Cautions and Adaptation
Mouth taping is a low-risk intervention for the right patient and a potentially dangerous one for the wrong patient. There are absolute contraindications that should never be overridden, relative contraindications that warrant evaluation first, and a graduated adaptation protocol that minimizes the failure rate even in good candidates. This deep dive enumerates the hard rules, walks through tape selection and skin care, explains the daytime-first adaptation sequence, and describes the signals that should trigger discontinuation. The practice is conservative when done correctly and reckless when done without screening.
Table of Contents
- Absolute Contraindications — Do Not Tape
- Relative Contraindications — Evaluate First
- Confirming Nasal Patency Before Taping
- Tape Selection: What to Use and What to Avoid
- Application Techniques (Strip, Cross, Lip-Center)
- The Graduated Adaptation Protocol
- Skin Reactions and Lip Care
- When to Discontinue
- Special Populations (Children, Pregnancy, Elderly)
- Key Research Papers
- Connections
- Featured Videos
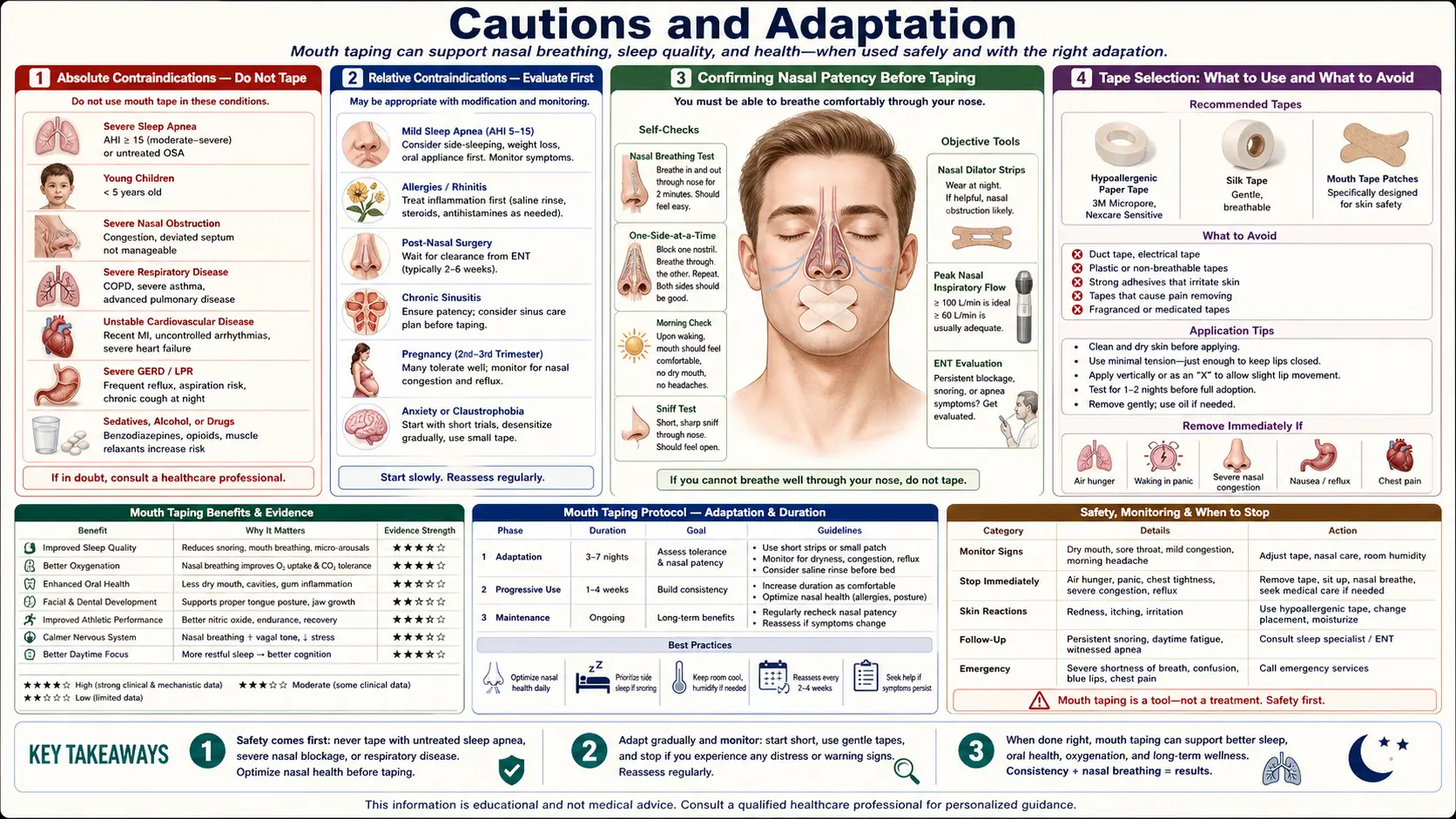
Absolute Contraindications — Do Not Tape
The following are absolute contraindications. Mouth taping should not be attempted under these circumstances under any condition, regardless of how mild the case seems:
- Untreated moderate-to-severe obstructive sleep apnea. See the Snoring and OSA deep dive. Taping does not treat OSA and may delay diagnosis of a serious cardiovascular risk factor.
