Lyme Disease Treatments — Antibiotics, Tick Prevention, and Post-Treatment Care
Antibiotic Treatment Protocols
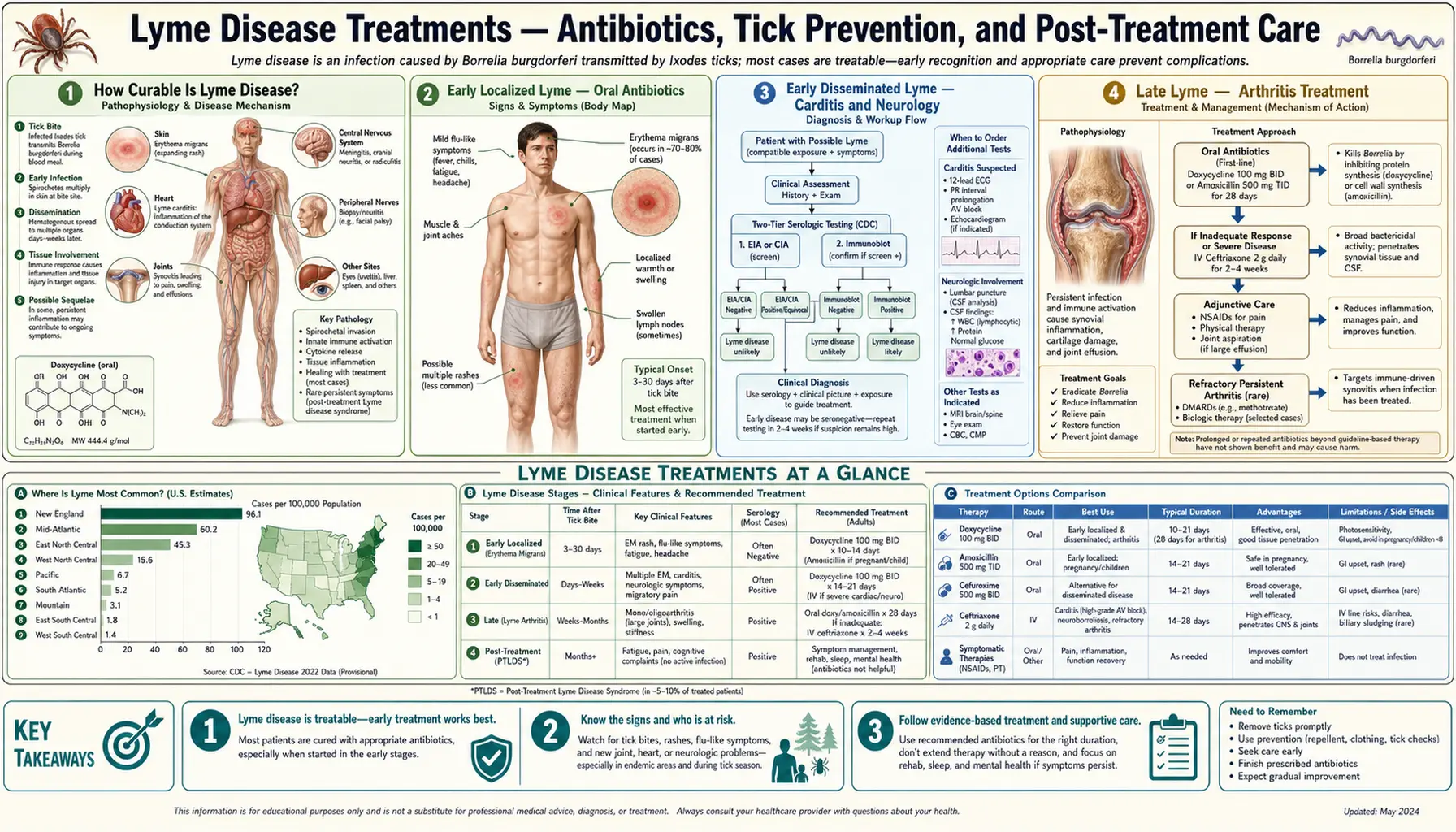
Doxycycline, amoxicillin, and ceftriaxone dosing by stage — early localized, carditis, neurological, and Lyme arthritis.
