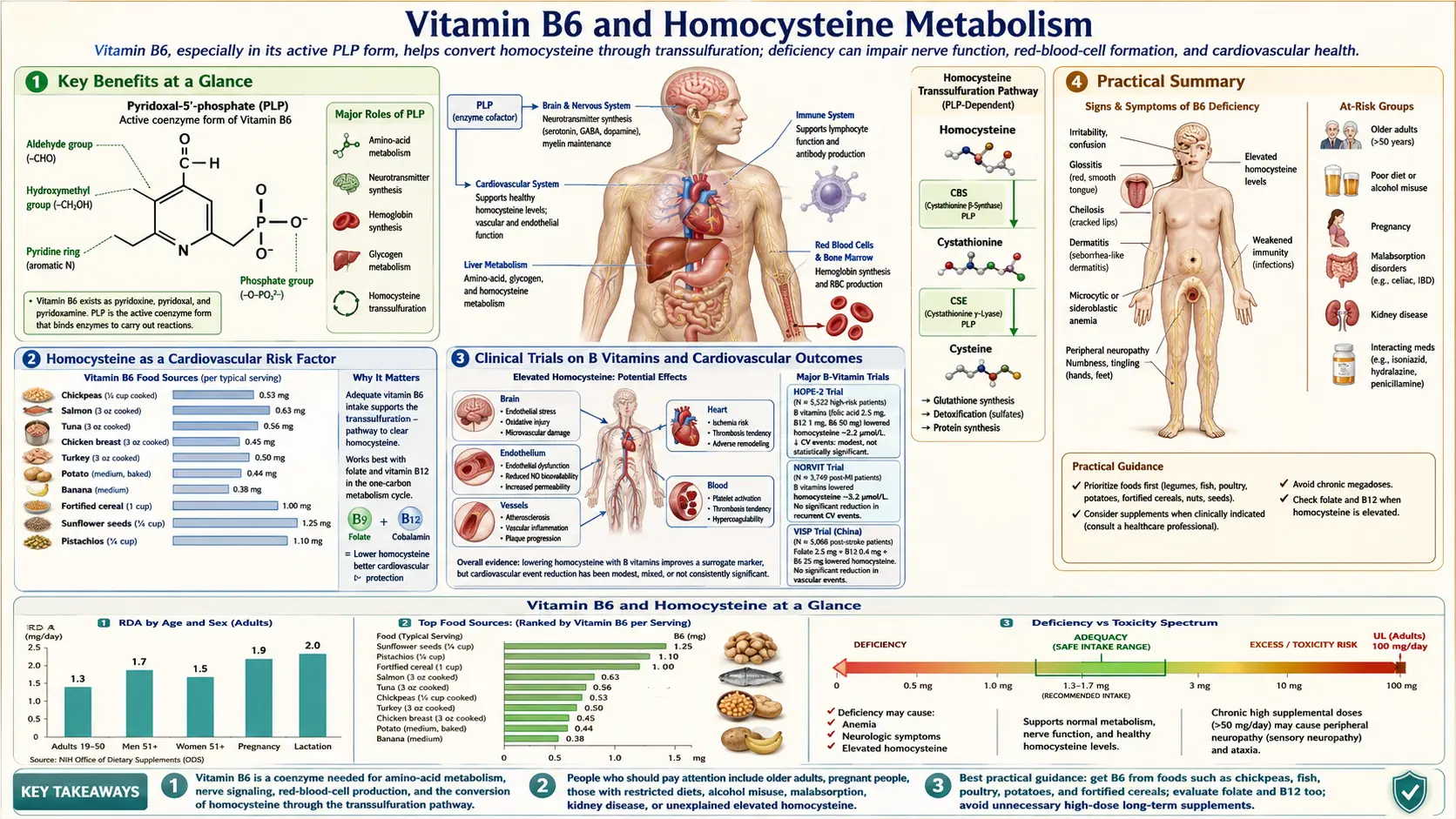
Vitamin B6 and Homocysteine Metabolism
Homocysteine is a sulfur-containing amino acid formed as an intermediate in the metabolism of methionine, an essential amino acid obtained from dietary protein. While homocysteine itself serves no known physiological function, its levels in the blood have emerged as an important biomarker for cardiovascular risk, cerebrovascular disease, and nutritional status. Vitamin B6, in its active form pyridoxal 5'-phosphate (PLP), is one of three B vitamins — along with vitamin B12 and folate — that are required for the efficient clearance of homocysteine from the body.
