Vitamin A Deficiency: Poor Growth and Child Mortality
Of all the ways a vitamin can matter, this is the most sobering: in young children, a lack of vitamin A does not just cause symptoms — it shortens lives. A child who is mildly deficient looks healthy. Then an ordinary bout of measles, diarrhea, or a chest infection that a well-nourished child would shrug off becomes, for the deficient child, far more likely to be fatal. Across dozens of low-income countries, giving children two cheap high-dose vitamin A capsules a year cuts their risk of dying by roughly a fifth. This page explains how a missing vitamin slows a child's growth and, more importantly, why it tilts the odds of survival — and it is honest that vitamin A is one cause of poor growth among several, not the whole story.
Table of Contents
- What This Looks Like in a Child
- The Mechanism: Why a Missing Vitamin Costs Lives
- Honesty: Vitamin A Is One Cause of Poor Growth, Not the Only One
- When Poor Growth Points Toward Vitamin A
- The Global Scale of the Problem
- What Causes Vitamin A Deficiency in Children
- Diagnosis and Measurement
- Correcting and Preventing It
- Red Flags / When to Seek Care
- Key Research Papers
- Connections
- Featured Videos
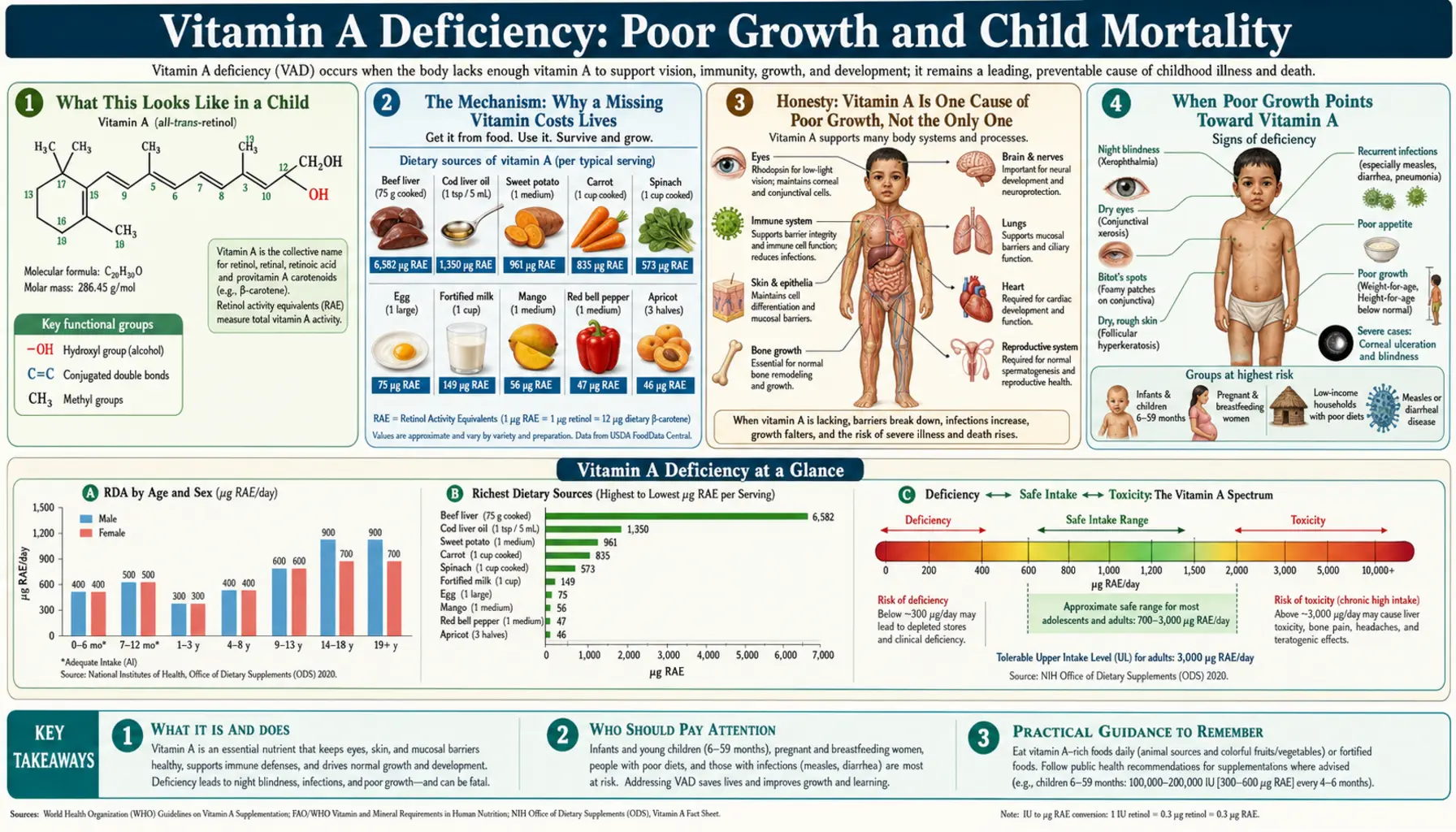
What This Looks Like in a Child
Vitamin A deficiency severe enough to threaten a child's life often does not announce itself dramatically. The earliest and most specific sign is in the eyes — night blindness, where a toddler stops finding their way around at dusk or bumps into things in dim light, and the white of the eye develops dry, foamy patches called Bitot's spots (covered in detail on the sibling page, Night Blindness and Eye Damage). But long before the eyes are affected, a subtler picture is unfolding in the rest of the body.
For growth and survival, the warning signs caregivers and clinicians tend to notice are:
- Faltering growth — a child who slips downward across the lines on a growth chart, gaining height and weight more slowly than expected for their age. This is often stunting (being short for one's age), the visible mark of chronic undernutrition.
- Frequent, severe, slow-to-clear infections — repeated bouts of diarrhea, recurrent chest infections, and illnesses (especially measles) that hit harder and last longer than in other children. This is the single most important feature, because it is the pathway to death.
- Dry, rough, “goosebump” skin — the same keratin build-up that affects the eye also roughens the skin (see Skin Problems and Hyperkeratosis).
- Poor appetite and apathy — a flagging interest in food and play that both worsens undernutrition and is worsened by it, creating a downward spiral.
