decisions about medical evaluation and prophylaxis.
Ixodes scapularis (black-legged tick / deer tick) — the Lyme disease vector in the northeastern, mid-Atlantic, and upper midwestern United States:
- Adults: 1.5–2 mm unfed (sesame seed size); reddish-orange body with black legs and a black "scutum" (shield-shaped plate on the back); engorged females expand to 10 mm
- Nymphs: 1–1.5 mm unfed (poppy seed size); translucent to pale brown; easily overlooked on skin
- Larvae: under 1 mm; 6 legs; rarely involved in transmission (not yet fed on infected reservoir)
- Geographic range: primarily eastern US from Maine to Florida, upper midwest including Minnesota and Wisconsin; range expanding
Ixodes pacificus (western black-legged tick) — the Lyme vector on the Pacific Coast (California, Oregon, Washington); similar in appearance to I. scapularis but infection prevalence in ticks is lower.
Ticks that do NOT transmit Lyme disease:
- Dermacentor variabilis (American dog tick): larger than deer ticks; ornate patterned white and brown scutum; no Lyme transmission but can transmit Rocky Mountain spotted fever and tularemia
- Amblyomma americanum (lone star tick): distinctive white spot on female; transmits ehrlichiosis, anaplasmosis, and alpha-gal syndrome but NOT Lyme disease
- Rhipicephalus sanguineus (brown dog tick): found in kennels and homes; transmits Rocky Mountain spotted fever in some areas but not Lyme
If you are uncertain about tick identification, many state health departments and university extension programs offer tick identification services. The TickSpotters program run by the University of Rhode Island provides free photographic tick identification online.
The Lyme Vaccine — Past, Present, and Future
A vaccine against Lyme disease is one of the most anticipated developments in infectious disease prevention. The story of the first vaccine, its withdrawal, and the current development pipeline is important for patients in endemic areas to understand.
LYMErix — the first generation (1998–2002): SmithKline Beecham's LYMErix was FDA-approved in December 1998 for adults aged 15–70 in endemic areas. It targeted OspA (outer surface protein A), a lipoprotein expressed on Borrelia burgdorferi's surface when in the tick midgut. The vaccine stimulated antibody production against OspA; when an infected tick began feeding on a vaccinated person, the person's anti-OspA antibodies were taken up with the tick's blood meal and killed the spirochetes in the tick's gut before they could migrate to the salivary glands and be transmitted. Efficacy in phase 3 trials: 76% after three doses in adults.
LYMErix was voluntarily withdrawn from the market in February 2002 — not because of a regulatory safety finding, but due to dramatically low sales, driven in part by a class action lawsuit alleging the vaccine caused treatment-resistant Lyme arthritis in genetically susceptible individuals (through molecular mimicry between OspA and a human protein). Independent scientific review and a subsequent FDA advisory committee review found no causal evidence for this claim. The vaccine's withdrawal left a preventable endemic disease without a preventive option for over two decades.
VLA15 / mRNALYME — the next generation: Valneva and Pfizer co-developed VLA15, a recombinant subunit vaccine targeting OspA from all six clinically relevant Borrelia genospecies (including B. burgdorferi in the US and B. afzelii, B. garinii in Europe). The VALOR Phase 3 trial, enrolling approximately 6,000 participants at high risk for Lyme exposure in the US and Europe, reported results in 2023: VLA15 (now called Lyme vaccine, or VAXELIS in some protocols) demonstrated approximately 89% efficacy against physician-confirmed Lyme disease and 85% efficacy against confirmed symptomatic infections. The vaccine appeared well tolerated; the most common adverse events were injection site reactions and mild systemic symptoms. Annual boosting is likely needed given the seasonal expression of OspA and geographic strain variation. The vaccine was submitted for FDA approval with a decision anticipated in 2025–2026.
Separately, Moderna has disclosed development of an mRNA-based Lyme vaccine; preclinical data suggest strong immune responses, with human trials planned.
