Mouth Taping: The Popular Sleep Practice — Evidence, Safety, and Who Should Avoid It
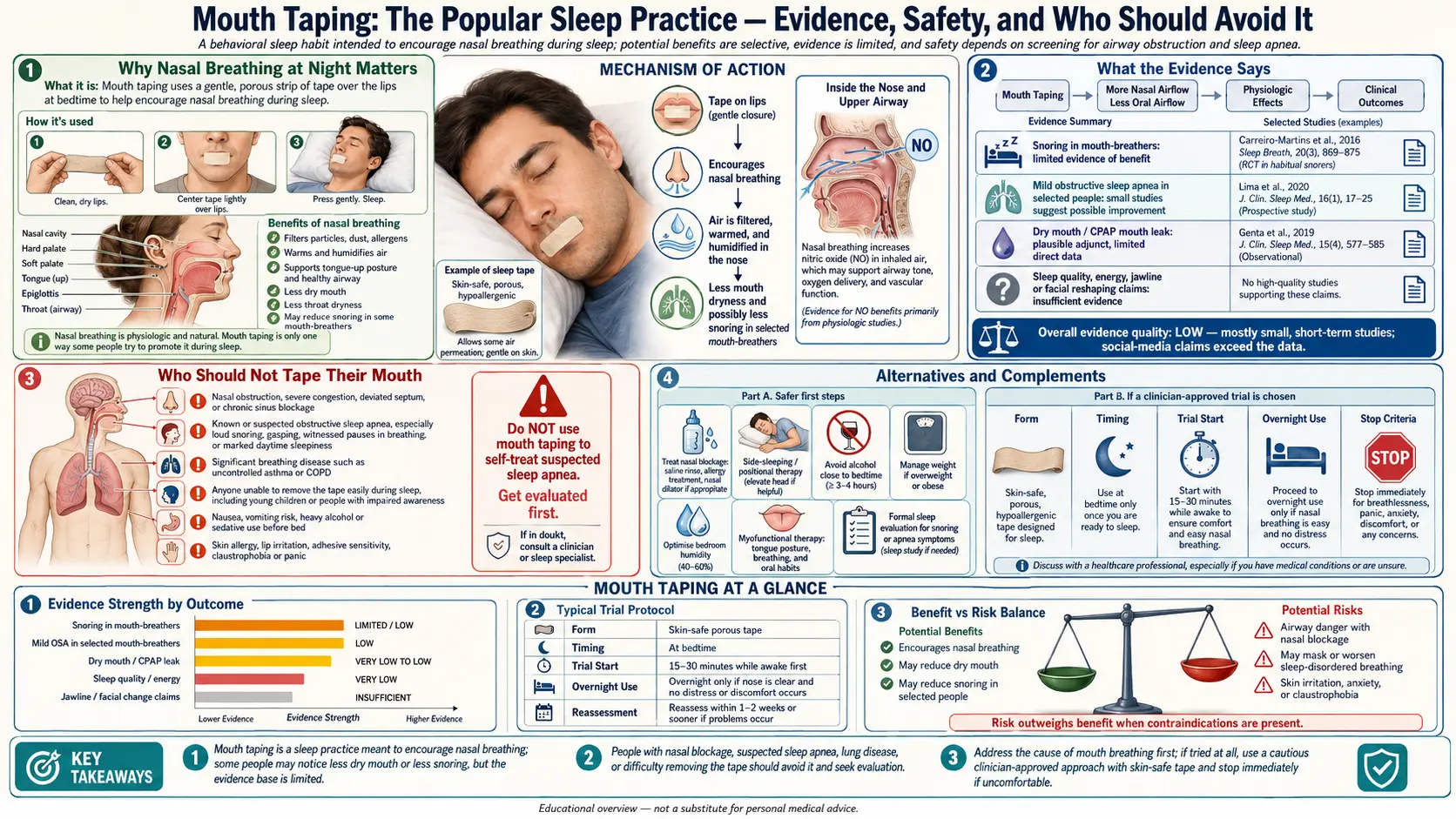



Mouth taping — placing a small strip of hypoallergenic tape across the lips at bedtime to encourage nasal breathing during sleep — has exploded from obscurity into mainstream sleep culture, driven largely by journalist James Nestor’s 2020 book Breath and subsequent coverage by sleep specialists, dentists, and myofunctional therapists. The practice is genuinely simple, typically cheap, and for the right person produces measurable improvements in sleep quality, snoring, dry mouth, and daytime energy. For the wrong person — particularly anyone with untreated obstructive sleep apnea — it may carry meaningful risks.
This article lays out what mouth taping actually does, the evidence so far, who stands to benefit, who should not try it without medical evaluation, and how to do it safely.