The cruel feature of this condition is that the child who is at greatest risk often looks only mildly unwell. A toddler can have subclinical vitamin A deficiency — low body stores, no obvious eye signs — and still carry a substantially higher risk of dying from their next common infection. That gap between “looks mostly fine” and “is in real danger” is exactly why population-wide supplementation, rather than waiting for symptoms, became the global strategy.
The Mechanism: Why a Missing Vitamin Costs Lives
To understand how a lack of vitamin A both slows growth and raises the risk of death, it helps to know what the vitamin actually does. Vitamin A's active forms — chiefly retinoic acid — act like a master switch inside cells. Retinoic acid binds to receptors on the DNA and turns whole sets of genes on or off, governing how cells grow, specialize, and renew. Two of those programs matter enormously here: building and maintaining barrier surfaces (the linings of the gut, lungs, and eyes, and the skin) and running the immune system.
The growth side. Vitamin A directly supports the formation and turning-over of the rapidly dividing cells that a growing body depends on, and it helps shape the cartilage and bone that lengthen a child's skeleton. Just as important, it keeps the gut lining healthy — and a healthy gut lining is what lets a child absorb the calories and nutrients in their food. When the lining is damaged, food passes through poorly absorbed, so even a fed child can be under-nourished. Deficiency also tends to travel with other shortfalls (protein, zinc, iron), so the growth penalty is rarely from vitamin A alone — a point the honesty section below returns to.
The survival side — the bigger story. The reason vitamin A deficiency is lethal is not the eye disease and not the stunting in themselves; it is the collapse of the body's defenses. Vitamin A is essential for keeping the epithelial barriers intact — the moist linings of the gut and airways that form the body's first wall against germs. When vitamin A runs low, these linings dry out, lose their protective mucus, and break down, so bacteria and viruses get in more easily. Behind that wall, vitamin A is also required to run the immune system itself: it supports the production and function of the white blood cells that fight infection and helps direct the response of T-cells and antibody-producing cells. A deficient child therefore faces a double hit — the gate is open and the soldiers are fewer and less coordinated. (The immune mechanism is detailed on the sibling page Weakened Immunity and Infections and on Vitamin A and Immune Function.)