After a Bite — When to See a Doctor
Most tick bites, even from deer ticks in endemic areas, do not transmit Lyme disease. However, the steps you take in the 72 hours after removing a tick can meaningfully reduce your risk — and recognizing the symptoms that warrant prompt medical evaluation can catch the disease at its most treatable stage.
Immediately after removal: Remove the tick as described above. Clean the bite site. Note the date. If possible, save the tick in a sealed container or photograph it for identification. Do not wait for symptoms to develop before taking this step.
Post-exposure prophylaxis (PEP) window — 72 hours: If the tick is identified as a deer tick (Ixodes scapularis), was attached for at least 36 hours, and the bite occurred in a Lyme-endemic area, a single 200 mg dose of doxycycline within 72 hours of removal provides approximately 87% protection against developing Lyme disease. Discuss this option with your doctor or an urgent care clinician — this is a time-sensitive decision. If doxycycline is contraindicated (pregnancy, age under 8), seek evaluation promptly to discuss alternative monitoring strategies.
Symptoms to watch for — 30 days:
- EM rash: An expanding red rash around or near the bite site, growing larger over days to weeks. The classic "bull's-eye" (central clearing) is actually present in only a minority of cases; most EM rashes are uniformly red and expanding. Any new expanding rash near a recent bite should be evaluated by a physician same-day. Do not wait for a bull's-eye appearance that may never develop.
- Flu-like illness: Fever, chills, fatigue, muscle aches, headache, or joint pain within 30 days of a tick bite should prompt medical evaluation, even without a visible rash.
- Cardiac or neurological symptoms: Palpitations, shortness of breath, facial drooping, or severe headache warrant urgent evaluation.
Testing in the first two weeks: Standard ELISA serology for Lyme disease is unreliable in the first 2 weeks of infection — the antibody response has not yet mounted. A negative test in the first 2 weeks after a bite does NOT rule out Lyme disease in a patient with an EM rash. Clinical diagnosis of EM rash in an appropriate epidemiological context is sufficient to start treatment without waiting for test confirmation.
Research Papers
- Search PubMed — Eisen RJ & Eisen L. The blacklegged tick, Ixodes scapularis: an increasing public health concern. Trends Parasitol. 2018.
- Search PubMed — Skar GL & Simonsen KA. Lyme Disease. StatPearls. 2023.
- Search PubMed — Hu LT. Lyme Disease. Ann Intern Med. 2016.
- Search PubMed — Lantos PM et al. Empiric antibiotic treatment of erythema migrans-like skin lesions as a function of geography. Vector Borne Zoonotic Dis. 2013.
- Search PubMed — Wormser GP et al. The clinical assessment, treatment, and prevention of lyme disease: IDSA clinical practice guidelines. Clin Infect Dis. 2006.
- Search PubMed — Steere AC et al. Lyme borreliosis. Nat Rev Dis Primers. 2016.
- Search PubMed — Berende A et al. Randomized trial of longer-term therapy for symptoms attributed to Lyme disease. N Engl J Med. 2016.
- Search PubMed — Shapiro ED. Lyme Disease. N Engl J Med. 2014.
- Search PubMed — Piesman J & Eisen L. Prevention of tick-borne diseases. Annu Rev Entomol. 2008.
- Search PubMed — Nadelman RB et al. Prophylaxis with single-dose doxycycline for the prevention of Lyme disease after an Ixodes scapularis tick bite. N Engl J Med. 2001.
Connections
- Lyme Disease Treatments Hub
- Antibiotic Treatment Protocols
- Post-Treatment Lyme Disease Syndrome
- Lyme Disease Symptoms Hub
- Early Lyme & EM Rash
- Borrelia burgdorferi Main Page
- Alpha-Gal Syndrome
- All Bacteria
- Lyme Disease — the main Lyme disease page covering stages, diagnosis, and treatment.