- Significant nasal obstruction. Severely deviated septum, large nasal polyps, severe chronic rhinitis, or any condition that materially impairs nasal airflow. Taping the mouth closed when the nose is obstructed is a respiratory emergency in waiting.
- Acute upper respiratory infection. Any cold, flu, or sinus infection that has produced significant nasal congestion. Resume taping only after full resolution.
- Recent alcohol consumption or sedative medication. Alcohol, benzodiazepines, opioids, and other CNS depressants reduce arousal response. The protective reflex that would normally cause a person to wake and remove tape if breathing is compromised is blunted. Wait at least 6 hours after alcohol and consult a physician before taping while on sedatives.
- Vomiting risk. Pregnancy with hyperemesis, recent gastroenteritis, history of nocturnal reflux with vomiting, or alcohol intoxication. Aspiration of vomit with a taped mouth is a documented cause of death and is the single most consequential failure mode of mouth taping.
- Severe gastroesophageal reflux disease (GERD). If reflux is severe enough that nocturnal regurgitation occurs, taping the mouth is dangerous. Treat the reflux first.
- Children under 18 without medical supervision. Pediatric airway anatomy, arousal response, and ability to remove tape are different from adults. Several pediatric sleep medicine societies have issued explicit warnings.
- Claustrophobia or significant anxiety about the practice. If the patient cannot tolerate the sensation of mouth closure psychologically, the resulting sleep disturbance and panic risk outweigh any potential benefit.
- Recent oral surgery, lip injury, or active dermatologic disease at the lips. Wait for full healing.
Relative Contraindications — Evaluate First
The following conditions are relative contraindications — they do not categorically rule out mouth taping, but they warrant medical evaluation and case-by-case judgment before starting:
- Suspected but undiagnosed OSA. Witnessed apneas, excessive daytime sleepiness, or other suggestive symptoms. Get a sleep study before considering mouth taping.
- Chronic allergic rhinitis. If nasal symptoms are well-controlled with topical steroids, antihistamines, or immunotherapy, mouth taping may be feasible. If congestion is significant, treat the underlying allergy first.
- Mild deviated septum. Many people have mild septal deviation without significant airflow impairment. Confirm patency (see next section) before taping.
- History of nocturnal panic attacks. Mouth closure can be a trigger for panic in susceptible individuals. Use partial closure techniques (see Application Techniques) and discontinue if panic occurs.
- Sensitive or atopic skin. Adhesive contact dermatitis is the most common minor complication. Use the gentlest available tape and monitor for reactions.
- Lip piercings or oral jewelry. Remove before taping to avoid skin trauma.
- Active CPAP therapy. Mouth taping as a CPAP adjunct to reduce mouth leak is increasingly used but should be discussed with the prescribing sleep medicine physician first.
Confirming Nasal Patency Before Taping
Before attempting any form of mouth taping, the patient must verify that the nose is patent and capable of supporting full minute ventilation. The simplest tests:
- Cottle maneuver. Use a fingertip to gently pull the cheek skin laterally on each side, opening the nasal valve. If breathing dramatically improves, there is a nasal-valve component to the obstruction that needs evaluation.
