Post-Treatment Lyme Disease Syndrome (PTLDS) — Persistent Symptoms, Evidence, and Management
- What Is PTLDS?
- How Common Is PTLDS?
- Symptoms — What Patients Experience
- Theories About What Causes PTLDS
- The NIH-Sponsored RCT Evidence
- What the Trials Don't Tell Us
- The "Chronic Lyme" Label and Its Problems
- Conditions That Overlap With PTLDS
- Evidence-Based Management Strategies
- Pain Management in PTLDS
- Cognitive and Mental Health Support
- Research Papers
- Connections
- Featured Videos
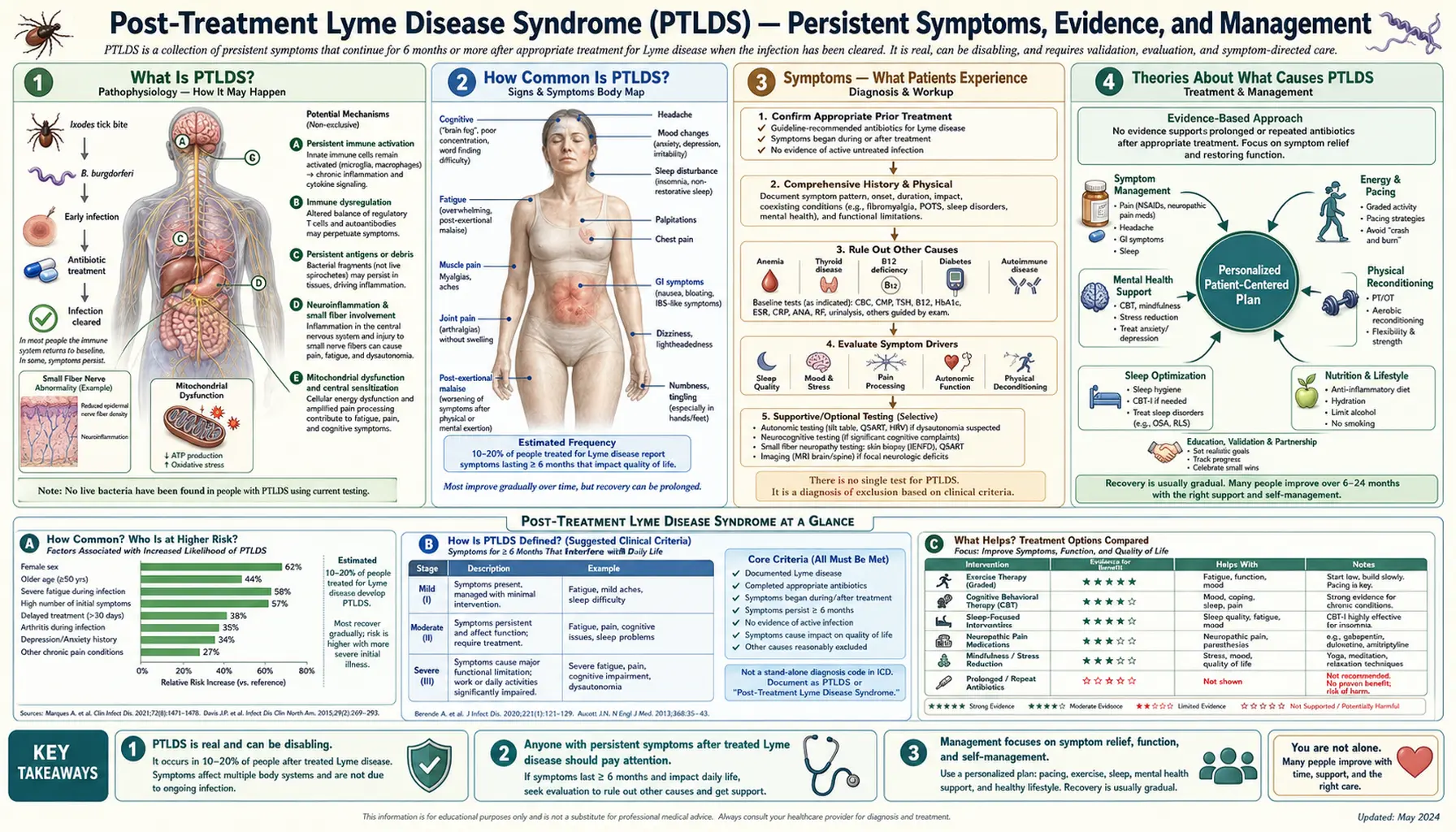
What Is PTLDS?