Tick Prevention & Environmental Control
DEET, permethrin, tick checks, safe removal, yard management, and the emerging Lyme vaccine.
Post-Treatment Lyme Disease Syndrome
PTLDS: persistent symptoms after adequate treatment, what the RCT evidence shows, and evidence-based management.
Table of Contents
- How Curable Is Lyme Disease?
- Early Localized Lyme — Oral Antibiotics
- Early Disseminated Lyme — Carditis and Neurology
- Late Lyme — Arthritis Treatment
- IV Ceftriaxone — When It's Needed
- Post-Exposure Prophylaxis
- Treatment in Pregnancy and Children
- What Happens If Lyme Goes Untreated
- Research Papers
- Connections
- Featured Videos
How Curable Is Lyme Disease?
Lyme disease, when treated promptly with appropriate antibiotics, is highly curable. Early localized Lyme disease — the stage of the bull's-eye EM rash before bacteria have widely disseminated — has a cure rate exceeding 95% with standard oral antibiotic courses. Patients typically begin to feel better within days of starting treatment.
Even at later stages, the prognosis remains favorable for most patients. Lyme arthritis responds to oral antibiotics in roughly 90% of cases, often without the need for intravenous treatment. Late neurological Lyme (Lyme encephalopathy, meningitis, radiculopathy) usually responds to intravenous ceftriaxone, though recovery of neurological function may take weeks to months after bacterial clearance.
The key variable is time to treatment. Delays allow Borrelia burgdorferi to disseminate through the bloodstream into joints, the nervous system, and the heart, making treatment more complex — though not impossible. The bacteria do not develop clinically significant antibiotic resistance, so treatment failure after adequate therapy is almost always due to immune-mediated inflammation rather than antibiotic-resistant organisms.
Early Localized Lyme — Oral Antibiotics
When Lyme disease is caught at the early localized stage — typically presenting as an expanding EM rash without systemic symptoms — oral antibiotics are the standard of care and are highly effective.
The preferred regimen for adults and children over 8 years old is doxycycline 100 mg twice daily for 10 days. This shorter course has been shown in clinical trials to be as effective as longer courses for uncomplicated early Lyme. Doxycycline also covers co-infections transmitted by the same tick bite, particularly Anaplasma and Ehrlichia, which is an important practical advantage in endemic areas.
Alternative regimens include amoxicillin 500 mg three times daily for 14 days, which is the preferred choice for pregnant women and children under 8 years, and cefuroxime axetil 500 mg twice daily for 14 days when neither doxycycline nor amoxicillin is tolerated. Both alternatives require a 14-day course rather than 10 days.
Most patients experience significant improvement within the first few days of starting antibiotics. The EM rash typically fades over the first week. It is important to complete the full antibiotic course even after symptoms resolve, to ensure complete bacterial clearance and reduce the risk of relapse or progression.
Early Disseminated Lyme — Carditis and Neurology
When Borrelia burgdorferi disseminates from the initial bite site through the bloodstream, it can infect the heart and nervous system within days to weeks of infection. This early disseminated stage requires treatment approaches tailored to the specific manifestation.
Lyme carditis typically presents as conduction abnormalities, most commonly atrioventricular (AV) block ranging from first-degree PR prolongation to complete heart block. First-degree and mild second-degree AV block can be managed with oral doxycycline 14–21 days, with cardiac monitoring. High-degree second-degree or third-degree (complete) AV block requires hospitalization and intravenous ceftriaxone 2 g daily until the block resolves (usually within days), after which oral therapy completes the course to a total of 21 days.
