Snoring and Sleep Apnea
The single biggest source of confusion in the popular mouth-taping conversation is the conflation of snoring (a primarily mechanical noise problem) with obstructive sleep apnea (a serious medical condition with measurable cardiovascular consequences). The evidence base for mouth closure in mild snoring is modest but real; the evidence base for mouth taping as monotherapy for moderate-to-severe OSA is essentially nonexistent, and the American Academy of Sleep Medicine has repeatedly stated that CPAP, mandibular advancement, or surgical intervention are the validated therapies. This deep dive walks through what the evidence actually shows, how to interpret a sleep study, and the narrow population for whom porous-strip mouth closure is a reasonable adjunct.
Interactive Visualization Sleep Apnea — collapse the airway, then splint it open with CPAP Watch the throat close as sleep deepens, the chest heave against a shut airway and oxygen slide into the 80s — then switch on CPAP and see the whole night go quiet. Launch →
Table of Contents
- Snoring vs. Sleep Apnea — They Are Not the Same Thing
- The Mechanics of Snoring
- The Mechanics of Obstructive Sleep Apnea
- The Evidence Base for Mouth Taping in Snoring and OSA
- The Lee 2015 Singapore Trial
- The Huang 2015 Porous Oral Patch Trial
- When to Get a Sleep Study
- The AASM Position and Why It Matters
- Mouth Taping as a CPAP Adjunct, Not a Substitute
- Key Research Papers
- Connections
- Featured Videos
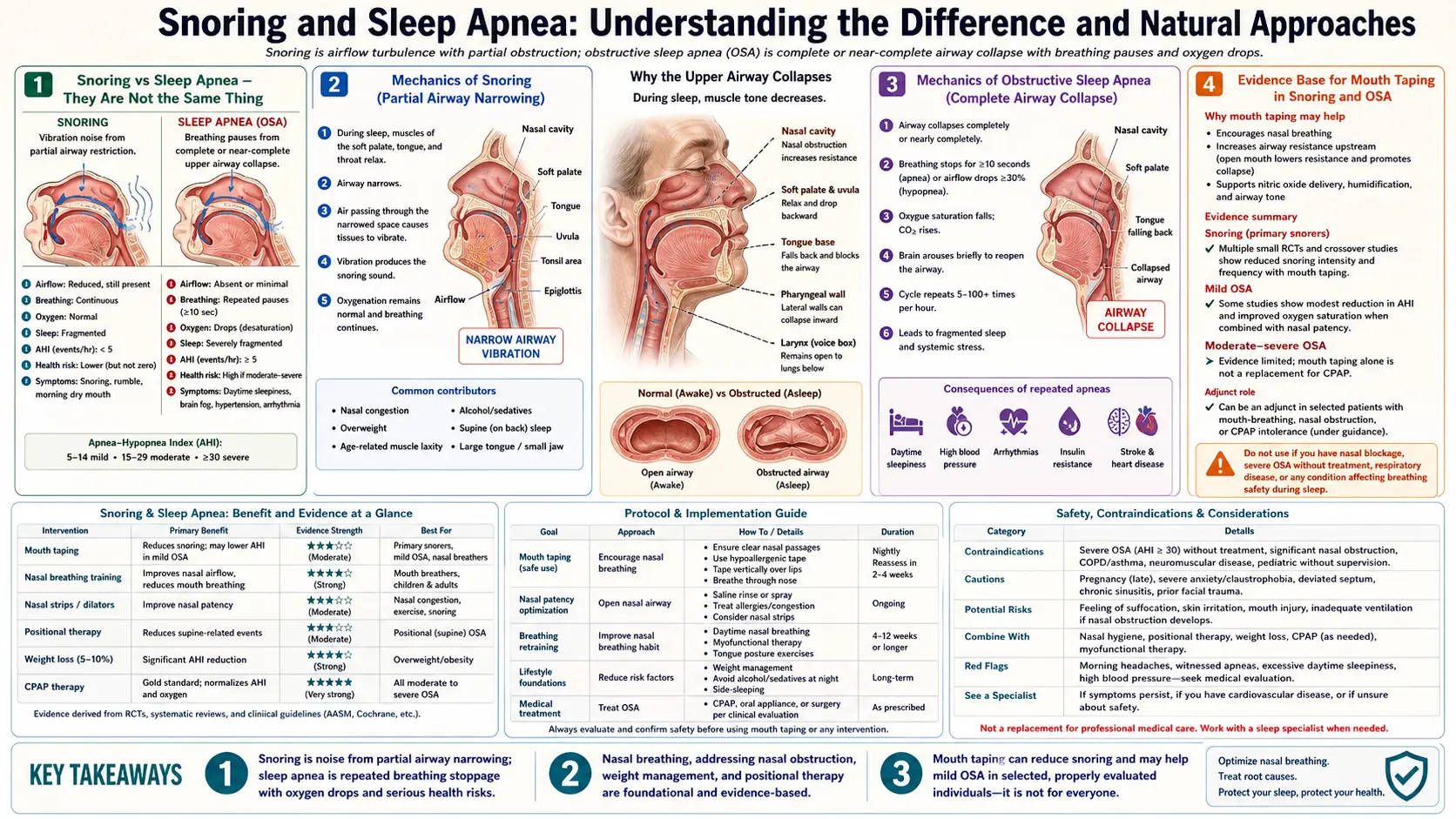
Snoring vs. Sleep Apnea — They Are Not the Same Thing
Snoring is the audible vibration of soft tissues in the upper airway during sleep. It is a mechanical phenomenon, not a medical diagnosis. Snorers may be asymptomatic, with normal oxygen saturation throughout the night, normal apnea-hypopnea index, and no measurable cardiovascular consequences. They simply make noise, which is primarily a problem for bed partners.