Post-Treatment Lyme Disease Syndrome (PTLDS) is the persistence of fatigue, musculoskeletal pain, and cognitive difficulties for more than 6 months after completing a recommended course of antibiotic therapy for confirmed Lyme disease. The term was coined to distinguish this post-infectious syndrome from the claim that active Borrelia burgdorferi infection continues — the evidence for ongoing viable infection after standard treatment is not established. But "PTLDS" also doesn't mean the symptoms aren't real. They are. And for the people experiencing them — sometimes for years — PTLDS can be profoundly disabling.
This page explains what we know, what remains unknown, and what can actually help.
How Common Is PTLDS?
Estimates range from 5% to 20% of people treated for Lyme disease, depending on the study and case definition used. Roughly 476,000 new Lyme disease cases are diagnosed in the US annually — meaning tens of thousands of people may develop PTLDS each year.
Risk factors for developing PTLDS include:
- Delayed diagnosis or treatment
- Severe initial illness
- Presence of neurological involvement at time of diagnosis
- Certain HLA subtypes (genetic differences in immune response)
PTLDS is more common in women and in patients who had more severe early-stage disease. Importantly, it does not appear to be more likely in patients whose antibiotic courses were shorter or longer within the recommended range — the key predictor is disease severity at presentation, not treatment duration.
Symptoms — What Patients Experience
PTLDS symptoms typically include:
- Profound fatigue — not ordinary tiredness; can be as limiting as that seen in cancer chemotherapy recovery
- Musculoskeletal pain — diffuse joint pain, muscle aches, often migrating day to day
- Cognitive dysfunction — "brain fog," difficulty concentrating, word-finding problems, poor short-term memory
- Sleep disturbance — unrefreshing sleep, insomnia, or hypersomnia
- Headaches and mood changes including depression and anxiety
Symptoms fluctuate and frequently worsen with physical or cognitive exertion — a phenomenon called post-exertional malaise (PEM), which is also seen in ME/CFS. They are often invisible: patients may look healthy while feeling severely ill. This discordance between outward appearance and inner experience is one of the most demoralizing aspects of the illness, and contributes to the common experience of not being believed by physicians, employers, or family.
Neuropsychological testing has documented measurable cognitive impairment in a significant subset of PTLDS patients — this is not subjective complaint alone. Brain imaging studies using PET scans have shown differences in microglial activation patterns compared to healthy controls.
Theories About What Causes PTLDS
No single mechanism has been proven. Several non-mutually-exclusive theories are under active investigation:
1. Autoimmune Activation
Borrelia burgdorferi surface proteins — especially OspA — share molecular similarity with human proteins including LFA-1 (a lymphocyte adhesion molecule) and neural antigens. The immune system, primed during infection, may continue attacking host tissue via this molecular mimicry. Anti-neural antibodies have been identified in some PTLDS patients, providing biological plausibility for this mechanism.
2. Persistent Neuroinflammation
PET imaging studies using a radiotracer that binds to activated microglia (brain immune cells) have shown elevated neuroinflammation markers in PTLDS patients compared to healthy controls — particularly in areas associated with fatigue, pain processing, and cognition. The original infection may trigger microglial activation that becomes self-sustaining.