Interactive Visualization Sleep Apnea — collapse the airway, then splint it open with CPAP Watch the throat close as sleep deepens, the chest heave against a shut airway and oxygen slide into the 80s — then switch on CPAP and see the whole night go quiet. Launch →Table of Contents
- Why Nasal Breathing at Night Matters
- Reported Benefits
- What the Evidence Says
- Who Is a Good Candidate
- Who Should Not Tape Their Mouth
- How to Do It Safely
- Alternatives and Complements
- Connections
- Featured Videos
Why Nasal Breathing at Night Matters
The nose is not a passive air inlet. Nasal breathing produces nitric oxide in the paranasal sinuses, filters particulates on nasal hair and mucus, humidifies and warms incoming air, slows breathing rate, and increases diaphragmatic engagement. Sleeping with a wide open mouth reverses nearly all of these effects, contributes to dehydration of oral tissues, raises the risk of snoring and pharyngeal collapse, and in children disrupts orofacial development.
Reported Benefits
Anecdotal and preliminary-trial benefits include:
- Reduced snoring in mild cases, because mouth breathing is a prerequisite for most snoring.
- Less dry mouth and morning sore throat.
- Fewer nighttime awakenings.
- Lower rate of dental caries and gum inflammation tied to mouth-breathing-induced xerostomia.
- Improved subjective sleep quality on wearable metrics in self-selected users.
- Reduction in morning bad breath (halitosis from anaerobic oral overgrowth in dry mouth).
What the Evidence Says
Clinical research on mouth taping is still young. A 2015 Taiwanese trial in patients with mild obstructive sleep apnea reported reductions in apnea-hypopnea index with porous oral patches in a subset of patients. A 2022 study in snorers without clinically significant OSA showed reduced snoring frequency. On the other hand, a 2024 review in JAMA Otolaryngology cautioned that the evidence base remains small and that mouth taping can be dangerous in patients with undiagnosed sleep apnea — in whom forced nasal breathing during an obstructive event could delay arousal. The practice is best viewed as an adjunct to, not a replacement for, proper diagnostic workup of snoring or fatigue.
Who Is a Good Candidate
- Habitual mouth-breather at night without evidence of sleep apnea.
- Mild snorer with partner complaints.
- Person who wakes with dry mouth or sore throat.
- Adults who already tolerate nasal breathing during the day.
- Patients with sleep apnea who are successfully treated with CPAP — some find taping complements CPAP delivery.
Who Should Not Tape Their Mouth
- Undiagnosed or untreated obstructive sleep apnea. Always complete a sleep study first if snoring is loud, witnessed apneas exist, or daytime sleepiness is significant.
- Significant nasal obstruction — deviated septum, severe polyps, chronic rhinitis. Fix the airway first.
- Children under medical evaluation. Pediatric nasal-breathing concerns require an ENT or sleep-medicine workup.
- Acute upper-respiratory illness with a blocked nose.
- Recent alcohol or sedative use that could blunt arousal.
- GERD severe enough to wake with reflux.
- Nausea-prone conditions or pregnancy in the third trimester.
How to Do It Safely
- Use a small, hypoallergenic, single-purpose tape (3M Micropore, specialized mouth-tape products) — not duct-tape or kinesiology tape.
- Place the tape vertically across the center of the lips, leaving corners free. Many users find a small X or a smaller horizontal strip sufficient. The goal is a gentle reminder, not an airtight seal.
- Test nasal patency first — sit upright and breathe comfortably through the nose for 60 seconds before taping. If that fails, clear the nose with saline irrigation before applying.
- Start with naps or the first hour of sleep, not the entire night, to assess tolerance.
- Never tape a child or impaired adult.
- Stop immediately if you develop morning headaches, racing heart, vivid dreams suggestive of oxygen desaturation, or any signal that breathing has worsened.
Alternatives and Complements
- Myofunctional therapy — tongue posture and facial-muscle training — is a more physiologically grounded fix for chronic mouth-breathing.
- Side sleeping reduces both snoring and the tendency for gravitational jaw drop.
- Nasal dilators (external strips or internal cones) improve airflow without restricting the mouth.
- CPAP therapy remains the standard for moderate-to-severe obstructive sleep apnea.
- Addressing allergies, reflux, and obesity — the upstream contributors.
Research Papers
Selected PubMed topic searches relevant to nasal breathing, mouth breathing, sleep-disordered breathing, and the physiological rationale for mouth taping.
- PubMed: Mouth breathing and sleep apnea
- PubMed: Nasal breathing and nitric oxide
- PubMed: Mouth taping and sleep quality
- PubMed: Oral breathing and dental malocclusion
- PubMed: Chronic mouth breathing in children
- PubMed: Nasal obstruction and snoring
- PubMed: CPAP and oronasal leak
- PubMed: Buteyko breathing and asthma
- PubMed: Nasal cycle and autonomic nervous system
- PubMed: Mouth breathing, xerostomia, and caries
- PubMed: Nasal breathing and exercise performance
- PubMed: OSA and positional/airway therapy
Connections
- Sleep Apnea: Why Breathing Stops at Night — interactive animation
- Obstructive Sleep Apnea
- Breathwork
- Sleep Hygiene
- Oral Microbiome
- Insomnia
- Sinusitis
- GERD
- Reflux
- Asthma
- Allergies
- Natural Anxiety Relief
- Stress Management