There is a vicious cycle on top of this. Infection itself drains vitamin A — a child with measles or severe diarrhea loses vitamin A in the urine and through the damaged gut, so an illness can tip a borderline child into outright deficiency, which then makes the next illness worse. This is why measles and vitamin A are so tightly linked: measles both depletes vitamin A and is far deadlier in children who are already short of it. The World Health Organization recommends vitamin A treatment for children with measles in areas where deficiency is a problem precisely because it reduces deaths and complications.
An analogy. Picture a walled town in a region where raiders pass through regularly. Vitamin A does two jobs: it keeps the town wall in good repair, and it pays and trains the garrison inside. A well-supplied town survives a raid with a few losses and rebuilds. A town that has run out of vitamin A has a crumbling wall and too few, poorly-led guards — so the same raid that the neighboring town shrugs off can overrun it. The raider here is an everyday childhood infection: measles, a diarrheal bug, a chest infection. None of them is exotic. What changes the outcome is whether the child's defenses were funded — and two cents of vitamin A a year is, astonishingly, enough to fund them.
Honesty: Vitamin A Is One Cause of Poor Growth, Not the Only One
It would be misleading to tell a parent that a child growing poorly is “low on vitamin A.” Stunting and faltering growth are final common pathways — the end result of many overlapping causes — and vitamin A is only one contributor, often not the dominant one. Being honest about this matters, because it changes what actually helps a child.
The major drivers of poor growth in young children include:
- Insufficient calories and protein — simply not eating enough food, or enough nutrient-dense food, is the most fundamental cause of stunting worldwide.
- Repeated infections — chronic and recurrent diarrhea and other infections divert energy to fighting illness and damage the gut's ability to absorb nutrients (so-called environmental enteric dysfunction). Infection and undernutrition reinforce each other.
- Other micronutrient shortfalls — especially zinc and iron, which independently affect growth. The large meta-analysis by Ramakrishnan and colleagues found that interventions giving multiple micronutrients improved child growth, whereas vitamin A given alone (or iron alone) generally did not — a crucial, sobering finding for anyone tempted to view vitamin A as a single fix.
- Poor maternal nutrition and low birth weight — growth deficits often begin before birth and in the first months of life.
- Lack of clean water and sanitation — the upstream cause of the repeated infections that stunt growth.
- Underlying disease — conditions that impair absorption (such as celiac disease, Crohn's disease, or cystic fibrosis) cause faltering growth regardless of how much food a child is offered.
The honest bottom line from the research is two-sided, and both halves are true. On growth, vitamin A supplementation has only a modest and inconsistent effect: a single randomized trial in Indonesian preschool children found vitamin A selectively improved linear growth (height) in those who were deficient, but pooled analyses across many studies do not show a reliable growth benefit from vitamin A alone. On survival, by contrast, the evidence is strong and consistent: in vitamin-A-deficient populations, supplementation clearly reduces child mortality. So the accurate message is not “vitamin A makes children grow,” but rather “in populations where deficiency is common, vitamin A keeps more children alive” — and growth, where it improves, does so mostly by reducing the infections that were holding a child back.
When Poor Growth Points Toward Vitamin A
Because faltering growth has many causes, a few features make vitamin A deficiency more likely to be part of the picture and worth checking:
- Eye signs are present — night blindness, dry eyes, or Bitot's spots are the most specific pointer to vitamin A deficiency. A child with both poor growth and any eye sign should be treated for vitamin A deficiency without delay (see Night Blindness and Eye Damage).
- The child lives where deficiency is common — in much of sub-Saharan Africa and South Asia, vitamin A deficiency is widespread among preschool children, so it should be high on the list. In high-income countries it is rare in healthy children and points instead toward an absorption problem.
- A diet very low in vitamin A — little or no liver, eggs, dairy, fortified foods, or deeply colored fruits and vegetables (the orange and dark-green ones rich in beta-carotene). See Vitamin A food sources.
- Recurrent infections out of proportion to peers — a child who catches everything, recovers slowly, and especially one who has had severe measles or persistent diarrhea.
- A known fat-malabsorption condition — vitamin A is fat-soluble, so any disease that impairs fat absorption (cystic fibrosis, celiac, Crohn's) can cause deficiency even on an adequate diet.