3. Persistent Non-Viable Antigens
Dead bacterial fragments — cell wall components, outer surface proteins, DNA — may persist in tissues long after viable bacteria are eliminated and continue to drive inflammatory signaling. This mechanism has precedent in other post-infectious syndromes.
4. Post-Infectious Immune Dysregulation
PTLDS shares striking features with post-infectious syndromes seen after other pathogens: post-COVID (Long COVID), post-Q fever fatigue syndrome, and post-EBV mononucleosis syndrome. The commonality suggests a general susceptibility — possibly genetic — to prolonged immune dysregulation following certain triggering infections, rather than anything unique to Borrelia.
5. Persister Cells (Controversial)
Some in-vitro laboratory research has demonstrated that B. burgdorferi can form metabolically dormant "persister" cells that survive antibiotic exposure. Whether these cells persist in living human tissue, emerge from dormancy, and contribute to ongoing symptoms is entirely unproven in human studies and remains highly contested among researchers.
6. Gut Microbiome Disruption
Antibiotic treatment inevitably disrupts the gut microbiome. Dysbiosis — an imbalance in gut bacterial communities — may contribute to fatigue, cognitive symptoms, and immune dysregulation in a subset of patients. This is an emerging area; direct evidence in PTLDS is limited but consistent with broader microbiome-illness research.
The NIH-Sponsored RCT Evidence
Four large randomized controlled trials have directly tested whether additional or prolonged antibiotic treatment helps PTLDS patients. All were funded by the NIH and published in top medical journals:
Klempner et al. 2001 (NEJM)
129 patients with well-documented prior Lyme disease and persistent symptoms were randomized to 90 days of IV ceftriaxone followed by oral doxycycline vs. matching placebos. There was no significant difference between groups in functional capacity, pain, fatigue, or cognitive function at the 180-day endpoint. One patient in the treatment arm died from a catheter-related blood clot — a real risk of prolonged IV antibiotic therapy. ( — Search PubMed)
Krupp et al. 2003 (Neurology)
55 patients with PTLDS and significant fatigue were randomized to IV ceftriaxone for 28 days vs. saline placebo. Fatigue improved more in the ceftriaxone group at 6 months — a positive result. However, cognitive outcomes did not differ between groups, and the study was limited by small sample size. This remains the most positive trial result in PTLDS antibiotic research. ( — Search PubMed)
Fallon et al. 2008 (Neurology)
37 patients with PTLDS and significant cognitive complaints were randomized to IV ceftriaxone for 10 weeks vs. placebo. There were measurable cognitive improvements at the 12-week primary endpoint in the treatment group — but these improvements were not sustained at 24 weeks follow-up. Serious adverse events occurred in the treatment arm. ( — Search PubMed)
Berende et al. 2016 (NEJM)
281 patients with PTLDS were randomized to 12 weeks of doxycycline alone, a combination antibiotic regimen, or placebo. There was no significant difference in health-related quality of life at 14 weeks or subsequent follow-up. This is the largest and most rigorously conducted trial to date. (PMID: 26973720)
Taken together: extended antibiotics do not provide sustained meaningful benefit in PTLDS and carry documented real risks including line infections, clots, and Clostridioides difficile colitis.
What the Trials Don't Tell Us
The negative antibiotic trials are definitive on one narrow question: extended antibiotics beyond standard treatment do not help PTLDS patients in a sustained, clinically meaningful way. They do not answer several other important questions:
- They don't prove symptoms are psychosomatic or imaginary. The trials document real suffering in all participants — treatment and placebo alike. The mechanism of that suffering is simply not bacterial infection requiring more antibiotics.
- They don't identify what does cause PTLDS or what mechanisms sustain it.
- They don't rule out that a subset of patients might benefit from treatments targeting specific mechanisms (autoimmune, neuroinflammatory) once those mechanisms are better characterized.
