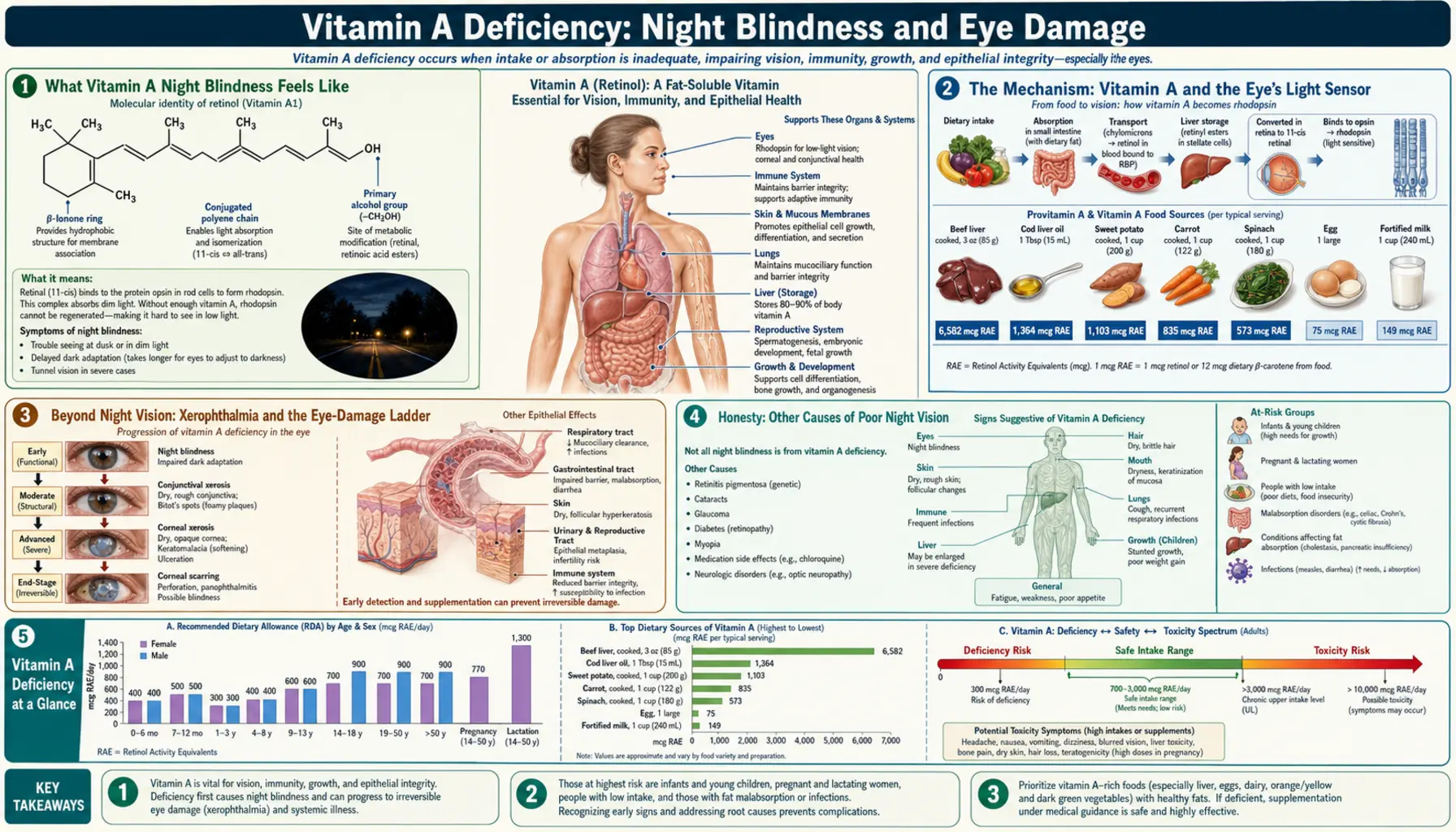
Vitamin A Deficiency: Night Blindness and Eye Damage
The very first sign of vitamin A running low is usually something quiet and easy to dismiss: the world stops coming back when the lights go down. You step from a bright kitchen into a dark hallway and stand frozen for far longer than you used to. Driving at night, the glare of oncoming headlights leaves you blind for seconds afterward. This is night blindness — the earliest, most reversible warning of vitamin A deficiency — and it is the first rung on a ladder that, left to climb, leads to a drying, scarring eye disease called xerophthalmia and can end in irreversible blindness. The same vitamin needed to make the light-sensing pigment in your eye is also needed to keep the surface of the eye moist and clear, which is why a single nutrient shortfall can both dim your night vision and damage the eye itself. This page explains how that happens, why night blindness is genuinely reversible if caught early, what the more advanced eye changes look like, and how the deficiency is confirmed and corrected.