Table of Contents
- Key Benefits at a Glance
- The Transsulfuration Pathway
- PLP as Cofactor: Mechanism of Action
- Homocysteine as a Cardiovascular Risk Factor
- Endothelial Damage Mechanism
- Synergy with B12 and Folate: The Remethylation Pathway
- MTHFR Considerations
- Clinical Trials on B Vitamins and Cardiovascular Outcomes
- Target Homocysteine Levels
- Testing and Treatment
- Practical Summary
- Research Papers
- Connections
- Featured Videos
Key Benefits at a Glance
- PLP (active B6) is the cofactor for both CBS and CGL in the transsulfuration pathway.
- Enables irreversible clearance of homocysteine through cysteine synthesis.
- Synergizes with B12 and folate in remethylation of homocysteine to methionine.
- Homocysteine above ~10 µmol/L is associated with increased cardiovascular and stroke risk.
- VISP, HOPE-2, and VITATOPS trials show consistent homocysteine lowering with B-vitamin therapy.
- Stroke risk reduction is the most consistent outcome signal from B-vitamin RCTs.
- Target homocysteine <10 µmol/L for general adults; <8 µmol/L for high-risk.
- Doses of 25–50 mg/day P5P or pyridoxine with B12 and folate effectively normalize levels.
The Transsulfuration Pathway
The transsulfuration pathway is the primary route by which homocysteine is irreversibly catabolized, and it is entirely dependent on vitamin B6:
Cystathionine Beta-Synthase (CBS)
- Reaction — CBS catalyzes the condensation of homocysteine with serine to form cystathionine, a reaction that requires PLP as an essential cofactor. This is the first and committed step of the transsulfuration pathway.
- Enzyme characteristics — CBS is a heme-containing enzyme that binds PLP at its active site. The heme moiety serves as a redox sensor, while PLP participates directly in the catalytic mechanism through Schiff base chemistry with the amino acid substrates.
- Regulation — CBS activity is allosterically activated by S-adenosylmethionine (SAM), the universal methyl donor. When SAM levels are high (indicating adequate methylation capacity), CBS is activated to divert homocysteine toward irreversible catabolism rather than remethylation to methionine.
- Genetic deficiency — homozygous CBS deficiency is the most common cause of classical homocystinuria, characterized by plasma homocysteine levels exceeding 100 micromoles per liter and severe clinical manifestations including lens dislocation, skeletal abnormalities, intellectual disability, and premature thromboembolic disease. Approximately 50 percent of patients with CBS deficiency respond to high-dose pyridoxine therapy (200 to 1,000 mg daily), which enhances residual CBS activity.
Cystathionine Gamma-Lyase (CGL)
- Reaction — CGL cleaves cystathionine to produce cysteine, alpha-ketobutyrate, and ammonia. Like CBS, CGL requires PLP as a cofactor.
- Downstream products — the cysteine generated by this pathway is used for glutathione synthesis (the body's primary intracellular antioxidant), taurine synthesis, and incorporation into proteins. The alpha-ketobutyrate enters the propionyl-CoA pathway and is ultimately oxidized for energy.
- Double PLP dependency — because both sequential enzymes of the transsulfuration pathway (CBS and CGL) require PLP, vitamin B6 deficiency has a particularly pronounced effect on this route of homocysteine disposal.
PLP as Cofactor: Mechanism of Action
Understanding how PLP functions in the transsulfuration pathway illuminates why B6 status is so critical for homocysteine metabolism:
- Schiff base formation — PLP binds to the epsilon-amino group of a lysine residue in the enzyme active site, forming an internal aldimine (Schiff base). When substrate enters the active site, a transaldimination occurs: the substrate's amino group displaces the lysine to form an external aldimine with PLP.
- Electron sink function — the pyridinium ring of PLP acts as an electron sink, stabilizing carbanion intermediates that form during the catalytic cycle. This electron-withdrawing capacity is what makes PLP such a versatile cofactor for reactions involving amino acid transformations.
- Reaction specificity — although PLP chemistry can theoretically support multiple reaction types (transamination, decarboxylation, elimination, racemization), each PLP-dependent enzyme controls which bond is broken through the precise orientation of the substrate-PLP complex within the active site.