Conversely, a well-grown, well-fed child in a high-income setting with a varied diet is very unlikely to be vitamin-A-deficient, and chasing that diagnosis would distract from the real cause of any growth concern. The point of these clues is to aim attention where it belongs.
The Global Scale of the Problem
This is, above all, a global public-health story, and the numbers are worth stating plainly. Vitamin A deficiency is one of the most common nutritional deficiencies among children in low- and middle-income countries. A pooled analysis of population surveys by Stevens and colleagues estimated that in 2013 roughly 29% of children under five in low- and middle-income countries — on the order of 190 million children — were vitamin A deficient, and it attributed close to 100,000 child deaths that year to the deficiency, concentrated in sub-Saharan Africa and South Asia. Earlier work by West and colleagues had similarly mapped how widespread the deficiency was among preschool children and women of reproductive age.
The deficiency does not sit in isolation. The landmark Lancet series on maternal and child undernutrition (Black and colleagues, 2008 and 2013) placed vitamin A deficiency among the cluster of nutritional risks — together with stunting, wasting, and zinc and iron deficiency — that together account for a large share of deaths in children under five worldwide. Vitamin A deficiency is, in other words, both a cause of death in its own right and a marker that a child is caught in the broader trap of undernutrition.
The encouraging counterpart to these grim figures is how cheaply the survival benefit can be bought. High-dose vitamin A capsules cost only cents per dose, and twice-yearly distribution has been one of the most cost-effective child-survival interventions ever deployed. Wirth and colleagues have catalogued how widely such programs run and where deficiency persists despite them — a reminder that coverage is uneven and the job is unfinished, even as diets and fortification slowly improve in many countries.
What Causes Vitamin A Deficiency in Children
Vitamin A deficiency in a child usually comes from one or a combination of the following:
- A diet poor in vitamin A — the most common cause globally. Preformed vitamin A (retinol) comes from animal foods — liver, eggs, dairy, and fish-liver oils — while plant foods provide beta-carotene, which the body converts to vitamin A. Diets built almost entirely on starchy staples (rice, maize, cassava) with little animal food or colorful produce supply too little of either.
- Weaning and early childhood — breast milk is a good source of vitamin A, so the highest-risk window often opens after weaning, when a child shifts onto a poor family diet. A mother who is herself deficient produces breast milk lower in vitamin A, extending the risk back to infancy.
- Repeated infection — as described above, measles, diarrhea, and other infections deplete vitamin A and damage the gut, both reducing intake (through poor appetite) and increasing loss. Infection and deficiency drive each other.
- Fat malabsorption — vitamin A needs dietary fat and a healthy gut and pancreas to be absorbed. Conditions such as cystic fibrosis, celiac disease, and Crohn's disease impair that process and can cause deficiency even where diet and supply are adequate.
- Very-low-fat diets and protein deficiency — because vitamin A travels and is stored with fat and is carried in the blood on a protein (retinol-binding protein) that the malnourished body cannot make enough of, severe protein-energy malnutrition worsens functional vitamin A deficiency.
In wealthy countries, dietary vitamin A deficiency in otherwise healthy children is uncommon; when it occurs there it almost always reflects an underlying malabsorption disorder or a very restrictive diet, and that underlying cause is what needs finding and treating.
Diagnosis and Measurement
Diagnosing vitamin A deficiency combines what the clinician sees with what the lab measures, and each has limits worth understanding.
Clinical signs. The eye findings — night blindness, conjunctival dryness, Bitot's spots, and in advanced disease the corneal damage of keratomalacia — are specific enough that, in a deficient population, their presence is itself a diagnosis and a reason to treat at once. Faltering growth is tracked on standard growth charts; recurrent severe infection adds to the suspicion. None of these is unique to vitamin A, which is why they are interpreted together and against the child's setting.
Blood testing. The usual lab measure is serum (plasma) retinol. It has an important quirk: the body keeps blood retinol fairly steady by drawing on liver stores, so the blood level stays near-normal until those stores are quite depleted — it is an insensitive gauge of mild deficiency. Worse, retinol falls during infection and inflammation regardless of true vitamin A status, so a low value in a sick child can over-state deficiency. For this reason results are interpreted alongside markers of inflammation (such as CRP), and a routine comprehensive metabolic panel is often drawn at the same time to check overall nutrition, protein, and liver and kidney function. The authoritative Biomarkers of Nutrition for Development (BOND) review by Tanumihardjo and colleagues lays out the strengths and weaknesses of each test — from serum retinol to more sophisticated measures of liver stores — and is the reference clinicians use to choose and interpret them.
