Arginine — Benefits Deep Dive
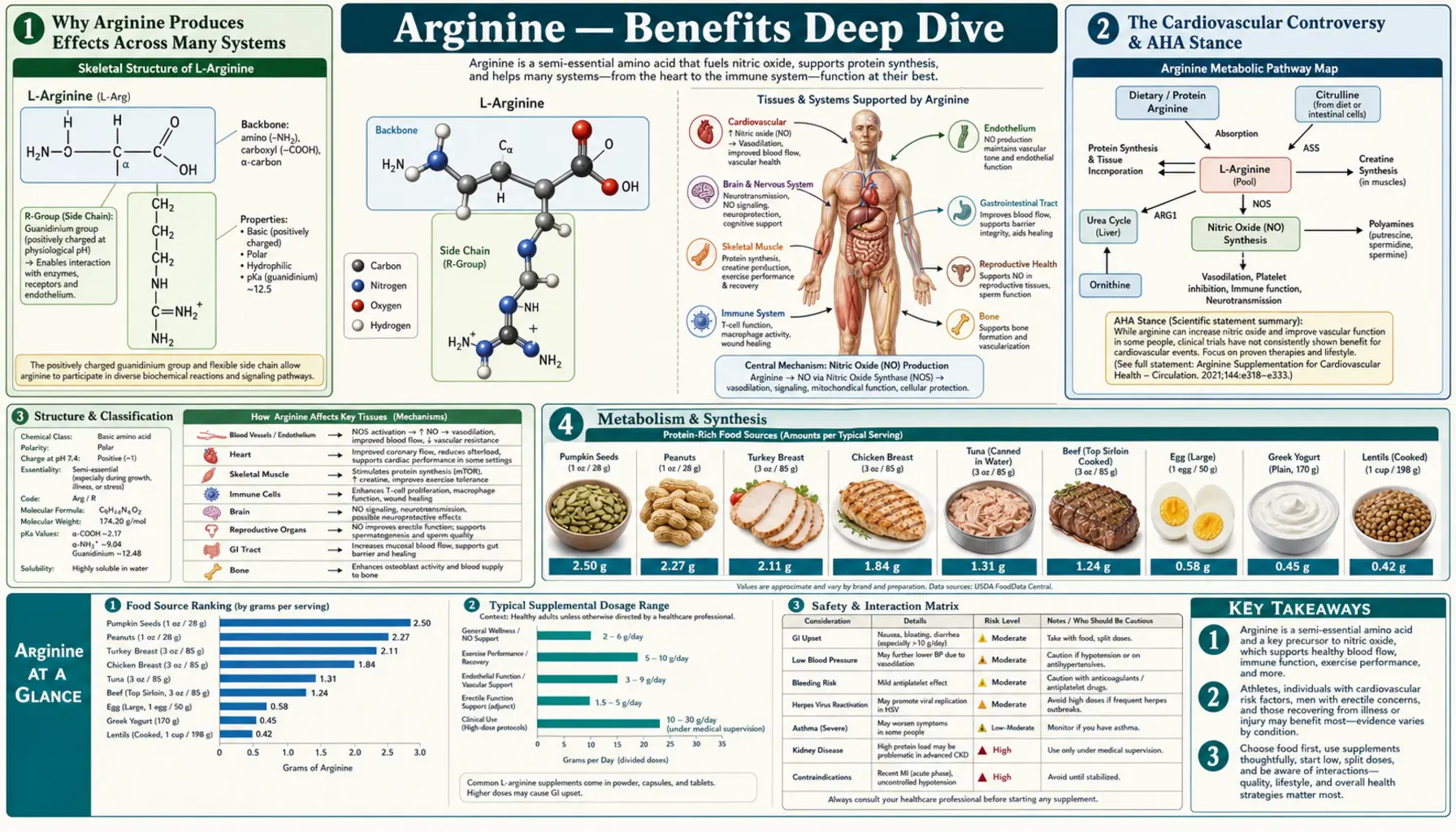
L-Arginine is the most metabolically versatile of the twenty proteinogenic amino acids. Classified as semi-essential (or conditionally essential) because adult humans can synthesize it from citrulline in the kidneys, arginine still becomes dietarily indispensable in growth, pregnancy, injury, sepsis, and any clinical state that elevates demand above endogenous production capacity. What makes arginine unique is its dual metabolic fate: a single arginine molecule can be routed through nitric oxide synthase to generate the gaseous vasodilator and antimicrobial effector molecule NO (with citrulline as byproduct), OR through arginase to generate ornithine and urea (with ornithine feeding the proline/collagen pathway and the polyamine/cell-proliferation pathway). No other amino acid sits at such a strategic fork. The four benefit pages below explore the conditions where arginine produces the largest clinical effect — vasodilator-driven cardiovascular biology including endothelial function, hypertension, and peripheral arterial disease; the NO-cGMP-PDE5 axis behind penile erection and the entire PDE5-inhibitor drug class; wound healing where both NOS and arginase arms are simultaneously required; and immune function including T-cell activation, macrophage polarization, and the tumor-microenvironment arginine-depletion mechanism that is one of the largest open frontiers in cancer immunotherapy.