- They don't address the question of what the right treatment is — only that more antibiotics isn't it.
Research into immune mechanisms, biomarkers, and targeted therapies for PTLDS is ongoing at NIH, Johns Hopkins, Columbia, and other academic centers. The field has made meaningful progress in characterizing the biology of the syndrome even when treatment breakthroughs remain elusive.
The "Chronic Lyme" Label and Its Problems
The term "chronic Lyme disease" is used in two very different contexts, and the confusion between them causes real harm:
Mainstream Medical Use
Sometimes used loosely — and increasingly discouraged — to describe PTLDS in patients with confirmed prior Lyme disease. When used this way, it refers to a real post-infectious syndrome in documented Lyme patients.
Alternative Medicine Use
Used by some practitioners to describe a claimed condition of ongoing active Borrelia infection, diagnosed using tests not validated by the CDC or mainstream labs, in patients who may have no serological or clinical evidence of ever having had Lyme disease.
This second usage is problematic for specific reasons:
- Non-standard tests (Igenex, Galaxy Diagnostics using non-CDC criteria) have high false-positive rates — they will label many people as "Lyme positive" who never had the disease
- Patients diagnosed this way may receive months or years of antibiotic therapy — including IV antibiotics — at enormous cost, with documented risks (line infections, C. diff, antibiotic resistance), and no evidence of benefit
- This mislabeling may indefinitely delay diagnosis of the condition actually causing symptoms: lupus, multiple sclerosis, fibromyalgia, small fiber neuropathy, or other treatable conditions
The important distinction: the controversy is about diagnosis, mechanism, and treatment — not about whether patients are suffering. Patients seeking a "chronic Lyme" diagnosis are genuinely ill and often desperate after years without answers. Their suffering is real. The disagreement is whether the cause is ongoing active Borrelia infection and whether antibiotics are the right tool.
Conditions That Overlap With PTLDS
PTLDS shares features with several other conditions, and these overlaps are clinically important — both because they need independent evaluation and because treatments developed for them may benefit PTLDS patients:
- Fibromyalgia — diffuse musculoskeletal pain, fatigue, sleep dysfunction, and cognitive complaints; can be triggered by infections; shares nearly identical symptom profile with PTLDS
- ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome) — profound fatigue, post-exertional malaise, unrefreshing sleep, cognitive dysfunction; considerable patient and clinical overlap with PTLDS; some researchers consider PTLDS a triggering pathway to ME/CFS
- Small fiber neuropathy — burning pain, tingling, numbness from damage to small unmyelinated nerve fibers; diagnosed by skin punch biopsy showing reduced nerve fiber density; found in a meaningful subset of PTLDS patients; may explain neuropathic pain components
- Depression and anxiety — comorbid in many PTLDS patients; may be secondary to the burden of chronic illness, or may share an underlying neuroinflammatory mechanism; either way, treating these conditions improves quality of life independently
- Inflammatory arthritis — some patients with "Lyme arthritis" after treatment have immune-driven joint inflammation that does not respond to antibiotics but does respond to anti-inflammatory therapy; distinct mechanism from PTLDS fatigue/cognition
Each of these conditions should be evaluated and treated on its own merits in PTLDS patients — not deferred pending resolution of "the Lyme question."
Evidence-Based Management Strategies
There is no single proven treatment for PTLDS. Management is symptom-directed and multidisciplinary. The following approaches have evidence from PTLDS research, related post-infectious syndromes, fibromyalgia, and ME/CFS:
Graded Activity and Pacing
Very gentle, gradual increase in physical activity is beneficial — but the approach must be carefully individualized. The critical rule: monitor for post-exertional malaise (PEM). If activity causes significant symptom worsening lasting more than 24 hours, that activity level is too much. Scale back and increase more slowly. Aerobic activity (walking, swimming, gentle cycling) is preferred over high-intensity exercise. Activity pacing — matching activity to available energy rather than pushing through — is the cornerstone of ME/CFS management and applies to PTLDS patients with PEM.
