Late Lyme Disease — Neuroborreliosis, Arthritis, and Chronic Manifestations
- What Is Late Lyme Disease?
- Lyme Arthritis — Symptoms and Mechanism
- Antibiotic-Refractory Lyme Arthritis
- Lyme Neuroborreliosis — Overview
- Peripheral Neuropathy and Radiculopathy
- Encephalopathy — Cognitive and Memory Problems
- Lyme Carditis in Late Disease
- Ocular Lyme Disease
- Acrodermatitis Chronica Atrophicans (European Lyme)
- Pediatric Late Lyme Disease
- Untreated Lyme — What Happens Over Time
- Research Papers
- Connections
- Featured Videos
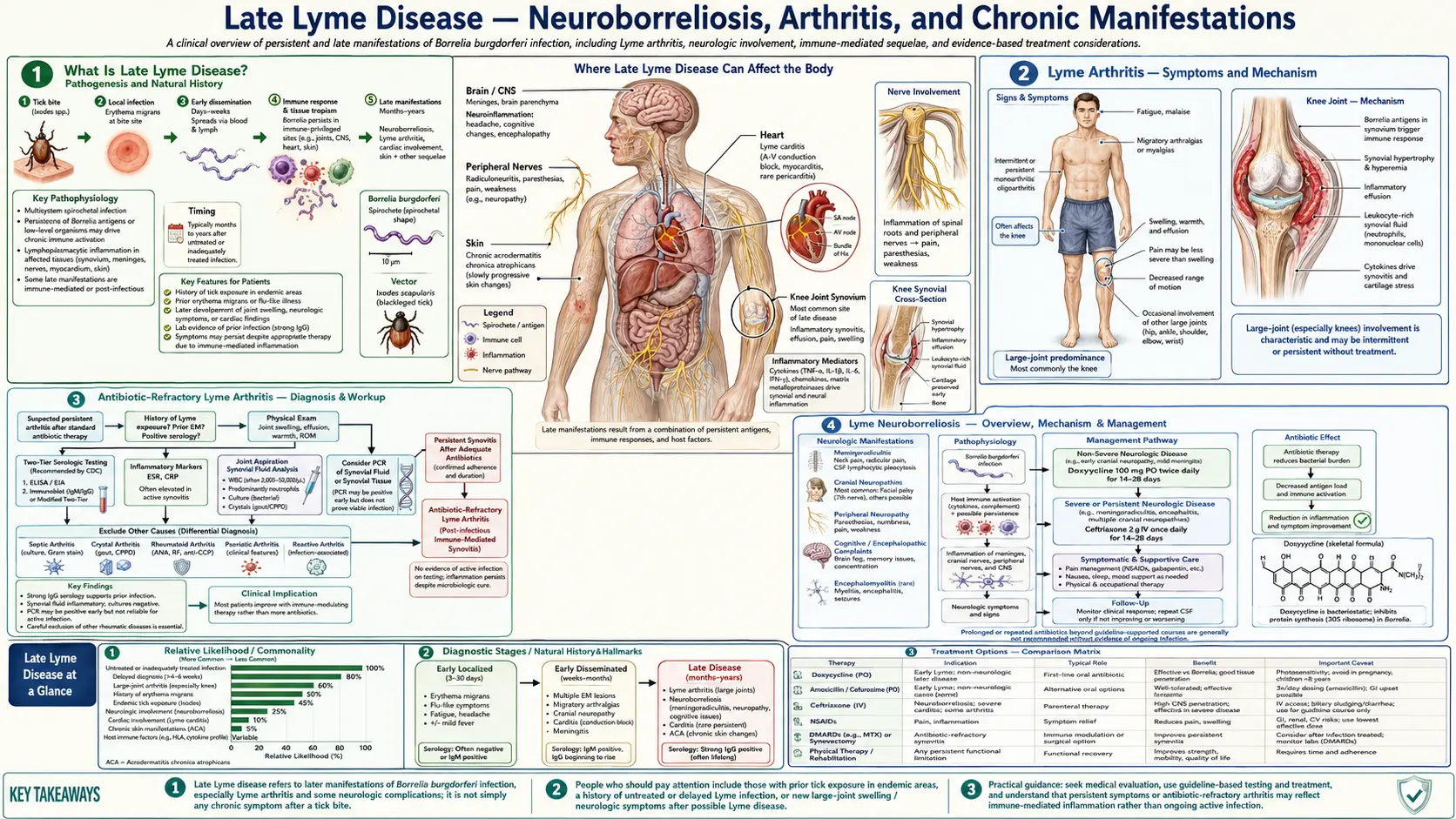
What Is Late Lyme Disease?