Table of Contents
- What Vitamin A Night Blindness Feels Like
- The Mechanism: Vitamin A and the Eye's Light Sensor
- Beyond Night Vision: Xerophthalmia and the Eye-Damage Ladder
- Honesty: Other Causes of Poor Night Vision
- When Night Blindness Points to Vitamin A
- What Causes Vitamin A to Run Low
- Getting Tested
- Correcting Vitamin A Deficiency Safely
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Vitamin A Night Blindness Feels Like
Doctors call it nyctalopia; almost everyone who has it calls it “not being able to see in the dark.” The technical meaning is specific and worth understanding: it is not blindness in the dark in the literal sense, but a failure of the eye to adapt to dim light. A healthy eye, moving from bright to dark, keeps getting more sensitive for up to half an hour as it tunes itself for the gloom (this is “dark adaptation”). In vitamin A deficiency that tuning is slow, incomplete, or both, so the dimly lit world that others can navigate stays stubbornly black to you.
The everyday experiences are remarkably consistent from person to person:
- Slow recovery walking into a dark room. Stepping from a lit room into a dark bedroom or a dim cinema, you stall in the doorway, unable to make out furniture that you know is there, for far longer than the people around you.
- Trouble driving at night. This is one of the most common complaints. The road feels darker than it should, and the glare of oncoming headlights produces a blinding flash followed by a long blind spell before your eyes recover.
- Bumping into things at dusk. In traditional descriptions from communities where the deficiency is common, children stop being able to find their way around the home as the sun goes down — so reliably that some cultures have their own folk name for it, sometimes translated as “evening blindness” or “chicken eyes” (because chickens, lacking rod-rich vision, are helpless after dark).
- Daytime vision feels normal. This is the tell-tale asymmetry: in bright light, central vision and visual acuity can be entirely normal, so the person may pass a standard eye-chart test and be reassured, while the problem is purely one of low light.
The crucial, hopeful fact about this stage is that it is fully reversible. Night blindness from vitamin A deficiency is a functional problem — the machinery of the eye is intact but starved of a raw material — and replacing vitamin A typically restores night vision within days. That is precisely why it matters so much: it is both the earliest warning and the last easy off-ramp before the deficiency starts to cause structural, scarring damage to the eye.
The Mechanism: Vitamin A and the Eye's Light Sensor
To understand why a vitamin shortage dims night vision specifically, you have to look at the back of the eye, at the retina, where two kinds of light-detecting cells live. The cones handle color and fine detail and work in bright light. The rods are the dim-light specialists — they are exquisitely sensitive, can respond to a handful of photons, and are the cells you rely on at night. And the rods are exactly the cells that fail first when vitamin A runs low.
Here is why. Each rod is packed with a light-sensitive pigment called rhodopsin (“visual purple”). Rhodopsin is built from two parts clipped together: a protein called opsin, and a small molecule called 11-cis-retinal — and that small molecule is made directly from vitamin A (retinol). When a photon of light strikes rhodopsin, it does something elegantly simple: it bends the retinal from its cis (kinked) shape into the straight trans shape. That tiny change of shape is the spark — it triggers a cascade that fires the rod and tells the brain “light.” The Nobel-winning work of George Wald established this as the chemical heart of vision.
But each capture of light uses up a molecule of rhodopsin: the bent (all-trans) retinal falls off the opsin, and the pigment goes “blank” until it can be rebuilt. Rebuilding it means taking that spent retinal, bending it back into the cis shape, and re-attaching it to opsin — a recycling loop biochemists call the visual cycle (or retinoid cycle), carried out between the rods and the supporting layer behind them. The whole loop runs on a steady supply of vitamin A. When that supply is short, the eye cannot regenerate rhodopsin fast enough; the rods are left with too little working pigment, and their ability to respond in dim light collapses. Hence night blindness.