Obstructive sleep apnea is a categorically different condition. It is defined by recurrent episodes of complete or near-complete upper-airway collapse during sleep, with associated oxygen desaturation, arousal from sleep, and a cascade of downstream cardiovascular and metabolic consequences. The defining metric is the apnea-hypopnea index (AHI), the number of apnea or hypopnea events per hour of sleep:
- Normal: AHI less than 5 events per hour
- Mild OSA: AHI 5-14 events per hour
- Moderate OSA: AHI 15-29 events per hour
- Severe OSA: AHI 30 or more events per hour
OSA is associated with markedly increased risk of hypertension (especially treatment-resistant hypertension), atrial fibrillation, heart failure, stroke, type 2 diabetes, and motor vehicle crashes from daytime sleepiness. Untreated severe OSA increases all-cause mortality by approximately 50%. CPAP treatment substantially reverses many of these risks. This is one of the best-studied and most consequential chronic medical conditions in adult medicine.
The categorical distinction matters because the popular mouth-taping conversation often blurs the two: a partner reports loud snoring, the snorer tapes their mouth, the snoring decreases (or shifts to nasal snoring of a different timbre), and everyone declares success. But if the snorer in fact has moderate-to-severe OSA, the underlying disease has not been treated — the noise has merely been quieter. The apnea events, the oxygen desaturations, and the cardiovascular damage continue.
The Mechanics of Snoring
Snoring is generated by vibration of the soft palate, the uvula, the pharyngeal walls, the tongue base, and (less commonly) the epiglottis during inspiration. The conditions required for snoring are:
- A partially narrowed upper airway (commonly from soft palate elongation, tongue base prominence, retrognathic mandible, or obesity-related pharyngeal narrowing)
- Reduced muscle tone during sleep (especially during REM sleep, when skeletal muscle paralysis is most pronounced)
- Sufficient inspiratory flow velocity to cause turbulent vibration of the relaxed soft tissues
Open-mouth sleep dramatically increases snoring risk by two mechanisms: (a) the mandible drops down and back, narrowing the pharyngeal space and bringing the tongue base closer to the posterior pharyngeal wall; and (b) the open mouth removes the seal between oral and nasal cavities, allowing inspiratory flow to take the path of least resistance through the mouth, which produces faster less-conditioned airflow over the vibrating soft palate.
Closing the mouth shifts inspiration through the nose. Nasal flow is slower (because of the higher resistance), more laminar, and tends to be directed away from the vibrating soft palate. In a substantial fraction of snorers, this mechanical change is enough to eliminate or substantially reduce snoring. This is the well-established physiological basis for chin straps, mandibular advancement devices, and (in the popular literature) mouth taping.
The Mechanics of Obstructive Sleep Apnea
OSA is not just loud snoring — it is recurrent airway collapse. The pharyngeal airway is a collapsible tube with no rigid skeletal support (unlike the trachea, which has cartilage rings). During wakefulness, the genioglossus and other pharyngeal dilator muscles maintain airway patency through tonic activation. During sleep, this tonic activity decreases. In susceptible individuals (anatomically narrowed airway, increased pharyngeal collapsibility, obesity-related compression, or reduced ventilatory drive), the airway collapses partially (hypopnea) or completely (apnea) during inspiration.
The collapse triggers a stereotyped sequence: respiratory effort against the closed airway, progressive hypoxemia, increasing sympathetic activation, and eventually a brief cortical arousal that restores muscle tone and reopens the airway. The patient may resume breathing with a loud gasp or snort. They typically have no memory of the event. The cycle repeats hundreds of times per night in severe OSA.