Neurological Lyme (Lyme neuroborreliosis) in its early disseminated form includes facial nerve palsy (Bell's palsy), meningitis, and radiculopathy. Isolated Lyme facial palsy, even bilateral, can be treated with oral doxycycline 14–21 days; intravenous therapy is not necessary unless cerebrospinal fluid shows active meningitis. Lyme meningitis or encephalitis, confirmed by CSF pleocytosis and positive Lyme serology, is an indication for intravenous ceftriaxone 14–28 days. Radiculopathy (shooting pain, weakness in a nerve-root distribution) generally responds to oral doxycycline 14–21 days but may require IV therapy in severe cases not improving on oral treatment.
Late Lyme — Arthritis Treatment
Lyme arthritis, which typically develops months after the initial infection, is the most common late manifestation in the United States. It presents as episodic or persistent swelling and pain, most often in the knee, though any large joint can be affected. Despite occurring late, Lyme arthritis responds well to antibiotics in the large majority of patients.
The first-line treatment is an oral antibiotic course — doxycycline 100 mg twice daily or amoxicillin 500 mg three times daily, both for 28 days. Approximately 90% of patients respond to this initial course. Response is assessed at 4 weeks: resolution of joint swelling and significant pain relief indicate success.
For patients who do not respond to the first oral course, current guidelines recommend either a second 28-day oral course or a switch to intravenous ceftriaxone 2 g daily for 14–28 days. However, if joint inflammation persists after two adequate antibiotic courses, the diagnosis shifts to antibiotic-refractory Lyme arthritis — an autoimmune process driven by ongoing immune activation even after bacterial clearance. This condition does not respond to additional antibiotics. Treatment is anti-inflammatory: NSAIDs, disease-modifying agents such as hydroxychloroquine or methotrexate, and in some cases synovectomy for persistent synovitis.
IV Ceftriaxone — When It's Needed
Intravenous ceftriaxone is a highly effective antibiotic for Lyme disease, but its use carries meaningful risks that mean it should be reserved for situations where oral antibiotics are genuinely insufficient or inappropriate.
Established indications for intravenous ceftriaxone in Lyme disease include: Lyme meningitis or encephalitis, where CNS penetration of oral drugs may be suboptimal; high-degree AV block requiring hospitalization; severe radiculopathy that has not responded to a trial of oral therapy; and certain cases of Lyme arthritis after oral treatment failure.
The standard dose is ceftriaxone 2 g intravenously once daily for 14–28 days depending on the indication. Delivery usually requires a peripherally inserted central catheter (PICC line) for outpatient IV therapy.
Risks of intravenous ceftriaxone are significant: biliary sludge or cholecystitis occurs in 2–7% of patients (ceftriaxone concentrates in bile and precipitates with calcium); Clostridioides difficile colitis; and central line-associated bloodstream infections. Several studies report serious adverse events from IV therapy exceeding those from the disease itself when used inappropriately. This underscores the importance of transitioning to oral therapy as soon as clinically possible — for example, switching from IV to oral doxycycline once a high-degree AV block resolves.
Post-Exposure Prophylaxis
A single dose of antibiotic taken shortly after a tick bite can prevent Lyme disease from developing — but this option applies only in specific circumstances, and is not appropriate for every tick bite.
Post-exposure prophylaxis (PEP) consists of a single 200 mg dose of doxycycline taken within 72 hours of tick removal. The evidence base comes from a landmark randomized controlled trial by Nadelman and colleagues (2001), which found that a single dose of doxycycline reduced the risk of developing erythema migrans by 87% compared to placebo among patients bitten by deer ticks in an endemic area.
Criteria for offering PEP (all should apply): the tick is identified as an Ixodes scapularis (black-legged/deer tick); the tick was attached for at least 36 hours; the bite occurred in an area endemic for Lyme disease; and doxycycline is not contraindicated (i.e., the patient is not pregnant, not under 8 years old, and has no contraindications). Single-dose doxycycline is not recommended for non-Ixodes ticks, brief attachments, or non-endemic regions, as the absolute risk of Lyme disease in those situations is too low to justify treatment.