The practical reality. In the low-resource settings where vitamin A deficiency is most common and most dangerous, individual blood testing is often impractical. Public-health programs therefore identify deficiency at the population level — through surveys of eye signs and retinol in samples of children — and respond by supplementing all young children in affected areas rather than testing each one. For an individual child, the combination of an at-risk setting, a poor diet, eye signs, or recurrent severe infection is frequently enough to justify treatment without waiting for a number.
Correcting and Preventing It
The response to vitamin A deficiency works on three levels — treating the deficient child, preventing deficiency across a population, and fixing the diet for the long term — and the doses differ sharply between them.
Treatment of an affected child (high dose, medically supervised). A child with clinical deficiency — eye signs — or one who has measles or severe malnutrition in an at-risk area is given high-dose vitamin A under a standard WHO schedule (an age-based dose, typically repeated the next day and again after a couple of weeks for xerophthalmia). These are large therapeutic doses delivered by health workers, not something to improvise at home, and they can rapidly reverse night blindness and reduce the risk of death and complications.
Prevention across a population (the public-health workhorse). The strategy that has saved the most lives is periodic high-dose supplementation — usually two capsules a year — for all children aged six months to five years in regions where deficiency is common. The Cochrane systematic review by Imdad and colleagues, pooling many large trials, found this reduces all-cause mortality in this age group by roughly a fifth, alongside fewer deaths from diarrhea and fewer cases of measles and night blindness. The earlier meta-analysis by Fawzi and colleagues reached the same headline conclusion. This is the evidence behind the global twice-yearly capsule campaigns. (It is also why the benefit is concentrated where deficiency exists: in well-nourished populations, supplementing children who already have enough vitamin A does not show the same survival benefit.)
Food and long-term fix. The durable solution is a diet that supplies enough vitamin A — the goal of the food-sources approach:
- Preformed vitamin A (retinol) from animal foods — cod liver (and cod-liver oil), beef liver, eggs, and dairy. Liver is the single richest source.
- Beta-carotene from deeply colored produce — sweet potatoes, carrots, pumpkin, mango, and dark leafy greens such as spinach. The body converts beta-carotene to vitamin A as needed (the difference between the two is explained on Beta-Carotene vs. Preformed Vitamin A). Because beta-carotene is fat-soluble, serving these foods with a little fat improves absorption.
- Food fortification and biofortification — adding vitamin A to staples (sugar, oil, flour) and breeding vitamin-A-rich crops (such as orange-fleshed sweet potato and biofortified maize) are increasingly the backbone of long-term prevention.
- Protecting the mother and breastfeeding — a well-nourished mother and breastfeeding give an infant a strong vitamin A start.
One safety caveat. Vitamin A is fat-soluble and stored in the liver, so it can be toxic in excess — this matters most for the high therapeutic doses, which is exactly why they are given on a defined schedule by health workers rather than freely. Food sources and beta-carotene, by contrast, are very safe (the body limits how much beta-carotene it converts). Vitamin A is also a special concern in pregnancy, where excess preformed vitamin A can harm the developing baby; the general limits and the harms of too much are covered on the Vitamin A Toxicity hub.
Red Flags / When to Seek Care
For vitamin A deficiency in a child, certain signs mean seek medical care promptly — and some mean treat as an emergency:
- Any eye sign — night blindness (a child who can't see or navigate at dusk), dry or dull-looking eyes, or foamy white patches on the white of the eye. Eye pain, sensitivity to light, clouding of the cornea, or a sudden change in vision is an emergency — corneal damage from vitamin A deficiency can destroy sight within days and needs immediate treatment to save the eye.
- Measles in a young child — in areas where deficiency occurs, a child with measles should receive vitamin A; seek care, because measles can deteriorate quickly and vitamin A reduces its complications and deaths.
- Severe or persistent diarrhea, or repeated chest infections — especially with poor feeding or signs of dehydration. Recurrent severe infection in an undernourished child is the dangerous pattern this whole page is about.
