Arginine for Erectile Function
Penile erection is, at its core, a vascular event. The trigger is sexual stimulation; the proximate cause is neuronal and endothelial nitric oxide release in the corpus cavernosum; the substrate that the relevant NOS isoforms cannot function without is L-arginine. This makes arginine the only nutritional intervention that sits upstream of the exact biochemical pathway exploited by the entire $10-billion-per-year PDE5 inhibitor industry — sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra), and avanafil all work by preserving the cGMP signal that NO triggers, but they require functional NO production upstream to have anything to preserve. For men with mild to moderate erectile dysfunction, particularly when ED is linked to endothelial dysfunction, hypertension, diabetes, or aging, oral arginine or citrulline supplementation can produce clinically meaningful improvement — sometimes sufficient to obviate the need for PDE5 inhibitors, sometimes restoring response in PDE5-nonresponders, and sometimes simply improving the quality and reliability of natural erections. The strongest evidence is for the arginine + pycnogenol combination, which has produced restoration of normal erectile function in over 90% of participants in published trials. This deep-dive covers the NO-cGMP-PDE5 axis, the comparative pharmacology of arginine versus pharmaceutical inhibitors, the trial evidence for arginine alone and in combination with pycnogenol, and the practical considerations for men incorporating amino acid supplementation into a broader ED management strategy.
Table of Contents
- The Physiology of Erection
- The NO-cGMP-PDE5 Axis
- How PDE5 Inhibitors Work
- Where Arginine Acts in the Pathway
- Clinical Trial Evidence for Arginine Alone
- Citrulline Trials in Erectile Dysfunction
- The Arginine + Pycnogenol Combination
- Arginine vs PDE5 Inhibitors
- PDE5 Non-Responder Rescue
- Practical Clinical Protocol
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
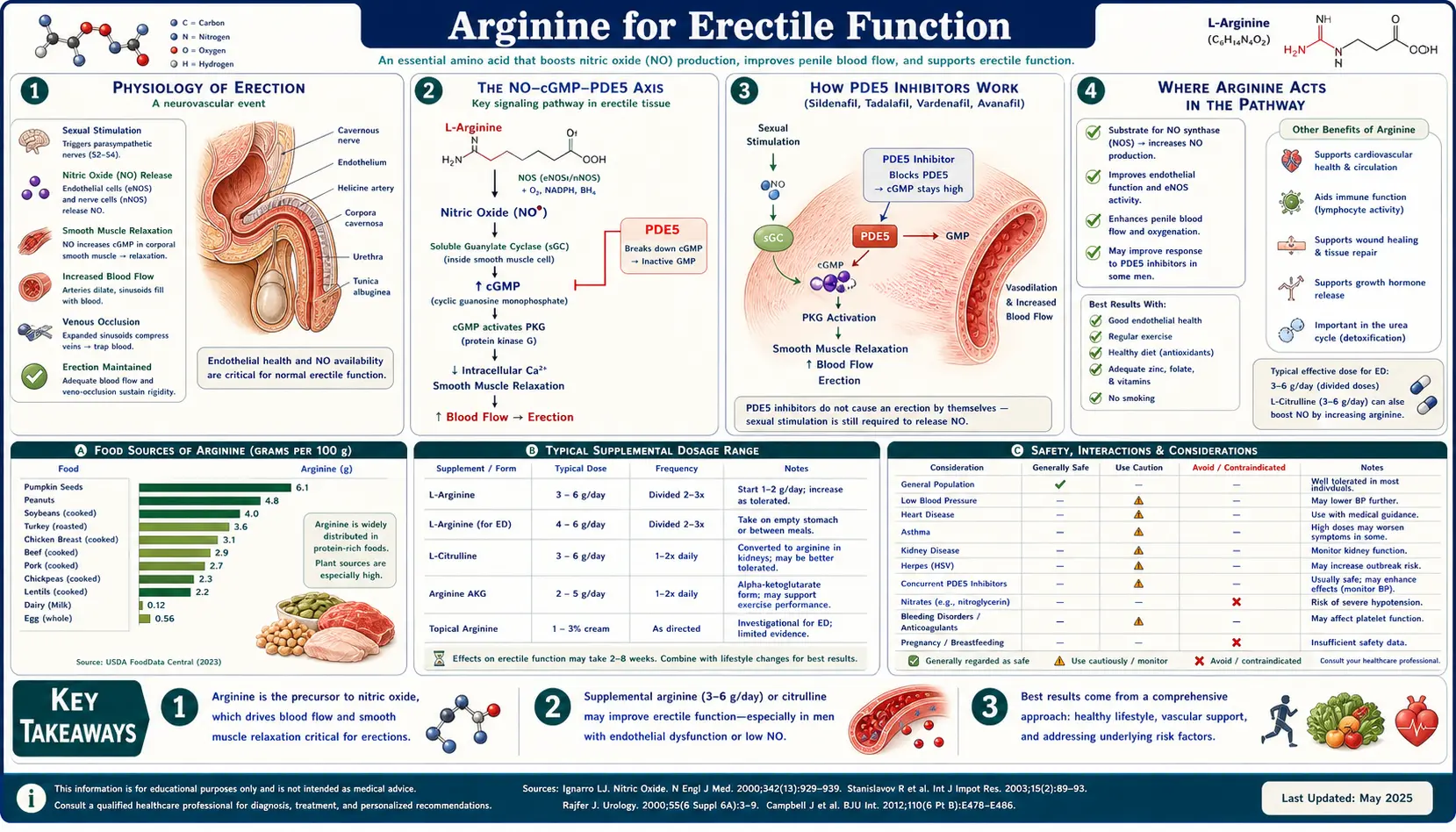
The Physiology of Erection
Penile erection results from increased arterial inflow to the corpus cavernosum combined with restricted venous outflow, producing engorgement of the erectile tissue with blood. The corpus cavernosum is a paired cylinder of vascular sinusoids surrounded by the tunica albuginea, a tough fibrous sheath. In the flaccid state, the arterial inflow to the cavernosum is restricted by tonic sympathetic vasoconstriction, and the sinusoids are largely empty. Erection requires three coordinated events:
- Sympathetic withdrawal and parasympathetic activation — sexual stimulation, either central (psychogenic) or peripheral (tactile via the dorsal penile nerve), triggers parasympathetic outflow via the pelvic splanchnic nerves and the cavernous nerves. These nerves release acetylcholine onto endothelial cells of the cavernosal sinusoids and noncholinergic, nonadrenergic (NANC) signals that release NO directly from neuronal terminals.
- NO release and smooth muscle relaxation — NO from both endothelial NOS3 (activated by acetylcholine and shear stress) and neuronal NOS1 (released directly from cavernous nerve terminals) diffuses into adjacent cavernosal smooth muscle. There it activates soluble guanylate cyclase, generating cGMP, which causes smooth muscle relaxation. Relaxed smooth muscle allows the sinusoids to fill with blood under arterial pressure.
- Venous restriction (the corporeal veno-occlusive mechanism) — as the sinusoids expand against the rigid tunica albuginea, the emissary veins that exit through the tunic are mechanically compressed, restricting venous outflow. The result is increased intracavernosal pressure approaching systemic arterial pressure, producing the rigidity characteristic of full erection.
The reverse process — detumescence — requires cGMP breakdown by phosphodiesterase type 5 (PDE5), which hydrolyzes cGMP to inactive 5'-GMP, allowing smooth muscle to return to its contracted baseline state and blood to drain from the sinusoids. This balance between NO/cGMP-driven relaxation and PDE5-driven cGMP breakdown is what determines erectile capacity at any given moment.
The NO-cGMP-PDE5 Axis
The molecular cascade that produces erection follows a well-defined four-step sequence:
- Substrate → Enzyme: L-arginine is the obligate substrate for nitric oxide synthase. The cavernosum expresses both NOS1 (in neurons) and NOS3 (in endothelium). Both convert arginine to citrulline and release NO.
- Enzyme → Signaling molecule: NO diffuses across cell membranes (it is a small, lipid-permeable, uncharged molecule), reaching smooth muscle cells without requiring a receptor.
- Signaling molecule → Second messenger: NO binds the heme group of soluble guanylate cyclase (sGC), activating it. sGC converts GTP to cGMP, the relaxant second messenger.
- Second messenger → Effect: cGMP activates protein kinase G (PKG), which phosphorylates targets including IP3 receptors, BKCa channels, and myosin light chain phosphatase. The net effect is reduced intracellular calcium and dephosphorylation of myosin, producing smooth muscle relaxation.