Deep-Dive Articles
Cardiovascular Health & Nitric Oxide
Arginine as the obligate substrate for the entire nitric oxide synthase family (NOS1 neuronal, NOS2 inducible, NOS3 endothelial), the endothelial vasodilation that underwrites vascular health, the L-arginine/ADMA ratio as a competition that determines NO production, the L-arginine paradox in heart failure, why oral citrulline is often a more bioavailable NO precursor than arginine itself (it bypasses hepatic arginase first-pass loss), and the practical trial evidence for hypertension, peripheral arterial disease, and the cautionary VINTAGE-MI signal in post-infarct patients.
Erectile Function
The complete physiology of erection as a vascular event, the NO-cGMP-PDE5 signaling axis that is the molecular basis of every PDE5 inhibitor drug (sildenafil, tadalafil, vardenafil, avanafil), where arginine sits upstream of PDE5 inhibition in the pathway, the clinical trial evidence for arginine and citrulline monotherapy, the impressive arginine + pycnogenol combination producing 90+% response rates, comparison to pharmaceutical PDE5 inhibitors, and the PDE5 non-responder rescue protocol using citrulline.
Wound Healing
Arginine's unique dual-substrate position at the NOS / arginase fork — required as substrate for the NO arm (inflammatory phase antimicrobial defense) and for the ornithine arm (proline for collagen synthesis, polyamines for cell proliferation), the four phases of wound healing and arginine's role in each, the surgical wound healing trials (Barbul, Daly, Kirk), pressure ulcer trials (Cereda), diabetic foot ulcer evidence, and the formal immunonutrition formulations (Impact, Oral Impact) combining arginine with glutamine, omega-3 fatty acids, and nucleotides.
Immune Function
Arginine in T-cell activation via the post-translational regulation of CD3-zeta chain (the essential TCR signaling component), the M1/M2 macrophage polarization that defines arginine's opposite metabolic fates in pro-inflammatory vs pro-resolving cells, the MDSC (myeloid-derived suppressor cell) arginase mechanism that drives tumor immunosuppression and resistance to checkpoint inhibitors, septic patient arginine deficiency, ICU immunonutrition (the cautionary Bertolini trial), and arginine in sickle cell disease and asthma.
Table of Contents
- Deep-Dive Articles
- Why Arginine Produces Effects Across Many Systems
- The Cardiovascular Controversy & AHA Stance
- Research Papers: Cardiovascular & NO
- Research Papers: Erectile Function
- Research Papers: Wound Healing
- Research Papers: Immune Function
- Research Papers: Cross-Cutting (Metabolism, Safety)
- External Authoritative Resources
- Connections
- Featured Videos
Why Arginine Produces Effects Across Many Systems
Most amino acids serve one principal function (protein synthesis) and perhaps one or two specialized derivatives. Arginine is fundamentally different because it operates simultaneously through at least five distinct metabolic pathways, each producing molecules with major physiological effects. This makes arginine the most metabolically versatile amino acid in human biochemistry, and explains why arginine status affects systems as diverse as the cardiovascular, immune, reproductive, musculoskeletal, and renal.
- Nitric oxide synthase substrate — the three NOS isoforms (NOS1 neuronal, NOS2 inducible, NOS3 endothelial) all draw exclusively on the arginine pool to produce NO. This single mechanism drives the cardiovascular effects on endothelial vasodilation, blood pressure, and peripheral arterial perfusion, the NO-cGMP-PDE5 cascade of penile erection, the antimicrobial effector arm of inflammatory wound healing, and the macrophage-mediated component of innate immune defense.