- One-nostril breathing test. Close one nostril with a finger and breathe normally through the other for 60 seconds. Repeat on the other side. Both sides should support comfortable normal breathing. If one side is significantly more obstructed, evaluate further.
- 30-minute daytime nose-only test. Walk for 30 minutes with the mouth deliberately closed (no tape). If this is comfortable and does not require breaks for mouth breathing, nasal capacity is adequate for resting nighttime use. If air hunger develops, address nasal obstruction first.
- Nasal valve dilator strip trial. Try Breathe Right or similar nasal strips for several nights. If sleep quality and snoring noticeably improve with the strips alone, nasal-valve narrowing is contributing. Strips can be combined with mouth taping in patients with mild nasal-valve issues.
If any of these tests reveals significant nasal obstruction, the appropriate next step is evaluation by an otolaryngologist or allergist — not improvised mouth taping. Common reversible causes include allergic rhinitis (treatable with topical steroids), nasal polyps (treatable with topical steroids or surgery), deviated septum (correctable with septoplasty), inferior turbinate hypertrophy (correctable with conservative or surgical reduction), and chronic sinusitis (treatable medically or surgically).
Tape Selection: What to Use and What to Avoid
Tape selection materially affects safety and tolerability. The relevant criteria:
- Porous. The tape should allow some airflow through itself, so that emergency oral breathing is possible if nasal obstruction develops suddenly during the night.
- Hypoallergenic adhesive. Most quality medical tapes use latex-free hypoallergenic acrylic adhesive. Avoid duct tape, packing tape, and other industrial products designed for permanent bonding.
- Easy to remove. The tape should release cleanly without skin damage. The patient should be able to remove it instantly with one hand if needed.
- Sized for the lips. Strips approximately 25-50 mm wide and 50-100 mm long are typical. Custom-designed mouth strips (3M Micropore, Hostage Tape, Somnifix, Dream Tape) are now widely available.
The most common recommended options:
- 3M Micropore tape. Cheap, widely available, hypoallergenic, easy to release. Cut into appropriate sized pieces. The default starting choice for adults.
- 3M Nexcare or Cover-Roll Stretch. Slightly more aggressive adhesion than Micropore, useful for patients with vigorous nighttime mouth movement.
- Hostage Tape. Pre-cut mouth-shaped strips with a central porous strip, designed specifically for the application. More expensive than improvised Micropore but easier to apply.
- Somnifix. Pre-cut strips with a central breathing slot, designed by sleep medicine physicians. The most extensively marketed product. Modest evidence base.
- Dream Tape, Mouth Strips, generic mouth tape. Many similar products. Vary in adhesive strength and skin tolerability.
Avoid: duct tape, electrical tape, packing tape, athletic tape (too aggressive), waterproof tape (no porosity), any tape designed for industrial rather than medical use. The risk is adhesive injury to the lip skin and inability to remove the tape quickly in an emergency.
Application Techniques (Strip, Cross, Lip-Center)
There are three commonly used application patterns, in increasing order of mouth-closure aggressiveness:
- Vertical strip (lip-center). A single vertical strip of tape approximately 25 mm wide placed centrally over the closed lips, from just below the nose to just above the chin. This leaves the corners of the mouth uncovered, allowing some emergency airflow and easier removal. The least restrictive option, recommended for beginners and for patients with any uncertainty about tolerance.
- Horizontal strip (full-lip). A single horizontal strip approximately 50 mm wide covering the entire lip line. More complete mouth closure than the vertical strip. Recommended after the patient has tolerated the vertical strip for several weeks.
- Cross pattern (X) or pre-cut product. Two strips crossed over the lips, or a pre-cut mouth-shaped product like Hostage Tape that combines coverage of the full lip line with engineered porosity. The most complete closure. Use only after extended tolerance has been demonstrated with the simpler patterns.
Application steps:
- Wash and dry the lips and surrounding skin before bed. Avoid lip balm immediately before application (it reduces adhesion).
- If using improvised tape, cut to size beforehand.
- Close the mouth in resting position with the tongue on the palate.