Late Lyme disease develops months to years after an untreated or inadequately treated initial infection with Borrelia burgdorferi. It represents the third and most serious stage of the infection, following early localized disease (the expanding rash) and early disseminated disease (spread to other organs). Not all patients progress through all stages — and treatment at any stage generally halts further progression.
In the United States, late Lyme disease most commonly presents as Lyme arthritis, accounting for roughly 80% of late-stage cases. In Europe, the picture differs because Borrelia afzelii predominates over B. burgdorferi sensu stricto, making acrodermatitis chronica atrophicans (a chronic skin condition) and certain neurological syndromes more prominent late manifestations.
The key clinical point is that late Lyme disease is not inevitable. Early antibiotic treatment is highly effective. Understanding what happens when infection is missed or inadequately treated is important both for clinicians managing complex cases and for patients trying to understand their own symptoms.
Lyme Arthritis — Symptoms and Mechanism
Lyme arthritis is the most common late manifestation of Lyme disease in North America, affecting approximately 60% of untreated patients. It classically presents as intermittent attacks of joint swelling and pain, which over time can become persistent. The knee is involved in roughly 90% of cases — often dramatically, with large effusions (fluid collections) that can reach several hundred milliliters. The swelling is typically out of proportion to the pain, which distinguishes it from many other arthritides.
Other large joints — shoulders, elbows, ankles, hips — can also be affected, but small joint involvement (fingers, wrists) is much less typical than in rheumatoid arthritis. The episodic nature early on — weeks of swelling followed by full remission — is characteristic. Over months without treatment, attacks may become more frequent and prolonged, eventually becoming continuous.
Mechanism: B. burgdorferi surface lipoproteins — particularly outer surface protein A (OspA) — bind to synovial tissue. This triggers a robust inflammatory cascade involving pro-inflammatory cytokines (TNF-α, IL-6, IL-17), macrophage activation, neutrophil recruitment, and villous hypertrophy of the synovial membrane. Synovial biopsy shows plasma cells, macrophages, and prominent vascular changes — a picture that can closely resemble early rheumatoid arthritis or reactive arthritis.
Diagnosis confirmation: PCR on synovial fluid (not blood) is the most sensitive test in active Lyme arthritis, with sensitivity in the 70–85% range. Two-tier serology (ELISA + Western blot) is nearly always positive at this stage since patients have had months to mount an antibody response. Distinguishing features from rheumatoid arthritis include: usually monoarticular or oligoarticular, episodic early course, asymmetric, responds to antibiotics in most cases, and absence of rheumatoid factor or anti-CCP antibodies.
Antibiotic-Refractory Lyme Arthritis
Approximately 10–15% of patients with Lyme arthritis do not respond to two courses of appropriate antibiotics (typically oral doxycycline followed by IV ceftriaxone). This is termed antibiotic-refractory Lyme arthritis. Importantly, it does not mean the bacteria are still present — PCR of synovial fluid in these patients is negative, confirming bacterial clearance. What persists is sterile inflammation driven by immune mechanisms, not ongoing infection.
The leading explanation is molecular mimicry and autoimmune perpetuation. OspA epitopes on the bacterial surface share structural similarity with LFA-1, a protein expressed on T cells within the synovium. After the bacteria are cleared, a subset of patients with specific HLA-DR4 haplotypes mounts a self-sustaining autoreactive T cell response targeting the joint lining. Additional mechanisms include anti-neural antibodies (particularly anti-ABIN-3) and an excessive Th1 cytokine profile that maintains inflammation even in the absence of viable spirochetes.
Treatment: Antibiotic-refractory Lyme arthritis is treated with anti-inflammatory agents, not more antibiotics. First-line options include hydroxychloroquine, disease-modifying antirheumatic drugs (DMARDs) such as methotrexate, and in some cases synovectomy (surgical removal of inflamed synovial tissue). Continued antibiotic treatment in this setting adds risk (Clostridioides difficile colitis, venous catheter infections for IV therapy) without benefit. The prognosis with appropriate anti-inflammatory treatment is generally good — most patients achieve remission within one to two years.