- Faltering growth — a child crossing downward through the growth-chart lines, losing weight, or persistently short for their age deserves evaluation for its underlying cause (which may or may not include vitamin A).
- Signs of serious illness in any young child — lethargy or unusual drowsiness, refusing to feed or drink, fast or labored breathing, a high fever that won't settle, or a child who simply “isn't right” — warrant urgent assessment regardless of nutritional status.
The unifying theme is that the danger of vitamin A deficiency is mostly the danger of the infection it fails to defend against. A deficient child can look only mildly unwell right up until a common illness turns serious, so when a young child in an at-risk setting falls ill, it is safest to seek care early rather than wait.
Key Research Papers
- Imdad A, Mayo-Wilson E, Herzer K, et al. (2017). Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database of Systematic Reviews;2017(11):CD008524. — DOI: 10.1002/14651858.CD008524.pub3
- Fawzi WW, Chalmers TC, Herrera MG, Mosteller F (1993). Vitamin A Supplementation and Child Mortality: A Meta-analysis. JAMA;269(7):898-903. — DOI: 10.1001/jama.1993.03500070078033
- Stevens GA, Bennett JE, Hennocq Q, et al. (2015). Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: a pooled analysis of population-based surveys. The Lancet Global Health;3(9):e528-e536. — DOI: 10.1016/S2214-109X(15)00039-X
- West KP Jr (2002). Extent of Vitamin A Deficiency among Preschool Children and Women of Reproductive Age. The Journal of Nutrition;132(9):2857S-2866S. — DOI: 10.1093/jn/132.9.2857S
- Hadi H, Stoltzfus RJ, Dibley MJ, et al. (2000). Vitamin A supplementation selectively improves the linear growth of Indonesian preschool children: results from a randomized controlled trial. The American Journal of Clinical Nutrition;71(2):507-513. — DOI: 10.1093/ajcn/71.2.507
- Ramakrishnan U, Aburto N, McCabe G, Martorell R (2004). Multimicronutrient Interventions but Not Vitamin A or Iron Interventions Alone Improve Child Growth: Results of 3 Meta-Analyses. The Journal of Nutrition;134(10):2592-2602. — DOI: 10.1093/jn/134.10.2592
- Black RE, Allen LH, Bhutta ZA, et al. (2008). Maternal and child undernutrition: global and regional exposures and health consequences. The Lancet;371(9608):243-260. — DOI: 10.1016/S0140-6736(07)61690-0
- Black RE, Victora CG, Walker SP, et al. (2013). Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet;382(9890):427-451. — DOI: 10.1016/S0140-6736(13)60937-X
- Stephensen CB (2001). Vitamin A, Infection, and Immune Function. Annual Review of Nutrition;21:167-192. — DOI: 10.1146/annurev.nutr.21.1.167
- Tanumihardjo SA, Russell RM, Stephensen CB, et al. (2016). Biomarkers of Nutrition for Development (BOND)—Vitamin A Review. The Journal of Nutrition;146(9):1816S-1848S. — DOI: 10.3945/jn.115.229708
- Wirth JP, Petry N, Tanumihardjo SA, et al. (2017). Vitamin A Supplementation Programs and Country-Level Evidence of Vitamin A Deficiency. Nutrients;9(3):190. — DOI: 10.3390/nu9030190
PubMed Topic Searches
- PubMed — Vitamin A supplementation and child mortality
- PubMed — Vitamin A deficiency, child growth, and stunting
- PubMed — Vitamin A, measles, and child mortality
- PubMed — Vitamin A deficiency prevalence in low-income countries
- PubMed — Vitamin A, infection, and epithelial immunity
Connections
- Vitamin A Deficiency Hub
- Night Blindness and Eye Damage
- Weakened Immunity and Infections
- Skin Problems and Hyperkeratosis
- Vitamin A Toxicity
- Vitamin A Overview
- Vitamin A and Immune Function
- Beta-Carotene vs. Preformed Vitamin A
- Vitamin A Food Sources
- Zinc
- Measles
- Celiac Disease
- Crohn's Disease
- Cystic Fibrosis
- Comprehensive Metabolic Panel
- Cod Liver
- Beef Liver
- Sweet Potatoes
- Spinach
- Eggs