- Apply the tape with light pressure. Do not stretch the tape over the lips; this can cause skin pulling and discomfort.
- Confirm that the tape can be removed easily with one hand by lifting one corner with a finger.
- Lie down and breathe normally through the nose for several minutes before falling asleep. If air hunger develops, remove the tape immediately.
The Graduated Adaptation Protocol
The single biggest cause of mouth-taping failure is starting too aggressively. The recommended graduated protocol takes 4-8 weeks and is designed to build tolerance progressively:
- Week 1: Daytime awareness only. No taping. During the day, consciously practice nose-only breathing for 1-2 hours per day. Begin Control Pause tracking (see Daytime Breathing Habits).
- Week 2: Daytime tape trial. Wear a small piece of tape (vertical strip) for 15-30 minutes during the day while doing low-intensity activities. Confirm comfort and confirm the ability to remove instantly.
- Week 3: Naps and short sleep. Wear the vertical strip during a 1-2 hour daytime nap. If well tolerated, progress to wearing during the first 2 hours of nighttime sleep, removing if you wake up.
- Week 4: Full nighttime vertical strip. Begin full-night use of the vertical strip. Many patients find this is the endpoint — the vertical strip is enough.
- Weeks 5-6: Progress to horizontal strip or pre-cut product. If the vertical strip is well tolerated and the patient is still noticing mouth opening during sleep (e.g., dry mouth on waking, tape displaced in the morning), progress to a more complete closure.
- Weeks 7-8: Stable use or progressive discontinuation. Most patients who have followed the protocol and concurrently retrained daytime breathing find that the tape becomes unnecessary — nasal breathing has become the autonomic default and continues into sleep without external prompting.
If at any stage the patient experiences poor sleep, repeated tape removal during the night, panic, or significant air hunger, drop back to the previous stage and proceed more slowly. Some patients will not tolerate any tape, and that is a legitimate outcome — for these patients, the daytime retraining work is the appropriate intervention.
Skin Reactions and Lip Care
Adhesive contact dermatitis is the most common minor complication of mouth taping. It usually manifests as mild redness, dryness, or itching on the lip skin where the tape contacts. Less commonly, true allergic contact dermatitis with vesicles or blistering can occur.
Prevention and management:
- Rotate tape position slightly each night so the same skin area is not stressed repeatedly
- Use the gentlest available hypoallergenic tape (3M Micropore is the gold standard)
- Apply a thin layer of lanolin or petrolatum to the lips (not the surrounding skin) at bedtime for moisturization — avoid applying where tape will contact, as it reduces adhesion
- If mild irritation occurs, take a several-night break and use a different brand of tape on resumption
- If true allergic dermatitis occurs (vesicles, marked redness, swelling), discontinue and consult a dermatologist
Some patients develop mild perioral dryness or chapping from the dehydration of the lip skin under the occlusive tape. A thicker barrier of lanolin or a lip balm specifically tolerated on the relevant areas of skin usually resolves this.
When to Discontinue
The following signals should trigger discontinuation of mouth taping and reassessment:
- Repeated overnight tape removal. If the patient consistently removes the tape unconsciously during the night, the body is signaling that the practice is not tolerated. Force is the wrong response.
- Worsening daytime sleepiness. If subjective sleep quality declines after starting taping, the practice may be inducing arousals rather than improving sleep.
- New or worsening snoring. Closing the mouth in a patient who actually has mouth-breathing-compensated airway anatomy can paradoxically increase nasal-airway turbulence and produce nasal snoring or worsened OSA. A sleep study before and after is the gold standard for evaluation.
- Witnessed apneas. If a bed partner reports new or worsening breathing pauses after starting tape, discontinue immediately and obtain a sleep study.
- Morning headaches. A new pattern of morning headaches can indicate occult hypercapnia or untreated OSA — both reasons to stop and evaluate.
- Panic or anxiety. If wearing the tape consistently provokes anxiety, the psychological cost outweighs the physiological benefit.
- Skin breakdown. Significant dermatitis or breakdown of lip skin warrants discontinuation while the skin heals.
- Intercurrent illness. Stop during any upper respiratory infection, even mild colds, and resume only after full resolution.