- Urea cycle substrate (arginase pathway) — arginase converts arginine to ornithine and urea, the latter being the principal nitrogenous waste product in mammals. The ornithine generated feeds the proline pathway (essential for collagen synthesis in connective tissue and wound healing) and the polyamine pathway (essential for cell proliferation in healing wounds, immune responses, and any rapidly dividing tissue). This is the second arm of the arginine fork that operates in opposition to the NOS arm.
- Protein synthesis — like all amino acids, arginine is incorporated into newly synthesized proteins. The arginine residues in proteins serve specific structural roles (positively charged side chain for ionic interactions, often binding to negatively charged phosphates in DNA, RNA, and ATP-binding pockets) and regulatory roles (arginine methylation is a major post-translational modification that controls protein-protein interactions and chromatin biology).
- Creatine synthesis — arginine combines with glycine via arginine:glycine amidinotransferase (AGAT) to form guanidinoacetate, which is then methylated by guanidinoacetate methyltransferase (GAMT) using methionine-derived S-adenosylmethionine to form creatine. Creatine is the principal high-energy phosphate buffer in muscle, where phosphocreatine donates its phosphate to ADP to regenerate ATP during high-intensity exercise. See Creatine.
- Agmatine and other minor pathways — arginine decarboxylase produces agmatine, a biogenic amine with effects on imidazoline receptors, NMDA receptor modulation, and several other neurological signaling pathways. The clinical significance is less well-defined than the major pathways but represents another dimension of arginine's biochemical scope.
The therapeutic complication of this versatility is that arginine effects can be context-dependent and sometimes paradoxical. Adding arginine to a patient whose limiting bottleneck is NOS substrate produces increased NO and the expected vasodilatory effects. Adding arginine to a patient whose macrophages are dominated by the M2 (arginase-expressing) phenotype may feed pathological tissue remodeling rather than the desired NO production. Adding arginine to a septic patient with already-upregulated iNOS can worsen hypotension. The clinical art is matching the supplementation strategy to the dominant pathophysiology rather than treating arginine as a generic immune or vascular tonic.
The Cardiovascular Controversy & AHA Stance
Arginine's cardiovascular story is one of the most clinically interesting and contested in supplement medicine. The biochemistry is compelling: arginine is the obligate substrate for the enzyme that produces nitric oxide, the most important endogenous vasodilator and the molecule whose impairment defines endothelial dysfunction (the earliest detectable abnormality in atherosclerosis). The hypothesis is straightforward: supplement the substrate, restore NO production, improve vascular health.
The trial evidence is more mixed than the hypothesis would predict:
- Positive trials — Boger's peripheral arterial disease trial (Circulation 1998), the Dong meta-analysis showing meaningful blood pressure reduction with oral arginine (2011), multiple smaller trials showing improved flow-mediated dilation in endothelial dysfunction
- Negative trials — the VINTAGE-MI trial (JAMA 2006), which showed increased mortality in post-myocardial infarction patients given oral arginine, leading the data safety monitoring board to stop the trial early. The mechanism is thought to involve peroxynitrite generation in the oxidatively stressed post-MI myocardium, where NO produced from arginine reacts with abundant superoxide to form a potent cytotoxic oxidant.
- Inconsistent trials — many smaller studies in stable angina, heart failure, and primary prevention have produced inconsistent results, with effect sizes that are modest at best.
The American Heart Association has not endorsed arginine as a cardiovascular intervention. The AHA scientific statements on functional foods and supplements acknowledge the literature but conclude that the evidence base is insufficient to recommend routine supplementation. Most cardiologists treat arginine the same way — available as an adjunct in selected patients (particularly those with peripheral arterial disease, gestational hypertension prevention, or documented endothelial dysfunction with elevated ADMA), but not part of standard cardiovascular management.
The clinical practice implication: arginine for cardiovascular health is reasonable in specific patient populations (PAD, gestational hypertension, mild hypertension with endothelial dysfunction) but should not be used in post-MI patients, in severe heart failure without cardiology supervision, or as a replacement for established cardiovascular medications. L-citrulline is often a better choice than direct arginine because of better bioavailability and tolerability. The full clinical discussion is on the Cardiovascular and NO deep-dive.