An analogy. Picture each rod as a camera that has to chemically “develop” a fresh frame of film for every shot, and vitamin A as the developing chemical. In bright daylight there is so much light that even a half-stocked camera grabs an image. But at night, when there is barely any light to work with, you need every rod fully loaded with fresh pigment to catch the few photons available. Let the developing chemical run low and the daytime photos still come out fine — while the night shots come back black. The eye is not broken; it has simply run out of the one ingredient it needs to reload its dim-light sensors. Top the vitamin back up and, because the rods themselves are undamaged, the pictures return.
Beyond Night Vision: Xerophthalmia and the Eye-Damage Ladder
Vitamin A does a second job in the eye that has nothing to do with detecting light, and it is this second job whose failure turns a reversible nuisance into a blinding disease. Beyond feeding the visual cycle, vitamin A is essential for maintaining healthy epithelium — the surface lining tissues — including the moist, transparent surfaces of the eye: the conjunctiva (the membrane over the white of the eye) and the cornea (the clear front window). Without enough vitamin A, these surfaces stop producing normal mucus and tears, dry out, thicken, and lose their clarity. The umbrella term for the whole spectrum of vitamin-A eye disease is xerophthalmia, literally “dry eye,” and the World Health Organization grades it as a recognizable ladder of worsening stages:
- Night blindness (XN) — the functional, fully reversible first stage described above; no visible damage to the eye yet.
- Conjunctival xerosis (X1A) — the white of the eye loses its normal glossy wetness and looks dry, dull, and roughened, because the conjunctiva is no longer producing normal mucus.
- Bitot's spots (X1B) — foamy, silvery-white, slightly raised patches on the white of the eye, usually to the side of the iris. They are made of built-up keratin and debris on the dried-out conjunctiva and are a classic, almost diagnostic sign of vitamin A deficiency in children. At this stage the changes are still largely reversible with treatment.
- Corneal xerosis (X2) — the drying now reaches the clear cornea itself, which becomes hazy and rough. This is a warning that the eye is approaching the point of no return.
- Corneal ulceration / keratomalacia (X3A, X3B) — the most feared stage. The cornea can ulcerate and, in keratomalacia, literally soften and melt away, sometimes over a matter of days, especially in a malnourished young child with an added infection such as measles. This destroys the cornea and causes permanent, irreversible blindness.
- Corneal scars (XS) and xerophthalmic fundus (XF) — the healed aftermath: a scarred, opaque cornea (a blinding white scar) is the lasting legacy of advanced disease.
The reason this ladder matters so much is the contrast between its top and bottom rungs. The first rung — night blindness — costs nothing but a little vitamin A to undo. The bottom rungs cause some of the most preventable blindness in the world: vitamin A deficiency remains a leading cause of childhood blindness globally, and the children who reach keratomalacia are at very high risk of dying as well, because the same deficiency that melted the cornea has also crippled their defenses against infection. The cruelty of xerophthalmia is that it climbs from utterly fixable to utterly irreversible, and it can do so quickly. (For the broader role of vitamin A in protecting against infection, see the sibling page on Weakened Immunity & Infections.)
Honesty: Other Causes of Poor Night Vision
It would be misleading to suggest that trouble seeing in the dark always means vitamin A deficiency. It usually does not — especially in well-fed populations where dietary vitamin A deficiency is uncommon. Poor night vision is a symptom with several causes, and being honest about them is part of getting the right diagnosis. Common alternative explanations include:
- Cataracts. A clouding of the eye's lens scatters light and is one of the most common reasons older adults struggle with night driving and glare from headlights. This is mechanical, not nutritional. See Cataracts.
- Retinitis pigmentosa and other inherited retinal diseases. A group of genetic conditions in which the rod cells themselves progressively degenerate. Night blindness is often the first symptom, but here it is caused by the rods dying, not by a missing nutrient, and it is not reversible with vitamin A.