Each step in this cascade can be the rate-limiting bottleneck in different patients. In a young healthy man, the limiting step is typically the psychogenic trigger, not the biochemistry. In an older man with hypertension and diabetes, the limiting step shifts to NO production — endothelial dysfunction reduces NOS3 activity, BH4 cofactor depletion uncouples NOS, ADMA elevation competitively inhibits NOS, and the net NO release is insufficient to drive enough cGMP to overcome basal PDE5 activity. The result is partial or absent erection despite intact neural signaling and intact downstream machinery.
For more on the broader cardiovascular biology of NO and ADMA, see our Cardiovascular and NO deep-dive.
How PDE5 Inhibitors Work
Sildenafil (Viagra) was discovered serendipitously in the late 1980s during the development of a pulmonary hypertension drug by Pfizer's Sandwich, Kent research site. Male trial participants reported unexpected erections, and the indication was rapidly pivoted. The drug was approved by the FDA in 1998 and became the first oral pharmacological therapy for erectile dysfunction.
The mechanism is competitive inhibition of phosphodiesterase type 5, the enzyme that hydrolyzes cGMP to 5'-GMP. By inhibiting PDE5, sildenafil prolongs the half-life of cGMP in cavernosal smooth muscle, amplifying and prolonging the relaxation produced by any given pulse of NO release. The key insight is that PDE5 inhibitors do not produce erection in the absence of sexual stimulation — they require upstream NO release to have any cGMP to preserve. Take sildenafil and watch television: nothing happens. Take sildenafil and engage in sexual activity: the same NO release that previously produced an inadequate erection now produces a robust one, because the cGMP signal is no longer rapidly degraded.
The four major PDE5 inhibitors currently available differ in pharmacokinetics:
- Sildenafil — half-life 4 hours, onset 30–60 min, take on empty stomach
- Vardenafil — half-life 4–5 hours, similar onset, similar food interaction
- Tadalafil — half-life 17.5 hours, onset 30–120 min, food-independent, the "weekend pill" because of sustained activity
- Avanafil — half-life 5 hours, onset 15–30 min (fastest), food-independent
All four work through the same fundamental mechanism: prolongation of cGMP signaling downstream of arginine-derived NO. They cannot help patients whose NO production is so severely impaired that even prolonged cGMP signaling cannot overcome the baseline tone. This is the population most likely to benefit from arginine supplementation as a complement to or replacement for PDE5 inhibitors.
Where Arginine Acts in the Pathway
Arginine supplementation acts at step 1 of the cascade — the substrate input to NOS. Its mechanism is fundamentally different from PDE5 inhibitors:
- PDE5 inhibitors work downstream by preventing degradation of an already-produced cGMP signal. They require functional NO production to work.
- Arginine works upstream by providing substrate for NOS, increasing NO production at the source. It does not depend on functional PDE5 inhibition; the cGMP signal can still be rapidly degraded, but the amplitude of the initial NO pulse is higher.
The implication is that the two approaches are complementary, not redundant. A patient with severe endothelial dysfunction might fail to respond to PDE5 inhibitors because there is insufficient NO production to produce meaningful cGMP, even with prolonged half-life. The same patient might respond to arginine supplementation by raising NO production into a range where the cGMP signal is sufficient. And a patient who is a partial responder to either monotherapy may achieve full response to the combination of arginine plus PDE5 inhibition — more NO produced (arginine) and more cGMP preserved per NO molecule (PDE5 inhibitor).
Several smaller studies have specifically tested the arginine + PDE5 inhibitor combination and shown improved response rates in PDE5 partial responders, although large definitive trials have not yet been conducted. From a mechanistic standpoint, the combination is biochemically rational and is increasingly used in integrative urology practice.
Clinical Trial Evidence for Arginine Alone
The clinical trial literature on arginine monotherapy for erectile dysfunction is moderately positive but heterogeneous. The earliest controlled trial was by Chen et al. (1999), randomizing 50 men with organic ED to L-arginine 5 g/day or placebo for six weeks. 31% of the arginine group reported significant subjective improvement in sexual function versus 11% of the placebo group. The effect was concentrated in men with documented reduced urinary nitric oxide metabolites at baseline — precisely the population predicted to benefit from substrate supplementation.
Klotz et al. (1999) tested a lower dose (1.5 g/day) in 32 men with mixed-etiology ED and found no significant difference from placebo, suggesting the dose was sub-therapeutic. Subsequent trials have generally used 3–6 g/day, often divided into two or three daily doses.