The other clinically important caution is the herpes/lysine antagonism. Arginine is a required substrate for herpes simplex virus replication, and lysine competes with arginine for cellular uptake and incorporation. The classical naturopathic teaching is that high arginine intake can precipitate herpes outbreaks, and that the lysine-to-arginine ratio in diet (or supplementation) influences outbreak frequency. The clinical literature is modest but consistent — many integrative practitioners recommend lysine 1–2 g/day for patients with frequent herpes recurrences, particularly if they are also taking arginine for cardiovascular or athletic indications. The L-Lysine page covers the lysine side of this antagonism.
Research Papers: Cardiovascular & NO
- Boger RH et al. (1998). Restoring vascular nitric oxide formation by L-arginine improves the symptoms of intermittent claudication in patients with peripheral arterial occlusive disease — PubMed: Boger PAD trial
- Schulman SP et al. VINTAGE-MI: L-arginine therapy in acute myocardial infarction (JAMA 2006) — PubMed: VINTAGE-MI
- Dong JY et al. (2011). Effect of oral L-arginine supplementation on blood pressure: a meta-analysis — PubMed: Dong meta-analysis
- Schwedhelm E et al. (2008). Pharmacokinetic properties of oral L-citrulline and L-arginine — PubMed: Citrulline pharmacokinetics
- Vallance P, Leiper J (2004). Cardiovascular biology of the ADMA / DDAH pathway — PubMed: ADMA cardiovascular biology
- Forstermann U, Sessa WC (2012). Nitric oxide synthases: regulation and function — PubMed: NOS regulation
- Bode-Boger SM et al. (2003). The L-arginine paradox: importance of the L-arginine/ADMA ratio — PubMed: Arginine paradox
- Hayashi T et al. (2005). Citrulline and arginine retard atherosclerosis in rabbits — PubMed: Atherosclerosis prevention
- Loscalzo J (2004). L-Arginine and atherothrombosis — PubMed: Loscalzo review
- Moinard C et al. (2008). Citrulline dose-ranging effects on plasma amino acids and hormones — PubMed: Moinard citrulline study
Research Papers: Erectile Function
- Stanislavov R, Nikolova V (2003). Treatment of erectile dysfunction with pycnogenol and L-arginine — PubMed: Pycnogenol + arginine 92% response
- Chen J et al. (1999). High-dose nitric oxide donor L-arginine in men with organic ED — PubMed: Chen arginine ED trial
- Cormio L et al. (2011). Oral L-citrulline supplementation improves erection hardness in mild ED — PubMed: Cormio citrulline ED
- Rhim HC et al. (2019). Arginine supplements on erectile dysfunction: meta-analysis — PubMed: Rhim meta-analysis
- Goldstein I et al. (1998). Oral sildenafil in the treatment of erectile dysfunction (NEJM) — PubMed: Sildenafil NEJM original
- Burnett AL (2006). The role of nitric oxide in erectile dysfunction — PubMed: Burnett NO and ED
- Toda N et al. (2005). Nitric oxide and penile erectile function — PubMed: Toda NO and erection
- Aoki H et al. (2012). Pycnogenol and L-arginine in Japanese patients with mild to moderate ED — PubMed: Aoki pycnogenol trial
- Shamloul R, Ghanem H (2013). Erectile dysfunction (Lancet review) — PubMed: Lancet ED review
- Andersson KE, Wagner G (1995). Physiology of penile erection — PubMed: Erection physiology
Research Papers: Wound Healing
- Barbul A et al. (1990). Arginine enhances wound healing and lymphocyte immune responses in humans — PubMed: Barbul classic wound trial
- Kirk SJ et al. (1993). Arginine stimulates wound healing and immune function in elderly humans — PubMed: Kirk elderly wound trial
- Cereda E et al. (2015). Arginine, zinc, antioxidants for pressure ulcer healing (Annals Internal Med) — PubMed: Cereda pressure ulcer
- Daly JM et al. (1995). Enteral immunonutrition in upper GI cancer surgery — PubMed: Daly immunonutrition
- Marimuthu K et al. (2012). Immunonutrition meta-analysis for major GI surgery — PubMed: Marimuthu meta-analysis
- Witte MB, Barbul A (2003). Arginine physiology and wound healing — PubMed: Witte/Barbul review