- Refractive error, especially uncorrected myopia. Near-sightedness gets functionally worse in the dark, because the pupil widens and the eye's focusing errors become more pronounced — so some “night blindness” is simply a glasses prescription that needs updating.
- Glaucoma and diabetic retinopathy. Conditions that damage the retina or optic nerve can impair dim-light and peripheral vision. See Diabetic Retinopathy.
- Normal aging and certain medications. Dark adaptation slows somewhat with age, and a few drugs can affect it as well.
The practical upshot is that new or worsening night blindness deserves an eye examination, not a self-diagnosis. Vitamin A deficiency is one cause among several, and the others — particularly cataracts and retinitis pigmentosa — need entirely different management. What makes the vitamin A cause distinctive is its company: the clues below.
When Night Blindness Points to Vitamin A
Night blindness is far more likely to be vitamin A deficiency when it occurs alongside the right context and the right companions. The features that should raise suspicion are:
- A reason to be deficient. Vitamin A night blindness rarely appears out of nowhere in a well-nourished adult. It is strongly associated with the risk situations in the next section — fat malabsorption, liver disease, bariatric surgery, very restricted diets, alcohol overuse, and (globally) childhood undernutrition and pregnancy in low-resource settings.
- Other signs of dryness. Because vitamin A maintains all surface tissues, deficiency often brings a constellation: dry, rough skin with hard little bumps (follicular hyperkeratosis), and a notably dry eye surface (dry eye disease). Night blindness plus a sandpapery dry eye and dry, bumpy skin is a far more telling pattern than night blindness alone.
- Visible eye changes. The appearance of Bitot's spots — those foamy white patches on the white of the eye — alongside poor night vision is close to diagnostic of vitamin A deficiency, particularly in a child.
- Frequent or severe infections. Because the same deficiency weakens immune defenses, recurrent or unusually severe infections occurring together with night blindness fit the vitamin A picture — see Weakened Immunity & Infections.
- A rapid response to vitamin A. Night blindness that resolves within a few days of vitamin A treatment is itself strong confirmation that vitamin A was the cause — a kind of diagnosis by response.
By contrast, night blindness with a completely normal, moist eye surface, normal skin, no malabsorption or dietary risk, and a family history of failing vision points away from vitamin A and toward an inherited retinal disease or a lens problem — which is exactly why an eye examination, not a supplement bottle, is the right first move when the cause is unclear.
What Causes Vitamin A to Run Low
Vitamin A is a fat-soluble vitamin, and the body keeps large stores of it in the liver — often enough for many months. That reserve is why deficiency develops slowly and why it tends to appear only when intake is poor and stores have been drained, or when the body cannot absorb or store the vitamin properly. The main routes to a true shortfall are:
- Inadequate diet, on a global scale. This is the dominant cause worldwide. In regions where preformed vitamin A (from animal foods such as liver, eggs, and dairy) is scarce and diets rely on staples low in the carotenoids the body converts to vitamin A, deficiency is common — especially in young children and pregnant women. It remains a major public-health problem across parts of Africa and South Asia.
- Fat malabsorption. Because vitamin A needs dietary fat and bile to be absorbed, any condition that impairs fat absorption can starve the body of it even when the diet contains plenty. Key examples are cystic fibrosis, celiac disease, Crohn's disease, chronic pancreatitis, and cholestatic liver disease. Vitamin-A night blindness in a well-fed Western adult is, classically, a clue to one of these.
- Liver disease. The liver both stores vitamin A and makes the transport protein (retinol-binding protein) that carries it in the blood. Significant liver disease can therefore lower circulating vitamin A and cause functional deficiency.
- Bariatric (weight-loss) surgery. Procedures that bypass part of the small intestine reduce fat absorption and are an increasingly recognized cause of fat-soluble vitamin deficiencies, including vitamin A, sometimes years after surgery.
- Very restricted or fat-free diets, and heavy alcohol use. Extremely limited diets can fall short of vitamin A and of the fat needed to absorb it, and chronic alcohol use both displaces good nutrition and interferes with vitamin A storage and metabolism in the liver.
- Increased need: infancy, pregnancy, and infection. Rapid growth and pregnancy raise requirements, and infections — measles in particular — sharply deplete vitamin A, which is exactly why measles can tip a marginally nourished child into blinding xerophthalmia and why the World Health Organization recommends vitamin A for children with measles in at-risk settings.