Sleep Optimization
Regular sleep-wake schedule is essential. For insomnia: cognitive behavioral therapy for insomnia (CBT-I) is the first-line evidence-based treatment and more effective than sleep medications long-term. Avoid alcohol — it worsens sleep architecture dramatically even when it helps onset. Screen for sleep apnea with polysomnography; undiagnosed apnea markedly worsens fatigue and cognitive function. Low-dose amitriptyline (10–25 mg) at bedtime can improve sleep quality and reduce pain in fibromyalgia overlap.
Cognitive Rehabilitation
Memory aids — written calendars, smartphone reminders, task lists — compensate for working memory deficits while cognitive function recovers. Task chunking (breaking work into smaller steps with rest between) reduces cognitive overload. Some evidence exists for formal cognitive rehabilitation programs in PTLDS-related cognitive impairment.
Mental Health Support
Cognitive behavioral therapy (CBT) for coping with chronic illness is beneficial. This does not mean symptoms are "in your head" — CBT helps patients manage any chronic illness better, including cancer and heart disease. Antidepressants for comorbid depression: SSRIs (sertraline, escitalopram) for depression/anxiety; SNRIs (duloxetine, venlafaxine) have dual benefit for depression and pain.
Integrative Approaches With Some Supporting Evidence
Mindfulness-based stress reduction (MBSR) has shown benefits in chronic pain and fatigue syndromes. Anti-inflammatory dietary patterns (Mediterranean diet) reduce systemic inflammatory markers. Omega-3 fatty acid supplementation may modestly reduce inflammatory markers.
Approaches to Avoid
Alternative antibiotic protocols (herbal antibiotics, long-term rotating antibiotic regimens), ozone therapy, hyperbaric oxygen therapy, and intravenous hydrogen peroxide have no evidence of benefit for PTLDS specifically and carry documented risks. These approaches also incur significant expense that could be directed toward evidence-based care.
Pain Management in PTLDS
Musculoskeletal pain — diffuse, migratory, and often severe — is the symptom that most impairs quality of life for many PTLDS patients. A practical stepwise approach:
First-Line Analgesics
- Acetaminophen — for mild pain; safe with regular dosing (stay under 3g/day; 2g/day if drinking alcohol)
- NSAIDs (ibuprofen 400–600 mg TID, naproxen 500 mg BID) — for moderate musculoskeletal pain; more effective than acetaminophen for inflammatory-type pain; take with food; note GI and renal risks with chronic daily use
- Topical NSAIDs (diclofenac gel 1%) — for localized joint pain; comparable efficacy to oral for target joints with significantly fewer systemic effects
Second-Line for Neuropathic and Fibromyalgia Overlap
- Duloxetine (Cymbalta) 30–60 mg daily — FDA-approved for fibromyalgia and chronic musculoskeletal pain; also treats comorbid depression; beneficial for the pain/mood overlap common in PTLDS
- Pregabalin (Lyrica) or gabapentin — for neuropathic pain components, especially burning, tingling, or shooting pain; also improves sleep at low doses
- Low-dose naltrexone (LDN) 1.5–4.5 mg at bedtime — off-label; growing evidence in fibromyalgia, ME/CFS, and inflammatory conditions; proposed mechanism involves microglial modulation; well-tolerated; requires compounding pharmacy
- Low-dose tricyclics (amitriptyline 10–25 mg, nortriptyline) — improve sleep and reduce pain; not primarily for depression at these doses
Physical Therapy
Important for joint pain and deconditioning but must be paced carefully. Myofascial release, gentle stretching, aquatic therapy, and therapeutic exercise are beneficial. Communicate clearly with the physical therapist about post-exertional malaise — sessions should not cause prolonged flares.