Lyme Neuroborreliosis — Overview
Neurological involvement in Lyme disease — termed Lyme neuroborreliosis (LNB) — can occur in early disseminated disease (weeks after infection) or, less commonly, as a late manifestation (months to years later). In North America, the most common neurological presentations are facial nerve palsy (Bell's palsy), radiculopathy (painful nerve root inflammation), and lymphocytic meningitis. Roughly 15% of untreated patients develop LNB.
In Europe, B. garinii strain predominates and produces Bannwarth syndrome — a particularly painful meningoradiculitis characterized by excruciating radicular pain often worst at night, lymphocytic CSF pleocytosis, and frequently facial palsy. Bannwarth syndrome is a classic presentation in European neuroborreliosis but relatively unusual in North American disease.
Diagnostic workup: When LNB is suspected, lumbar puncture is essential. CSF findings include lymphocytic pleocytosis (typically 100–300 white cells/µL, predominantly lymphocytes), elevated protein, and normal glucose. Intrathecal antibody production — demonstrating that Borrelia-specific antibodies are being made within the CNS compartment (not just leaking in from blood) — is the most specific diagnostic criterion. This is calculated as the CSF:serum antibody index. Most patients with LNB are seropositive in blood, though rare seronegative cases have been documented.
Treatment: IV ceftriaxone 2 g daily for 14–28 days is standard for CNS Lyme disease. Oral doxycycline achieves adequate CSF penetration and is an acceptable alternative for peripheral neuropathy, radiculopathy, and mild meningitis in patients without significant CNS parenchymal involvement. Most patients improve substantially with treatment, though recovery can take weeks to months.
Peripheral Neuropathy and Radiculopathy
Peripheral nervous system involvement in Lyme disease produces a spectrum of symptoms that can be difficult to distinguish from other neuropathies without serological context. Radiculopathy — inflammation of nerve roots — presents as painful, burning, or shooting sensations that follow dermatomal patterns (bands around the trunk, shooting down an arm or leg). Numbness, tingling, and weakness in the affected distribution are common. Symptoms may be bilateral and asymmetric.
Mononeuropathy multiplex — simultaneous involvement of multiple named peripheral nerves at distinct locations — is a distinctive pattern that can suggest Lyme neuroborreliosis when it occurs in an endemic area. Facial nerve palsy is the most common cranial neuropathy (can be bilateral, which is rare in Bell's palsy from other causes). Other cranial nerves (III, IV, VI — eye movement; VIII — hearing and balance) are occasionally affected.
Electrodiagnostic studies (nerve conduction velocity, EMG) show axonal polyneuropathy in most cases. The clinical picture overlaps with diabetic neuropathy, inflammatory neuropathies, and cervical/lumbar radiculopathy — making Lyme serology critical in the diagnostic workup for patients with these symptoms who live in or have traveled to endemic areas.
Most patients with Lyme radiculopathy and peripheral neuropathy improve significantly with appropriate antibiotic therapy, though recovery may be gradual over weeks to months, reflecting the time needed for nerve regeneration after axonal damage.
Encephalopathy — Cognitive and Memory Problems
Lyme encephalopathy refers to diffuse brain dysfunction occurring during active B. burgdorferi infection, manifesting as subtle but measurable cognitive deficits. Symptoms include impaired memory (particularly verbal memory and recall), word-finding difficulty, slowed processing speed, poor concentration, and difficulty with complex mental tasks. Patients often describe it as "brain fog" — a feeling of mental cloudiness that makes familiar tasks harder than they should be.
These symptoms are real and documentable. Neuropsychological testing in affected patients consistently shows mild but statistically significant deficits in memory and processing speed compared to age-matched controls. Brain MRI may reveal white matter hyperintensities (T2/FLAIR signal changes) in some patients, though this finding is not universal and is not specific to Lyme disease.
Mechanism: Multiple pathways are implicated. B. burgdorferi can directly infect the CNS, and inflammatory cytokines produced in response to infection cross the blood-brain barrier and disrupt neurotransmission and synaptic function. Intrathecal antibody production and microglial activation contribute to the neuroinflammatory milieu.
Distinguishing from PTLDS: True Lyme encephalopathy occurs during active, confirmed infection and should improve with antibiotic treatment. Post-treatment Lyme disease syndrome (PTLDS) — persistent symptoms after adequate treatment — is a separate entity that should not be called Lyme encephalopathy in the absence of evidence of ongoing infection. CSF ELISA showing intrathecal antibody production is the most reliable way to confirm CNS involvement during active disease. After successful treatment, most patients with true Lyme encephalopathy show cognitive improvement over six to twelve months.