Identifying which of these is at work matters, because the fix differs: a dietary shortfall is corrected with food and supplements, whereas malabsorption from cystic fibrosis or after bariatric surgery requires ongoing, monitored, often higher-dose replacement and treatment of the underlying problem.
Getting Tested
When vitamin A deficiency is suspected, the picture is usually built from the history, the eye examination, and a blood test — no single test stands alone.
The standard blood test is serum retinol, which measures the amount of vitamin A circulating in the blood. It has an important limitation patients should understand: because the liver buffers blood levels using its stores, serum retinol can stay near-normal until those stores are substantially depleted, and it also falls temporarily during infection and inflammation regardless of true vitamin A status. So a “normal” result does not completely exclude early deficiency, and a low result during an acute illness should be interpreted with care. Even so, a clearly low serum retinol in the right clinical setting is strong supporting evidence.
Other useful pieces of the workup include:
- The eye examination itself. An eye-care professional can detect conjunctival and corneal dryness, identify Bitot's spots, and grade xerophthalmia — findings that, combined with the history, are often more informative than the blood number.
- Dark adaptometry. A test that formally measures how the eye's sensitivity recovers in the dark; impaired dark adaptation that improves after vitamin A supports the diagnosis.
- Tests for the underlying cause. Because malabsorption and liver disease are common culprits, evaluation frequently includes liver function tests and other markers of fat absorption and nutrition (a broader metabolic panel helps characterize liver and kidney function). Where one fat-soluble vitamin is low, others — vitamin D and vitamin E — are often checked too, since they share the same absorption pathway.
In short, the diagnosis is clinical and contextual: a story that fits, an eye that shows it, and a blood level that supports it, all pointing the same way.
Correcting Vitamin A Deficiency Safely
The good news is that vitamin A deficiency responds well and quickly to treatment, and night blindness in particular often reverses within days. The principle is to replace the vitamin promptly — urgently if the eye is already affected — while fixing whatever caused the deficiency and respecting that vitamin A, unlike water-soluble vitamins, can build up to toxic levels if overdone.
- Food first, for prevention and mild cases. The richest sources of ready-made vitamin A are animal foods: beef liver and cod liver oil are extraordinarily concentrated, with eggs and dairy adding more. The body also makes vitamin A from provitamin A carotenoids (chiefly beta-carotene) in deeply colored plants — sweet potatoes, kale, spinach, and orange vegetables — though conversion is less efficient and is improved by eating them with a little fat. A noteworthy safety point: you essentially cannot reach vitamin A toxicity from plant carotenoids, because the body throttles its conversion.
- Medical, high-dose vitamin A for established deficiency or xerophthalmia. When the eye is affected, this is a medical emergency treated with a specific, weight- and age-based schedule of high-dose vitamin A (the World Health Organization protocol gives large oral doses on day 1, day 2, and roughly two weeks later). This is given under medical supervision — it is not self-treatment — and in a young child with corneal involvement it can be sight-saving and life-saving.
- Treat the underlying cause. In malabsorption (cystic fibrosis, celiac disease, post-bariatric surgery, cholestatic liver disease), replacement must be ongoing and monitored, often with water-miscible vitamin A preparations and periodic blood checks, because the leak that caused the deficiency does not close on its own.
- Respect the ceiling — especially in pregnancy. Because vitamin A is fat-soluble and stored, chronic high-dose supplementation can cause toxicity (see the companion Vitamin A Toxicity hub). Crucially, high-dose preformed vitamin A is harmful to a developing baby and can cause birth defects, so the large therapeutic doses used for deficiency are not given to pregnant women in the same way; vitamin A in pregnancy is managed carefully and specifically. This is the one area where “more is better” is dangerously wrong.
For most people the message is reassuring: catch it at the night-blindness stage, restore vitamin A through diet or appropriately dosed supplements, address the cause, and vision returns. The danger lies only in leaving it untreated until the cornea is damaged, or in swinging too far the other way with reckless high-dose self-supplementation.