Cormio et al. (2011) tested L-citrulline 1.5 g/day versus placebo in 24 men with mild ED. After one month, half of the citrulline group had improved to normal erectile function versus 8% of placebo. The citrulline dose was much lower than the typical arginine dose because of the superior bioavailability discussed in the Cardiovascular and NO page.
Meta-analysis of the arginine ED trials by Rhim et al. (2019), pooling 10 RCTs and over 540 patients, found that L-arginine doses in the range of 2.4–6 g/day produced significant improvement in IIEF (International Index of Erectile Function) scores compared with placebo, with effect sizes most prominent in mild and moderate ED. The improvement was less robust in severe ED, where adjunctive PDE5 inhibition is typically required.
The overall picture: arginine monotherapy at 3–6 g/day, or citrulline at 1.5–3 g/day, produces clinically meaningful benefit in mild to moderate erectile dysfunction in approximately 30–50% of treated men over 4–12 weeks. The benefit is concentrated in men with vasculogenic ED associated with endothelial dysfunction, diabetes, hypertension, or aging.
Citrulline Trials in Erectile Dysfunction
The citrulline literature is more recent than the arginine literature but is generally consistent with the broader pharmacological case for citrulline as the superior oral NO precursor. The key trials:
- Cormio et al. (2011) — L-citrulline 1.5 g/day vs placebo, 24 men, mild ED, 1-month duration. 50% of citrulline group improved to normal erectile function. Notable because the dose is much lower than typical arginine doses and the response rate matches or exceeds the larger arginine trials.
- Shirai et al. (2018) — L-citrulline plus resveratrol combination in men with mild ED. The combination produced larger improvements than placebo, with the resveratrol component thought to act through additional endothelial protective mechanisms.
- Lattuca et al. (2020) — longer-duration citrulline trial (3 months) showed sustained improvement in erectile function, suggesting the benefit is not transient.
Citrulline is typically dosed at 1.5–3 g per day for ED. Higher doses (6–8 g daily, divided) are used for athletic performance and severe peripheral vascular disease, but the lower dose is usually sufficient for the erectile indication because the cavernosal smooth muscle is exquisitely sensitive to NO at the relevant concentrations.
Citrulline is also better tolerated than arginine. Arginine doses above 5–10 g often cause gastrointestinal distress (nausea, cramping, diarrhea) due to the high osmotic load of the amino acid. Citrulline does not produce these effects at functional doses, making it the more practical option for daily long-term use.
The Arginine + Pycnogenol Combination
The most impressive results in the arginine ED literature have come from the combination of L-arginine with pycnogenol, a standardized extract of French maritime pine bark (Pinus pinaster) that is rich in oligomeric proanthocyanidins. Pycnogenol has multiple proposed mechanisms relevant to endothelial function: direct antioxidant activity (scavenging superoxide and protecting BH4 from oxidation), upregulation of eNOS expression, and modulation of inflammatory cytokines that contribute to endothelial dysfunction.
The pivotal trial was by Stanislavov and Nikolova (2003), published in the Journal of Sex and Marital Therapy. Forty men with confirmed erectile dysfunction were treated with L-arginine 1.7 g/day for the first month, then L-arginine 1.7 g + pycnogenol 40 mg twice daily for the second month, then L-arginine 1.7 g + pycnogenol 40 mg three times daily for the third month. Erectile function was assessed monthly using a self-report rating of intercourse satisfaction.
The results:
- After arginine alone (month 1): 5% of participants reported normal erectile function
- After arginine + pycnogenol 80 mg/day (month 2): 80% reported normal erectile function
- After arginine + pycnogenol 120 mg/day (month 3): 92.5% reported normal erectile function
The placebo-controlled follow-up by Stanislavov, Rohdewald, and others have generally replicated the finding that pycnogenol dramatically potentiates the modest effect of arginine alone. The proposed mechanism is that pycnogenol's antioxidant activity protects the BH4 cofactor and prevents NOS uncoupling, allowing the supplemental arginine substrate to be efficiently converted to NO rather than to superoxide.
The commercial formulation marketed as "Prelox" combines L-arginine aspartate with pycnogenol in a fixed-dose tablet and has been studied in several additional trials, generally confirming the benefit. The cost is substantially lower than chronic PDE5 inhibitor use, and the safety profile is excellent.
For men with mild to moderate vasculogenic ED, the arginine + pycnogenol combination is one of the most evidence-based non-prescription options available, with response rates approaching those of low-dose PDE5 inhibitors.