Lyme Carditis in Late Disease
Cardiac involvement in Lyme disease — Lyme carditis — most typically occurs during early disseminated disease, appearing two to eight weeks after the initial infection. However, it occasionally presents as a late manifestation or goes unrecognized until a late stage of illness.
The hallmark is conduction system disease: varying degrees of atrioventricular (AV) block. First-degree AV block (prolonged PR interval on ECG) is most common and often asymptomatic. Mobitz type I and type II second-degree block cause intermittent dropped beats. Complete (third-degree) heart block — where atrial and ventricular activity are dissociated — can cause syncope, pre-syncope, and, in rare cases, sudden cardiac death. All grades of block typically fluctuate rapidly in Lyme carditis, which distinguishes it from fixed conduction disease from other causes.
Myopericarditis (inflammation of the heart muscle and its surrounding sac) occurs less commonly but can cause chest pain, shortness of breath, and reduced cardiac function. Several cases of Lyme-associated sudden cardiac death have been reported in the literature, typically in young adults with unrecognized complete heart block.
Management: Antibiotic therapy (IV ceftriaxone for high-degree block; oral doxycycline for first-degree) resolves carditis in most cases. Temporary transvenous pacing is required in patients with high-degree AV block causing hemodynamic instability. Permanent pacing is rarely needed — the block typically resolves within days to weeks of starting antibiotics. Continuous cardiac monitoring during initial treatment is standard of care for significant heart block.
Ocular Lyme Disease
Eye involvement in Lyme disease is uncommon but well-documented and can affect multiple ocular structures. B. burgdorferi has been demonstrated in ocular tissue in animal models, and clinical cases of Lyme-associated uveitis (inflammation inside the eye — the iris, ciliary body, and choroid) have been reported in endemic areas. Uveitis in Lyme disease can be anterior (affecting the front structures) or posterior (involving the retina and choroid), and patients may present with eye pain, redness, photophobia, floaters, or decreased vision.
Other documented ocular manifestations include optic neuritis (inflammation of the optic nerve causing vision loss and pain with eye movement), keratitis (corneal inflammation), episcleritis (inflammation of the tissue overlying the white of the eye), and papilledema (optic disc swelling from elevated intracranial pressure in Lyme meningitis).
Diagnosis requires both positive Lyme serology in the appropriate clinical context and exclusion of other causes of uveitis (sarcoidosis, HLA-B27-associated disease, viral uveitis, toxoplasmosis). Treatment combines systemic antibiotics for the underlying infection and anti-inflammatory agents (topical or systemic corticosteroids) for intraocular inflammation. Prognosis depends on the degree of inflammation and how promptly treatment is initiated — most patients recover well, though posterior segment involvement carries higher risk of permanent visual impairment.
Acrodermatitis Chronica Atrophicans (European Lyme)
Acrodermatitis chronica atrophicans (ACA) is a late skin manifestation of Lyme disease that is far more common in Europe than in North America, reflecting the predominance of Borrelia afzelii in European ticks. It may develop months to years after the initial tick bite, often without a recalled EM rash or earlier symptoms.
ACA typically begins on the extremities — often the dorsum of the foot or lower leg — as a reddish-blue discoloration with subtle swelling. Over months to years, the skin in the affected area undergoes progressive atrophy: it thins dramatically, loses subcutaneous fat, and takes on a tissue-paper or cigarette-paper appearance, with prominent underlying veins visible through the transparent skin. The affected area may have a "wrinkled silk" texture. The process is relentless without treatment.
Peripheral neuropathy co-occurs in the affected limb in 40–70% of ACA patients, producing numbness, tingling, and burning pain. Borrelia can be detected by culture or PCR from the skin lesion even in very late disease, confirming ongoing spirochetal infection as the driver. Serological testing (IgG) is strongly positive in virtually all ACA cases.
Treatment with prolonged oral doxycycline (three to four weeks, sometimes longer in advanced cases) leads to resolution of active inflammation, though atrophic skin changes that have already occurred are irreversible. ACA should be considered in patients returning from endemic European areas with unexplained progressive skin atrophy on the extremities.
Pediatric Late Lyme Disease
Children account for a disproportionate number of Lyme disease cases in the United States, partly because of outdoor activity in tick-endemic areas during summer months. Late Lyme disease in children has some important differences from the adult presentation.