When to Seek Care / Red Flags
Most night blindness is evaluated calmly with an eye examination and, where appropriate, a blood test. But certain features mean seek eye care promptly — and in the case of a child with advancing eye changes, urgently, because the window between reversible and permanent damage can be short:
- Any visible drying, dullness, or foamy white (Bitot's) spots on the white of the eye — signs the deficiency has moved past the reversible night-blindness stage onto the eye-damage ladder.
- A hazy, cloudy, or rough-looking cornea (the clear front of the eye), eye pain, or rapidly worsening vision — these suggest corneal involvement and require emergency eye care; keratomalacia can destroy a cornea within days.
- Night blindness in a young child, or in any child who is malnourished or recovering from measles — children deteriorate fastest and have the most to lose.
- Night blindness together with a known malabsorption condition (cystic fibrosis, celiac or Crohn's disease, prior bariatric surgery, or liver disease) — a signal that fat-soluble vitamins are not being absorbed and need formal assessment.
- New or steadily worsening night vision at any age — even when vitamin A is not the cause, this warrants an eye examination to check for cataracts, retinal disease, or glaucoma.
The single most important idea to carry away is the time-sensitivity: night blindness and Bitot's spots are reversible, but a damaged cornea is not. When eye changes are visible, especially in a child, treat it as the emergency it is rather than waiting to see whether it improves.
Key Research Papers
- Sommer A (2008). Vitamin A Deficiency and Clinical Disease: An Historical Overview. The Journal of Nutrition;138(10):1835-1839. — DOI: 10.1093/jn/138.10.1835
- Sommer A (1997). Vitamin A deficiency, child health, and survival. Nutrition;13(5):484-485. — DOI: 10.1016/s0899-9007(97)00013-0
- Stevens GA, Bennett JE, Hennocq Q, et al. (2015). Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991 and 2013. The Lancet Global Health;3(9):e528-e536. — DOI: 10.1016/s2214-109x(15)00039-x
- West KP Jr (2002). Extent of Vitamin A Deficiency among Preschool Children and Women of Reproductive Age. The Journal of Nutrition;132(9):2857S-2866S. — DOI: 10.1093/jn/132.9.2857s
- Wald G (1968). Molecular Basis of Visual Excitation. Science;162(3850):230-239. — DOI: 10.1126/science.162.3850.230
- Kiser PD, Golczak M, Palczewski K (2014). Chemistry of the Retinoid (Visual) Cycle. Chemical Reviews;114(1):194-232. — DOI: 10.1021/cr400107q
- Saari JC (2012). Vitamin A Metabolism in Rod and Cone Visual Cycles. Annual Review of Nutrition;32:125-145. — DOI: 10.1146/annurev-nutr-071811-150748
- Mayo-Wilson E, Imdad A, Herzer K, Yakoob MY, Bhutta ZA (2011). Vitamin A supplements for preventing mortality, illness, and blindness in children aged under 5: systematic review and meta-analysis. BMJ;343:d5094. — DOI: 10.1136/bmj.d5094
- Imdad A, Mayo-Wilson E, Herzer K, Bhutta ZA (2017). Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database of Systematic Reviews;(3):CD008524. — DOI: 10.1002/14651858.cd008524.pub3
- Hussey GD, Klein M (1990). A Randomized, Controlled Trial of Vitamin A in Children with Severe Measles. New England Journal of Medicine;323(3):160-164. — DOI: 10.1056/nejm199007193230304
PubMed Topic Searches
- PubMed — Vitamin A deficiency and night blindness
- PubMed — Xerophthalmia and the WHO classification
- PubMed — Bitot's spots and conjunctival xerosis
- PubMed — Keratomalacia and corneal damage
- PubMed — Rhodopsin, retinal, and the visual cycle
Connections
- Vitamin A Deficiency Hub
- Weakened Immunity & Infections
- Skin Problems (Hyperkeratosis)
- Poor Growth & Child Mortality
- Vitamin A Overview
- Vitamin A Toxicity
- Vitamin A and Vision
- Dry Eye Disease
- Cataracts
- Diabetic Retinopathy
- Measles
- Cystic Fibrosis
- Liver Function Tests
- Vitamin D3
- Vitamin E
- Beef Liver
- Cod Liver Oil
- Sweet Potatoes