The decision to discontinue is not a failure. Mouth taping is a tool, not a goal. Many patients achieve durable nasal-breathing autonomy through daytime retraining alone and never need the tape. Others find that the tape is a useful short-term scaffold that becomes unnecessary after several weeks. A small number find they do not tolerate it and do better with other interventions (nasal-valve dilators, mandibular advancement, CPAP for OSA, allergy treatment for rhinitis). All of these are legitimate outcomes.
Special Populations (Children, Pregnancy, Elderly)
Children. Mouth taping in pediatric patients is controversial. The American Academy of Pediatric Dentistry and several sleep medicine societies have explicitly cautioned against improvised mouth taping in children. Pediatric airway physiology, arousal response, and ability to remove tape in an emergency are different from adults. If a child has habitual mouth breathing, the appropriate evaluation is by a pediatric sleep medicine physician, ENT, or orofacial myofunctional therapist — not improvised home taping. Common reversible causes in children include adenoid hypertrophy (most common), allergic rhinitis, and tongue-tie.
Pregnancy. Pregnancy is associated with several factors that complicate mouth taping: increased risk of GERD and nocturnal regurgitation (relative contraindication if symptomatic), increased nasal congestion (rhinitis of pregnancy), and increased risk of vomiting in the first trimester. Mouth taping during pregnancy is not categorically prohibited but should be approached cautiously and discontinued at any sign of regurgitation or persistent nasal congestion. Discuss with obstetrician.
Elderly. Older adults have higher prevalence of OSA, GERD, polypharmacy (including sedating medications), reduced arousal response, and reduced manual dexterity for tape removal. Mouth taping in elderly patients should generally be done only after a sleep study has ruled out significant OSA and with a partner present in the home.
Patients with neurological disease. Stroke, Parkinson's disease, ALS, advanced dementia, and any condition that impairs swallowing, arousal, or manual dexterity is a relative contraindication. These patients are at higher risk of aspiration if regurgitation occurs and may be unable to remove tape in an emergency.
Patients with central sleep apnea. Central apnea (the brain fails to signal a breath) is fundamentally different from obstructive apnea (the airway collapses). Central sleep apnea is associated with heart failure, opioid use, high-altitude living, and certain neurological conditions. Mouth taping does not address central apnea and may delay recognition. Witnessed apneas without snoring are particularly suspicious for central rather than obstructive events.
Key Research Papers
- Lee YC, Lu CT, Cheng WN, Li HY. The impact of mouth-taping in mouth-breathers with mild OSA Search PubMed
- Huang TW, Young TH. Novel porous oral patches for mild to moderate OSA Search PubMed
- Patil SP, Ayappa IA, et al. AASM CPG for treatment of adult OSA with PAP — PMID 30736887
- Friedman M, et al. Impact of nasal obstruction on OSA Search PubMed
- Mickelson SA. Nasal surgery for OSA syndrome Search PubMed
- Choi JE, Waddell JN, Lyons KM, Kieser JA. Intraoral pH and temperature during sleep with and without mouth breathing Search PubMed
- Gozal D, Kheirandish-Gozal L. The multiple challenges of OSA in children Search PubMed
- Guilleminault C, Huang YS. From oral facial dysfunction to dysmorphism and the onset of pediatric OSA — PMID 29103943
- Brockmann PE, et al. Prevalence of habitual snoring and neurocognitive consequences in children Search PubMed
- Camacho M, Certal V, et al. Myofunctional therapy to treat OSA: systematic review and meta-analysis — PMID 25348130
- Bonuck K, Freeman K, Chervin RD, Xu L. Sleep-disordered breathing in a population-based cohort: behavioral outcomes at 4 and 7 years — PMID 22392181
- Olsen KD, Kern EB, Westbrook PR. Sleep and breathing disturbance secondary to nasal obstruction PubMed: Olsen nasal obstruction
Connections
- Mouth Taping (Main Hub)
- Benefits Deep Dive Hub
- Nasal Breathing Benefits
- Snoring and Sleep Apnea
- Daytime Breathing Habits
- Sleep Hygiene
- Breathwork
- Obstructive Sleep Apnea
- Sinusitis
- GERD (Reflux)
- All Remedies