The repetitive arousals fragment sleep architecture, reducing time in deep slow-wave sleep and REM. The repetitive hypoxemia-reoxygenation cycles drive oxidative stress, endothelial dysfunction, sympathetic hyperactivity, and chronic systemic inflammation. These are the mechanisms behind the documented cardiovascular and metabolic consequences.
The critical point for mouth taping: closing the mouth does not address any of the underlying anatomy or collapsibility. A patient with severe OSA who tapes their mouth still has a collapsible pharyngeal airway, still has the same anatomical risk factors, and will continue to apnea regardless of which orifice they would otherwise be breathing through. The intervention is mismatched to the mechanism. The validated interventions for OSA — CPAP, mandibular advancement, hypoglossal nerve stimulation, weight loss, surgical airway expansion — all address either airway pressure or anatomy directly.
The Evidence Base for Mouth Taping in Snoring and OSA
The peer-reviewed literature on mouth taping per se is small. A PubMed search returns fewer than two dozen relevant papers. The two most-cited studies are Lee 2015 (Singapore) and Huang 2015 (Taiwan), both of which used porous oral patches (specifically engineered mouth-closure devices, not improvised medical tape) in carefully selected populations.
The composite picture from the available evidence:
- Mild snoring (no OSA): Mouth closure produces a measurable reduction in snoring frequency and intensity in a substantial fraction of snorers. Effect size is modest but real. Patient satisfaction is generally high.
- Mild OSA (AHI 5-14): Mouth closure produces small but statistically significant reductions in AHI in selected patients, primarily those with mouth-breathing-dominant phenotypes. The effect size is much smaller than CPAP and would not be considered curative.
- Moderate-to-severe OSA (AHI ≥ 15): No evidence of benefit as monotherapy. Mouth taping should not delay or replace CPAP, mandibular advancement, or other validated therapy in this population.
- Patients on CPAP already: Mouth taping is sometimes used as an adjunct to reduce mouth leak in patients using nasal CPAP. This is a different clinical question from monotherapy.
The Lee 2015 Singapore Trial
Lee YC and colleagues published in Healthcare (Basel) 2022 (often cited as "Lee 2015" based on the trial period) a prospective study of porous oral patches in patients with mild OSA. The study enrolled 20 patients with mild OSA (AHI 5-15) confirmed on baseline polysomnography. All patients had subjective mouth breathing during sleep and were not on CPAP.
The intervention was a custom porous oral patch worn during a single overnight polysomnography. The primary outcome was change in AHI compared with the baseline study. The published results showed:
- Median AHI decreased from baseline values into a lower range, with statistically significant reduction in the intervention night
- Snoring index decreased substantially
- Subjective sleep quality improved
- No serious adverse events were reported during the single supervised night
The study is the most-cited piece of evidence in favor of mouth taping for snoring and mild OSA. The important limitations are: small sample, mild OSA only, single-night observation (no long-term follow-up), and the use of a custom porous patch rather than improvised tape from a hardware store. The signal is real, but it does not generalize to moderate or severe OSA, and it does not validate any specific product available for purchase by consumers.
The Huang 2015 Porous Oral Patch Trial
Huang TW and Young TH published in Otolaryngology-Head and Neck Surgery 2015 a study of a novel porous oral patch in 30 patients with mild-to-moderate OSA. The patch was specifically designed to maintain mouth closure while allowing emergency oral airflow if nasal obstruction occurred.
The results showed a roughly 47% reduction in median AHI from baseline to intervention night, with no significant change in nadir oxygen saturation. The snoring index decreased by approximately 50%. The authors concluded that the porous oral patch was a viable adjunctive treatment in mild-to-moderate OSA with documented mouth-breathing phenotype.
This study is technically the strongest single piece of evidence for mouth closure as a therapeutic intervention. The same caveats apply: small sample, single-night observation, custom-engineered patch rather than off-the-shelf tape, and exclusion of severe OSA. The authors explicitly noted that the patch should not be considered first-line therapy for OSA and was being evaluated as an adjunct or alternative for patients intolerant of CPAP.
When to Get a Sleep Study
Anyone who is considering mouth taping for snoring or suspected sleep-disordered breathing should first determine whether they have OSA. The diagnostic gold standard is in-laboratory polysomnography (PSG), but home sleep apnea testing (HSAT) is now widely available, less expensive, and adequate for most patients with high pretest probability.