What to Avoid
Opioids are not recommended for PTLDS or fibromyalgia-spectrum pain — poor evidence, significant risks of dependence and hyperalgesia, and they worsen sleep. Corticosteroids are not indicated except for the specific subtype of antibiotic-refractory Lyme arthritis.
Cognitive and Mental Health Support
"Brain fog" in PTLDS is not a psychiatric symptom — it reflects measurable cognitive impairment documented on formal neuropsychological testing in published research. Processing speed, working memory, and verbal recall are the most commonly affected domains. But cognitive function is worsened by depression, anxiety, sleep deprivation, and uncontrolled pain — addressing all these drivers is essential.
Practical Cognitive Supports
- Written calendars and task lists rather than relying on memory
- Smartphone reminders for medications, appointments, and tasks
- Task chunking — breaking multi-step tasks into small numbered steps
- Scheduled cognitive breaks during demanding work
- Reducing multitasking (sequential is less cognitively demanding)
Workplace Accommodations
Many PTLDS patients benefit from formal workplace accommodations under the ADA: flexible scheduling, reduced cognitive load tasks during flares, written rather than verbal instructions, and remote work options. A treating physician can document functional limitations for accommodation requests.
Mental Health Treatment
Depression and anxiety should be treated actively — not as secondary to resolving "the Lyme question." SSRIs are first-line for depression and anxiety. CBT specifically targeting chronic illness coping (not psychosomatic framing) is valuable. Peer support groups for PTLDS and ME/CFS patients provide validation and practical coping strategies that clinical visits often cannot.
Long-Term Prognosis
Most PTLDS patients improve meaningfully over months to years. Studies following PTLDS cohorts show that the majority — roughly 70–80% — experience significant symptom improvement within 1–2 years, though often not complete resolution. A minority experience persistent significant disability. Recovery is real and worth actively working toward — the prognosis, while not guaranteed, is generally better than patients fear at the height of illness.
Research Papers
- Search PubMed — Klempner et al. 2001 (NEJM): Extended antibiotics vs. placebo in PTLDS — no sustained benefit; RCT stopped early due to futility
- Search PubMed — Fallon et al. 2008 (Neurology): IV ceftriaxone for cognitive symptoms in PTLDS — short-term improvement not sustained at 24 weeks
- Search PubMed — Krupp et al. 2003 (Neurology): IV ceftriaxone for PTLDS fatigue — fatigue improved at 6 months; cognitive outcomes did not differ
- Search PubMed — Berende et al. 2016 (NEJM): Longer-duration antibiotics vs. placebo in PTLDS — no significant difference in quality of life outcomes
- Search PubMed — Aucott et al. 2019: Prospective cohort characterizing symptom domains and functional impairment in PTLDS
- Search PubMed — Rebman et al. 2018: Neuroinflammation findings in PTLDS using PET imaging; elevated microglial activation compared to controls
- Search PubMed — Bouquet et al. 2019: Cytokine and immune marker profiles distinguishing PTLDS from healthy controls and recovered Lyme patients
- Search PubMed — Wormser et al. 2012: Risk factors for PTLDS development; disease severity at presentation as primary predictor
- Search PubMed — Aucott et al. 2017: Posttreatment Lyme disease symptoms score (PLDS-S) — validated patient-reported outcome measure for PTLDS trials
- Search PubMed — Stricker & Johnson 2015: Review of immune mechanisms in PTLDS and research directions for targeted therapies
Connections
- All Bacteria
- Lyme Disease Treatments Hub
- Doxycycline & Antibiotic Treatment
- Tick Prevention & Environmental Control
- Lyme Disease Symptoms Hub
- Early Lyme & Erythema Migrans Rash
- Late Lyme, Neuroborreliosis & Arthritis
- Diagnosis: ELISA, Western Blot & Controversies
- Borrelia burgdorferi — Lyme Disease Main Page
- Fibromyalgia
- Chronic Fatigue Syndrome (ME/CFS)
- Peripheral Neuropathy