- Cofactor saturation — in B6-replete individuals, CBS and CGL are fully saturated with PLP. As B6 status declines, the proportion of apo-enzyme (without PLP bound) increases, reducing catalytic capacity and allowing homocysteine to accumulate.
Homocysteine as a Cardiovascular Risk Factor
Elevated plasma homocysteine (hyperhomocysteinemia) has been established as an independent risk factor for cardiovascular disease through extensive epidemiological evidence:
- Risk gradient — meta-analyses of prospective studies indicate that each 5 micromole per liter increase in plasma homocysteine is associated with approximately a 20 percent increase in coronary heart disease risk and a 50 percent increase in cerebrovascular disease risk, independent of traditional risk factors.
- Classification of hyperhomocysteinemia — mild elevation is defined as 12 to 30 micromoles per liter, moderate as 30 to 100 micromoles per liter, and severe as above 100 micromoles per liter. Mild hyperhomocysteinemia affects an estimated 5 to 10 percent of the general population and a higher proportion of elderly individuals.
- Venous thromboembolism — elevated homocysteine is also associated with increased risk of deep vein thrombosis and pulmonary embolism, with a pooled odds ratio of approximately 2.5 for homocysteine levels above the 95th percentile.
- Peripheral arterial disease — hyperhomocysteinemia is prevalent among patients with peripheral arterial disease, and elevated levels predict disease progression and adverse limb outcomes.
Endothelial Damage Mechanism
The vascular toxicity of homocysteine operates through multiple interacting mechanisms that damage the endothelium and promote atherosclerosis:
- Oxidative stress — homocysteine undergoes auto-oxidation in plasma, generating reactive oxygen species (ROS) including superoxide anion, hydrogen peroxide, and hydroxyl radicals. The sulfhydryl group of homocysteine can also react with metal ions to generate oxidative stress through Fenton chemistry.
- Nitric oxide impairment — homocysteine reduces endothelial nitric oxide bioavailability through multiple mechanisms: direct chemical inactivation of NO, uncoupling of endothelial nitric oxide synthase (eNOS) by oxidizing its cofactor tetrahydrobiopterin (BH4), and inhibiting eNOS expression. The resulting endothelial dysfunction impairs vasodilation and promotes vasoconstriction.
- Endoplasmic reticulum stress — homocysteine induces the unfolded protein response (UPR) in endothelial cells, leading to endoplasmic reticulum stress, activation of pro-apoptotic pathways, and endothelial cell death.
- Pro-inflammatory effects — homocysteine activates NF-kappa-B signaling in endothelial cells, upregulating expression of adhesion molecules (VCAM-1, ICAM-1, E-selectin) and chemokines (MCP-1) that recruit inflammatory cells to the vessel wall, initiating and propagating the atherosclerotic process.
- Smooth muscle cell proliferation — homocysteine stimulates vascular smooth muscle cell proliferation and collagen synthesis, contributing to intimal thickening and arterial stiffness.
- Thrombogenic effects — homocysteine activates tissue factor expression, inhibits thrombomodulin and protein C activation, reduces heparan sulfate proteoglycan expression, and impairs fibrinolysis by increasing plasminogen activator inhibitor-1 (PAI-1) levels. These effects collectively shift the hemostatic balance toward a prothrombotic state.
Synergy with B12 and Folate: The Remethylation Pathway
While vitamin B6 operates in the transsulfuration pathway, vitamins B12 and folate control the alternative route of homocysteine disposal — remethylation back to methionine:
- Methionine synthase reaction — this B12-dependent enzyme transfers a methyl group from 5-methyltetrahydrofolate (5-MTHF) to homocysteine, regenerating methionine and tetrahydrofolate (THF). This reaction simultaneously requires both vitamin B12 (as methylcobalamin) and folate (as 5-MTHF).
- MTHFR and 5-MTHF generation — methylenetetrahydrofolate reductase (MTHFR) converts 5,10-methylenetetrahydrofolate to 5-MTHF, the form of folate required for homocysteine remethylation. This enzyme uses FAD (riboflavin/B2-derived) as a cofactor, adding another B vitamin to the homocysteine regulation network.
- Complementary pathways — the remethylation and transsulfuration pathways serve complementary functions. Remethylation conserves methionine when methionine intake is low, while transsulfuration disposes of excess homocysteine when methionine intake is high. Both pathways must function adequately for optimal homocysteine homeostasis.