Facial nerve palsy is the most common neurological manifestation in pediatric Lyme disease — occurring more frequently in children than in adults with Lyme neuroborreliosis. Bilateral facial palsy, while rare in adults with Bell's palsy from other causes, should strongly prompt Lyme testing in children from endemic areas. Recovery with antibiotic treatment is excellent in most pediatric cases.
Lyme arthritis is also common in children and often the presenting feature that leads to diagnosis. The knee is again the predominant joint. Most children respond well to oral antibiotic therapy (doxycycline in those over eight years; amoxicillin in younger children). The minority with antibiotic-refractory arthritis respond to anti-inflammatory treatment as in adults.
Cognitive and behavioral changes — declining school performance, increased irritability, difficulty concentrating, fatigue — may be subtle manifestations of Lyme encephalopathy in children who cannot articulate what they are experiencing. Parental or teacher observation of behavioral changes in a child from an endemic area should prompt Lyme evaluation. With treatment, most children recover fully. Long-term neurodevelopmental consequences from untreated pediatric Lyme encephalopathy are not well characterized but are a concern that motivates prompt diagnosis and treatment.
Untreated Lyme — What Happens Over Time
Historical data from pre-antibiotic-era cases and natural history studies conducted before effective treatment was standard give a picture of what happens when Lyme disease progresses without intervention. The initial EM rash resolves spontaneously within weeks regardless of treatment — it is a localized inflammatory response, not a sign that the infection is clearing. The spirochetes disseminate during this time.
In the 1970s and 1980s pre-diagnosis era, untreated patients in Lyme, Connecticut (where the disease was first described) developed persistent arthritis, recurrent neurological problems, and, in some cases, cardiac disease. The Steere et al. natural history cohort documented that without treatment, 60% developed Lyme arthritis, 15% developed neurological complications, and 8% developed cardiac involvement. These numbers represent the pre-treatment worst case.
With modern diagnosis and antibiotic treatment, the vast majority of patients — at any stage — recover fully. Late-stage disease that has not caused permanent structural damage (such as irreversible joint destruction or established nerve fiber loss) responds well to appropriate antibiotics. The message for patients is simultaneously sobering (untreated infection does progress and cause harm) and reassuring (treatment works at any stage, and the prognosis for treated late Lyme remains good).
The minority of patients who develop post-treatment Lyme disease syndrome — persistent symptoms after adequate antibiotic courses — are not experiencing ongoing bacterial infection but rather its aftermath. Understanding this distinction is critical for appropriate management and for having realistic expectations about the timeline of recovery.
Research Papers
These peer-reviewed publications provide the evidence base for understanding late Lyme disease manifestations:
- Search PubMed — Steere AC et al. Lyme arthritis: an epidemic of oligoarticular arthritis in children and adults in three Connecticut communities.
- Search PubMed — Logigian EL et al. Chronic neurologic manifestations of Lyme disease.
- Search PubMed — Lantos PM. Chronic Lyme disease: the controversies and the science.
- Search PubMed — Steere AC et al. Antibiotic-refractory Lyme arthritis is associated with HLA-DR molecules that bind a Borrelia burgdorferi peptide.
- Search PubMed — Mead PS. Epidemiology of Lyme disease. Infectious Disease Clinics of North America.
- Search PubMed — Wormser GP et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by IDSA.
- Search PubMed — Kullberg BJ, Vrijmoeth HD, van de Schoor F, Hovius JW. Lyme borreliosis: diagnosis and management.
- Search PubMed — Rebman AW, Aucott JN. Post-treatment Lyme disease as a model for persistent symptoms in Lyme disease.
- Search PubMed — Bhate C, Schwartz RA. Lyme disease: Part II. Management and prevention.
- Search PubMed — Borchers AT et al. Lyme disease: a rigorous review of diagnostic criteria and treatment.
Additional PubMed searches: Lyme arthritis treatment Lyme neuroborreliosis antibiotic-refractory Lyme arthritis acrodermatitis chronica atrophicans
Connections
- All Bacteria
- Early Lyme & EM Rash
- Lyme Diagnosis — ELISA & Western Blot
- Lyme Disease Symptoms Hub
- Lyme Disease Treatments Hub
- Doxycycline & Antibiotic Treatment
- Post-Treatment Lyme Disease Syndrome
- Borrelia burgdorferi Overview
- Bell's Palsy
- Peripheral Neuropathy
- Arthritis
- Fibromyalgia
- Myocarditis
- Lyme Disease — the complete overview, from tick transmission and the early rash through to the late-stage complications described here.