Arginine vs PDE5 Inhibitors
A practical comparison between arginine-based therapy and PDE5 inhibitors:
- Onset of action — PDE5 inhibitors work within 30–60 minutes of a single dose. Arginine requires weeks of daily dosing to produce maximal benefit, because the mechanism is repletion of endothelial substrate and gradual restoration of NOS function, not acute pharmacological inhibition.
- Duration of effect — PDE5 inhibitor effect is limited to the drug's half-life (4 hours for sildenafil/vardenafil/avanafil, 17.5 hours for tadalafil). Arginine produces sustained background improvement in endothelial NO production, with no on-demand timing required.
- Response rate in moderate ED — PDE5 inhibitors approximately 70%; arginine + pycnogenol approximately 80–90% in some trials; arginine alone approximately 30–50%.
- Response rate in severe ED — PDE5 inhibitors approximately 50–60%; arginine likely less effective as monotherapy; combination may improve response.
- Side effects — PDE5 inhibitors: headache, flushing, dyspepsia, visual disturbances, rare hearing loss, priapism. Arginine: GI distress at high doses, potential herpes outbreak triggering. Citrulline: minimal.
- Drug interactions — PDE5 inhibitors: absolute contraindication with nitrates (severe hypotension); caution with alpha blockers. Arginine: potentiation of antihypertensives, theoretical interaction with nitrates.
- Cost — PDE5 inhibitors $5–$30 per dose (generic sildenafil now $2–$5 per dose). Arginine + pycnogenol approximately $30–$50 per month.
- Underlying disease addressing — PDE5 inhibitors are symptomatic; they do not address the underlying endothelial dysfunction. Arginine and citrulline aim to improve the underlying vascular biology.
For most men with mild to moderate ED, particularly when ED is part of a broader pattern of cardiovascular risk (the recognition of ED as a predictor of coronary disease has become well-established), arginine-based therapy as either primary intervention or PDE5 adjunct makes physiologic sense.
PDE5 Non-Responder Rescue
Approximately 25–35% of men do not respond adequately to first-line PDE5 inhibitor therapy. The non-responder population is enriched for severe endothelial dysfunction, diabetes, post-prostatectomy nerve injury, and advanced cardiovascular disease. Several mechanisms can underlie non-response:
- Insufficient NO production to generate enough cGMP for PDE5 inhibition to amplify
- Cavernosal smooth muscle structural changes that reduce responsiveness to cGMP
- Nerve damage that prevents adequate parasympathetic NO release
- Sub-therapeutic dosing or improper administration timing
For non-responders driven primarily by low NO production (the first mechanism), arginine supplementation can sometimes convert non-responders to responders. The clinical approach: switch from arginine to higher-dose citrulline (3–6 g/day) for 8–12 weeks, then re-trial PDE5 inhibitor at maximum tolerated dose. Several small case series have shown 20–40% of prior non-responders achieve adequate response with the addition of citrulline.
For mechanisms 2–4, arginine is unlikely to help, and second-line therapies (intracavernosal injection of alprostadil, vacuum erection device, penile prosthesis) become the appropriate next step. The role of arginine is specifically in patients with reversible endothelial dysfunction as the rate-limiting bottleneck.
Practical Clinical Protocol
A defensible clinical approach for men with vasculogenic erectile dysfunction:
- Cardiovascular workup first — ED in men over 40 is a recognized predictor of coronary disease, with average lead time of approximately 3–5 years before a cardiovascular event. Anyone presenting with new ED should have full cardiovascular risk assessment including blood pressure, lipid panel, fasting glucose, HbA1c, and consideration of carotid ultrasound or other vascular imaging.
- Lifestyle interventions — exercise (particularly aerobic exercise that improves endothelial function), weight loss if obese, smoking cessation, Mediterranean diet, and treatment of hypertension and dyslipidemia. These foundational interventions improve ED in their own right.
- First-line supplement — L-citrulline 1.5–3 g/day, taken in the morning, for at least 8 weeks. Better tolerated and biochemically superior to L-arginine for most patients.
- Combination upgrade — if response is partial, add pycnogenol 120–180 mg/day or use a combination product (Prelox or equivalent). Continue for another 8 weeks.
- PDE5 inhibitor addition — if further improvement is needed, add a PDE5 inhibitor (sildenafil 25–100 mg or tadalafil 5–20 mg) at the prescriber's discretion. Continue the citrulline + pycnogenol background therapy.