- Triple B vitamin approach — because deficiency of any single B vitamin (B6, B12, or folate) can cause hyperhomocysteinemia, effective treatment typically involves assessing and addressing the status of all three. Supplementation with only one vitamin when another is deficient may provide an incomplete response.
MTHFR Considerations
Genetic variations in the MTHFR gene have important implications for homocysteine metabolism and the relative importance of B6-dependent pathways:
- C677T polymorphism — this common variant (carried by approximately 10 to 15 percent of the population in homozygous form) produces a thermolabile enzyme with approximately 30 percent of normal activity at 37 degrees Celsius. Homozygous carriers (TT genotype) have mildly elevated homocysteine levels, particularly when folate status is low.
- A1298C polymorphism — this variant also reduces MTHFR activity, though to a lesser extent than C677T. Compound heterozygosity (one copy of each variant) produces a phenotype similar to C677T homozygosity.
- Implications for B6 therapy — in individuals with impaired MTHFR activity, the remethylation pathway is compromised, making the B6-dependent transsulfuration pathway relatively more important for homocysteine clearance. Ensuring optimal B6 status in MTHFR variant carriers may partially compensate for reduced remethylation capacity.
- Folate form considerations — individuals with MTHFR variants may benefit from supplementation with 5-methyltetrahydrofolate (5-MTHF, also called methylfolate or L-methylfolate) rather than folic acid, as they have reduced ability to convert folic acid to the active 5-MTHF form. This is relevant because adequate 5-MTHF availability reduces the burden on the transsulfuration pathway.
Clinical Trials on B Vitamins and Cardiovascular Outcomes
Despite the strong epidemiological association between homocysteine and cardiovascular disease, clinical trials of B vitamin supplementation to lower homocysteine have produced mixed results:
- HOPE-2 Trial — this large randomized trial (5,522 patients with vascular disease or diabetes) found that supplementation with folic acid, B6, and B12 for 5 years significantly lowered homocysteine but did not reduce the primary composite outcome of cardiovascular death, myocardial infarction, or stroke. However, a significant 25 percent reduction in stroke risk was observed.
- VISP Trial — the Vitamin Intervention for Stroke Prevention trial found no significant difference in recurrent stroke, MI, or death between high-dose and low-dose B vitamin supplementation in patients with recent stroke, though the lack of a true placebo group limited interpretation.
- NORVIT Trial — this Norwegian trial found no benefit of B vitamin supplementation after myocardial infarction, and a combination of folic acid, B6, and B12 showed a trend toward increased cardiovascular events, raising concerns about potential harm.
- Meta-analyses — pooled analyses of homocysteine-lowering trials consistently show a significant reduction in stroke risk (approximately 10 to 25 percent) with B vitamin supplementation, but no significant reduction in coronary events or overall cardiovascular mortality.
- Interpretation — the discrepancy between epidemiological data and trial results has led to debate about whether homocysteine is a causal risk factor or merely a marker of underlying nutritional or metabolic derangement. The current consensus is that correcting B vitamin deficiency is important for multiple health reasons, but high-dose B vitamin supplementation solely to lower homocysteine is not justified as a cardiovascular prevention strategy in the general population.
Target Homocysteine Levels
While there is no universally agreed-upon optimal homocysteine level, the following thresholds are commonly used in clinical practice:
- Optimal range — less than 10 micromoles per liter. Some researchers advocate for levels below 8 micromoles per liter for maximal vascular protection, though the evidence base for this more aggressive target is limited.
- Normal range — 5 to 15 micromoles per liter, as defined by most clinical laboratories. This wide range may include levels associated with increased cardiovascular risk.
- Mild hyperhomocysteinemia — 15 to 30 micromoles per liter. This range warrants investigation for underlying causes (B6, B12, or folate deficiency, renal insufficiency, hypothyroidism) and nutritional intervention.
- Moderate hyperhomocysteinemia — 30 to 100 micromoles per liter. This range suggests a more significant metabolic disturbance and requires thorough evaluation including consideration of genetic enzyme deficiencies.
- Severe hyperhomocysteinemia — above 100 micromoles per liter. This level is typically seen only in classical homocystinuria (CBS deficiency) or severe combined B vitamin deficiency and requires specialist evaluation and treatment.