Treatment in Pregnancy and Children
Lyme disease during pregnancy requires prompt treatment to protect both mother and fetus. Borrelia burgdorferi can cross the placenta, and case reports document adverse fetal outcomes with untreated maternal Lyme disease, though controlled data are limited. The antibiotic of choice is amoxicillin 500 mg three times daily for 14–21 days for early Lyme, or 28 days for arthritis. Amoxicillin is FDA category B and considered safe throughout pregnancy.
Doxycycline is contraindicated in pregnancy (fetal bone and tooth effects) and in children under 8 years (dental staining of developing permanent teeth). The IDSA 2020 guidelines make this a firm contraindication, not just a preference. For pregnant women who require intravenous therapy (meningitis, high-degree AV block), ceftriaxone 2 g IV daily is the appropriate choice and is considered safe in pregnancy.
For children under 8 years, amoxicillin 50 mg/kg/day divided into three doses (maximum 500 mg per dose) is the first-line oral therapy. Cefuroxime axetil (30 mg/kg/day in two doses, maximum 500 mg per dose) is an alternative. As in adults, intravenous ceftriaxone is used for severe neurological disease or high-degree cardiac block.
What Happens If Lyme Goes Untreated
Understanding the natural history of untreated Lyme disease underscores why diagnosis and treatment matter — while also clarifying some of the exaggerated claims made in alternative medicine contexts.
In some patients, early localized Lyme disease may resolve spontaneously without treatment. However, this spontaneous resolution is unpredictable, and a significant proportion of untreated patients progress to disseminated disease over weeks to months. The EM rash itself can disappear even as spirochetes are spreading to other organ systems.
Untreated early disseminated Lyme can lead to persistent neurological deficits (facial weakness, cognitive difficulties), recurrent arthritis affecting multiple joints, and, rarely, chronic Lyme carditis. Late neurological Lyme, particularly encephalopathy or severe radiculopathy, can cause lasting impairment if treatment is delayed by months or years.
Importantly, even with longstanding untreated infection, antibiotic treatment usually produces improvement — sometimes dramatic improvement — though full recovery of previously damaged tissues is not always possible. The spirochetes remain susceptible to antibiotics regardless of how long the infection has been present. This distinguishes Lyme from some other chronic infections where antibiotic resistance accumulates over time.
Research Papers
- Search PubMed — Wormser GP et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by IDSA. Clin Infect Dis. 2006.
- Search PubMed — Lantos PM et al. Empiric antibiotic treatment of erythema migrans-like skin lesions as a function of geography: a clinical and cost effectiveness modeling study. Vector Borne Zoonotic Dis. 2013.
- Search PubMed — Hu LT. Lyme Disease. Ann Intern Med. 2016.
- Search PubMed — Klempner MS et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001.
- Search PubMed — Krupp LB et al. Study and treatment of post Lyme disease (STOP-LD): a randomized double masked clinical trial. Neurology. 2003.
- Search PubMed — Berende A et al. Randomized trial of longer-term therapy for symptoms attributed to Lyme disease. N Engl J Med. 2016.
- Search PubMed — Skar GL & Simonsen KA. Lyme Disease. StatPearls. 2023.
- Search PubMed — Steere AC et al. Lyme borreliosis. Nat Rev Dis Primers. 2016.
- Search PubMed — Nadelman RB et al. Prophylaxis with single-dose doxycycline for the prevention of Lyme disease after an Ixodes scapularis tick bite. N Engl J Med. 2001.
- Search PubMed — Shapiro ED. Lyme Disease. N Engl J Med. 2014.
Connections
- Antibiotic Treatment Protocols
- Tick Prevention & Environmental Control
- Post-Treatment Lyme Disease Syndrome (PTLDS)
- Lyme Disease Symptoms Hub
- Early Lyme & EM Rash
- Late Lyme, Neuroborreliosis & Arthritis
- Lyme Diagnosis — ELISA & Western Blot
- Borrelia burgdorferi Main Page
- Arthritis
- Peripheral Neuropathy
- All Bacteria
- Lyme Disease — the main disease overview these protocols treat: stages, diagnosis, and prognosis.