- Drover JW et al. (2011). Perioperative arginine-supplemented diets: systematic review — PubMed: Drover perioperative review
- Stechmiller JK et al. (2005). Arginine supplementation and wound healing — PubMed: Stechmiller review
- Albina JE et al. (1990). Arginine metabolism in wounds — PubMed: Albina classic
- Armstrong DG et al. (2014). Oral nutritional supplementation in diabetic foot ulcers — PubMed: Armstrong diabetic foot
Research Papers: Immune Function
- Rodriguez PC et al. (2002). Regulation of T-cell receptor CD3-zeta chain expression by L-arginine — PubMed: Rodriguez CD3-zeta
- Bronte V, Zanovello P (2005). Regulation of immune responses by L-arginine metabolism (Nature Reviews Immunology) — PubMed: Bronte/Zanovello review
- Rodriguez PC, Ochoa AC (2008). Arginine regulation by MDSCs and tolerance in cancer — PubMed: MDSC arginase mechanism
- Geiger R et al. (2016). L-arginine modulates T-cell metabolism and anti-tumor activity (Cell) — PubMed: Geiger T-cell metabolism
- Bertolini G et al. (2003). Early enteral immunonutrition in severe sepsis: interim analysis — PubMed: Bertolini sepsis trial
- Morris CR et al. (2013). Arginine therapy in sickle cell vaso-occlusive pain — PubMed: Morris sickle cell trial
- Steggerda SM et al. (2017). Arginase inhibition by CB-1158 in tumor microenvironment — PubMed: CB-1158 arginase inhibitor
- Maarsingh H et al. (2009). Arginase in allergic asthma pathophysiology — PubMed: Arginase in asthma
- Munder M (2009). Arginase as emerging player in mammalian immune system — PubMed: Munder arginase review
- Calder PC (2007). Immunonutrition in surgical and critically ill patients — PubMed: Calder immunonutrition
Research Papers: Cross-Cutting (Metabolism, Safety)
- Morris SM Jr (2009). Recent advances in arginine metabolism: roles and regulation of the arginases — PubMed: Morris arginase review
- Wu G, Morris SM Jr (1998). Arginine metabolism: nitric oxide and beyond — PubMed: Wu/Morris classic review
- Luiking YC et al. (2009). Arginine de novo and nitric oxide production in disease states — PubMed: Luiking de novo synthesis
- Boger RH (2007). The pharmacodynamics of L-arginine — PubMed: Boger pharmacodynamics
- Husson A et al. (2003). Argininosuccinate synthetase from the urea cycle to the citrulline-NO cycle — PubMed: ASS enzyme
- Castillo L et al. (1993). Splanchnic metabolism of dietary arginine in relation to nitric oxide synthesis — PubMed: Splanchnic first-pass
- Curis E et al. (2005). Almost all about citrulline in mammals — PubMed: Curis citrulline review
- Wu G et al. (2009). Arginine metabolism and nutrition in growth, health and disease — PubMed: Wu nutrition review
- Hannemann J et al. (2020). Safety of L-arginine and L-citrulline supplementation: a systematic review — PubMed: Safety review
- Griffith RS et al. (1987). Lysine vs arginine for herpes simplex virus — PubMed: Lysine/arginine HSV
External Authoritative Resources
- Linus Pauling Institute — L-Arginine Micronutrient Information Center — the most authoritative scientific summary of arginine biology, regularly updated
- NIH Office of Dietary Supplements — Fact Sheets
- MedlinePlus — L-Arginine (consumer-oriented summary of uses, evidence, and interactions)
- American Heart Association — AHA scientific statements on functional foods and supplements
- PubMed — All research on L-arginine (~90,000+ papers)
- PubMed — All research on L-citrulline (~4,000+ papers)
Connections
- Arginine (Main Page)
- Arginine for Cardiovascular Health & NO
- Arginine for Erectile Function
- Arginine for Wound Healing
- Arginine for Immune Function
- All Amino Acids
- Lysine
- Taurine
- Glutamine
- Glycine
- Proline
- Methionine
- Cardiovascular Disease
- Hypertension
- Erectile Dysfunction
- Diabetes
- Metabolic Syndrome
- Lysine (HSV Counterbalance)
- Creatine
- Collagen
- Zinc
- Vitamin C
- Kidney Function
- Immune Boosting