Testing and Treatment
When to Test Homocysteine
- Premature cardiovascular disease — testing is reasonable in patients with coronary artery disease, stroke, or peripheral arterial disease at younger ages (men under 55, women under 65) without traditional risk factors.
- Unexplained thromboembolic disease — homocysteine testing is part of the evaluation for thrombophilia in patients with unexplained venous or arterial thrombosis.
- Family history of homocystinuria — siblings and children of individuals with CBS deficiency should be screened.
- Suspected B vitamin deficiency — homocysteine serves as a functional marker of B6, B12, and folate status and may be elevated before classic hematologic abnormalities appear.
- Chronic kidney disease — renal impairment reduces homocysteine clearance, and levels are commonly elevated in patients with advanced CKD.
Treatment Approach
- Dietary optimization — increasing intake of foods rich in B6 (poultry, fish, potatoes, chickpeas), B12 (animal products, fortified foods), and folate (dark leafy greens, legumes, fortified grains) is the first-line approach for mild hyperhomocysteinemia.
- B vitamin supplementation — for persistent elevation despite dietary changes, supplementation with folic acid (400 to 1,000 mcg), vitamin B12 (500 to 1,000 mcg), and vitamin B6 (25 to 50 mg) daily is typically effective at normalizing homocysteine levels within 4 to 8 weeks.
- Addressing underlying causes — hypothyroidism, renal insufficiency, and medications (methotrexate, anticonvulsants, metformin, nitrous oxide) that interfere with B vitamin metabolism or homocysteine clearance should be identified and managed.
- Monitoring — repeat homocysteine testing 2 to 3 months after initiating treatment confirms adequacy of response. Persistent elevation despite supplementation suggests a genetic enzyme defect, poor compliance, or an unaddressed secondary cause.
- Pyridoxine-responsive homocystinuria — patients with CBS deficiency who respond to pyridoxine require lifelong high-dose B6 supplementation (typically 200 to 500 mg daily), combined with dietary methionine restriction and betaine supplementation for optimal homocysteine control.
Practical Summary
- Vitamin B6 is essential for the irreversible disposal of homocysteine through the transsulfuration pathway, with PLP serving as the cofactor for both CBS and CGL.
- B6 works in concert with B12 and folate to maintain homocysteine homeostasis; all three vitamins should be assessed when hyperhomocysteinemia is identified.
- Elevated homocysteine is associated with increased cardiovascular and cerebrovascular risk, though the causal nature of this relationship remains debated.
- Correcting B vitamin deficiency effectively lowers homocysteine and is recommended for individuals with documented deficiency, but routine high-dose supplementation for cardiovascular prevention in B vitamin-replete individuals is not supported by current trial evidence.
- MTHFR variant carriers may benefit from particular attention to both folate form (methylfolate vs. folic acid) and adequate B6 intake to support the transsulfuration pathway as a compensatory route for homocysteine clearance.
Research Papers
- Toole JF, et al. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke (VISP). (PubMed topic search)
- HOPE-2 Investigators. Homocysteine lowering with folic acid and B vitamins in vascular disease. (PubMed topic search)
- VITATOPS Trial Study Group. B vitamins in patients with recent transient ischaemic attack or stroke. (PubMed topic search)
- PubMed — Homocysteine and endothelial dysfunction (topic search)
- PubMed — Transsulfuration pathway and PLP (topic search)
- PubMed — Homocysteine and cardiovascular risk meta-analyses (topic search)
- PubMed — B vitamins and stroke prevention meta-analyses (topic search)
- PubMed — Cystathionine beta-synthase deficiency (topic search)
- PubMed — MTHFR C677T and homocysteine (topic search)
- NIH Office of Dietary Supplements — Vitamin B6 Fact Sheet for Health Professionals
- Linus Pauling Institute — Vitamin B6
- Harvard T.H. Chan School of Public Health — Vitamin B6
Connections
- All Vitamins
- Vitamin B6
- Pyridoxine and Brain Health
- Vitamin B12
- B12 Deficiency Diagnosis
- Vitamin B9
- Folate and Mental Health
- Homocysteine
- Methionine
- Cysteine
- Cardiovascular Disease
- Stroke
- Atherosclerosis
- Inflammatory Markers
- Magnesium
- Vitamin B12 Test
- Folate and Pregnancy
- Niacin and Cholesterol