- Specialist referral — for non-response despite optimized combination therapy, urological evaluation for nerve injury, structural pathology, or second-line interventions.
For more on erectile dysfunction as a clinical entity, see our Erectile Dysfunction page.
Cautions and Drug Interactions
- Nitrate medications — nitroglycerin, isosorbide, and any other organic nitrate produces NO directly. Combined with arginine and especially with PDE5 inhibitors, this can produce severe hypotension. Patients with stable angina who use nitrates should not combine high-dose arginine with PDE5 inhibitors. Most clinicians will recommend a 24–48 hour washout between nitrate and PDE5 use.
- Concurrent PDE5 inhibitors — the combination is biochemically rational but can produce additive hypotensive effects. Start with lower doses of both and titrate to effect.
- Alpha-blockers (for benign prostatic hyperplasia) — tamsulosin, doxazosin, and similar drugs can interact with PDE5 inhibitors (and to a lesser extent with arginine) to produce orthostatic hypotension. Patient education and careful timing are required.
- Active herpes simplex infection — arginine supports HSV replication. Men with frequent oral or genital herpes outbreaks may want to use citrulline preferentially (which produces less of a plasma spike) and add lysine 1–2 g/day as a counterbalance. See L-Lysine.
- Recent myocardial infarction (within 6 months) — based on the VINTAGE-MI signal discussed on the Cardiovascular page, high-dose arginine should be avoided in the post-MI period. PDE5 inhibitor use post-MI is also restricted and requires cardiology clearance.
- Severe hypertension or unstable angina — ED treatment of any kind in a man with poorly controlled cardiovascular disease should be deferred until the underlying condition is stabilized.
Key Research Papers
- Chen J et al. (1999). Effect of oral administration of high-dose nitric oxide donor L-arginine in men with organic erectile dysfunction: results of a double-blind, randomized, placebo-controlled study. BJU International. — PubMed
- Stanislavov R, Nikolova V (2003). Treatment of erectile dysfunction with pycnogenol and L-arginine. Journal of Sex and Marital Therapy. — PubMed
- Cormio L et al. (2011). Oral L-citrulline supplementation improves erection hardness in men with mild erectile dysfunction. Urology. — PubMed
- Rhim HC et al. (2019). The potential role of arginine supplements on erectile dysfunction: a systemic review and meta-analysis. Journal of Sexual Medicine. — PubMed
- Burnett AL (2006). The role of nitric oxide in erectile dysfunction: implications for medical therapy. Journal of Clinical Hypertension. — PubMed
- Goldstein I et al. (1998). Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. NEJM. — PubMed
- Klotz T et al. (1999). Effectiveness of oral L-arginine in first-line treatment of erectile dysfunction in a controlled crossover study. Urologia Internationalis. — PubMed
- Aoki H et al. (2012). Clinical assessment of a supplement of Pycnogenol and L-arginine in Japanese patients with mild to moderate erectile dysfunction. Phytotherapy Research. — PubMed
- Ledda A et al. (2010). Investigation of a complex plant extract for mild to moderate erectile dysfunction in a randomized, double-blind, placebo-controlled, parallel-arm study. BJU International. — PubMed
- Andersson KE, Wagner G (1995). Physiology of penile erection. Physiological Reviews. — PubMed
- Toda N et al. (2005). Nitric oxide and penile erectile function. Pharmacology and Therapeutics. — PubMed
- Shamloul R, Ghanem H (2013). Erectile dysfunction. The Lancet. — PubMed
- Hackett G et al. (2018). British Society for Sexual Medicine guidelines on the management of erectile dysfunction in men: 2017. Journal of Sexual Medicine. — PubMed
PubMed Topic Searches
- PubMed: L-arginine and ED
- PubMed: L-citrulline and ED
- PubMed: Pycnogenol + arginine
- PubMed: NO-cGMP-PDE5 axis
- PubMed: Sildenafil and endothelial function
Connections
- Arginine Overview
- Arginine Benefits Hub
- Arginine for Cardiovascular Health
- Arginine for Wound Healing
- Arginine for Immune Function
- Erectile Dysfunction
- Cardiovascular Disease
- Hypertension
- Diabetes
- Metabolic Syndrome
- Lysine
- Lysine
- Taurine
- All Amino Acids
- Kidney Function
- Citrulline — the alternative NO precursor that worked at a fraction of the arginine dose.