The clinical signs that should trigger a sleep study before any consideration of mouth taping:
- Witnessed apneas (partner reports breathing pauses or gasping during sleep)
- Loud habitual snoring (heard from outside the bedroom)
- Excessive daytime sleepiness (Epworth Sleepiness Scale 11 or higher)
- Morning headaches, dry mouth, or sore throat
- Nocturnal gasping or choking
- Treatment-resistant hypertension
- Atrial fibrillation, especially nocturnal
- BMI 30 or higher
- Neck circumference greater than 17 inches (men) or 16 inches (women)
- Mallampati class III or IV oropharyngeal anatomy
If a sleep study returns AHI less than 5 with normal oxygen saturation and the patient's problem is primary snoring, mouth taping (in the absence of contraindications — see Cautions and Adaptation) is a reasonable conservative intervention. If the study shows OSA at any severity, mouth taping is at best an adjunct, never a substitute for validated therapy.
The AASM Position and Why It Matters
The American Academy of Sleep Medicine has published clinical practice guidelines for the treatment of adult obstructive sleep apnea (Patil et al. Journal of Clinical Sleep Medicine 2019). The guidelines are explicit: positive airway pressure (CPAP, BPAP, APAP) is first-line therapy for moderate-to-severe OSA. Mandibular advancement devices are recommended as an alternative for patients with mild-to-moderate OSA who cannot tolerate PAP. Surgical interventions (uvulopalatopharyngoplasty, hypoglossal nerve stimulation, maxillomandibular advancement) are reserved for specific anatomical phenotypes.
Mouth taping does not appear in the AASM guidelines as a recommended therapy at any severity. The American Academy of Sleep Medicine in 2023 published a position statement explicitly cautioning that mouth taping is not a validated treatment for OSA and that delays in evaluation due to self-treatment with mouth taping have potential for harm.
This is not a dismissal of the underlying physiology — nasal breathing during sleep is unambiguously better than oral breathing for the reasons enumerated in the Nasal Breathing Benefits deep dive. The AASM position is specifically that mouth closure does not address the anatomical and collapsibility issues that drive OSA, and that patients with witnessed apnea or other suggestive symptoms need a proper diagnostic workup and validated treatment.
Mouth Taping as a CPAP Adjunct, Not a Substitute
One legitimate clinical use case for mouth taping is in patients already established on nasal CPAP who have problems with mouth leak. Mouth leak during CPAP occurs when the soft palate falls during sleep and the high-pressure nasal flow escapes through the open mouth, reducing effective airway pressure, causing dry mouth, and triggering arousals.
The conventional solutions are: (a) switch from nasal mask to full-face mask, which often increases mask leak and reduces comfort, or (b) add a chin strap, which is uncomfortable for many patients. Some sleep medicine practitioners use porous mouth tape as a third option to maintain mouth closure during nasal CPAP without the bulk of a full-face mask or chin strap. This use case is off-label but is increasingly described in the clinical literature.
Importantly, this is a different question from monotherapy. In the CPAP-adjunct case, the patient is receiving validated OSA therapy and using tape to optimize delivery of that therapy. In the monotherapy case, the patient is using tape instead of validated therapy and risking the cardiovascular consequences of untreated OSA. The two scenarios should not be conflated.
Key Research Papers
- Lee YC, Lu CT, Cheng WN, Li HY. The impact of mouth-taping in mouth-breathers with mild obstructive sleep apnea (Healthcare 2022) — Search PubMed
- Huang TW, Young TH. Novel porous oral patches for patients with mild OSA and mouth breathing (Otolaryngol Head Neck Surg 2015) — Search PubMed
- Meurice JC, Marc I, Carrier G, Series F. Effects of mouth opening on upper airway collapsibility Search PubMed
- Kim EJ, Choi JH, et al. The impacts of open-mouth breathing on upper airway space in OSA Search PubMed
- Fitzpatrick MF, McLean H, et al. Effect of nasal or oral breathing route on upper airway resistance during sleep — PMID 12882467
- Koutsourelakis I, Vagiakis E, Roussos C, Zakynthinos S. OSA and oral breathing in patients free of nasal obstruction Search PubMed
- Patil SP, Ayappa IA, et al. AASM clinical practice guideline for the treatment of adult OSA with positive airway pressure — PMID 30736887
- Madronio MR, et al. Older individuals have increased oro-nasal breathing during sleep Search PubMed
- Friedman M, et al. Impact of nasal obstruction on OSA Search PubMed
- Georgalas C. The role of the nose in snoring and OSA: an update Search PubMed
- Yu JL, Rosen I. Utility of the modified Mallampati grade in the assessment of OSA Search PubMed
- Brockmann PE, et al. Prevalence of habitual snoring and neurocognitive consequences in children Search PubMed
Connections
- Sleep Apnea: Why Breathing Stops at Night — interactive animation
- Mouth Taping (Main Hub)
- Benefits Deep Dive Hub
- Nasal Breathing Benefits
- Daytime Breathing Habits
- Cautions and Adaptation
- Obstructive Sleep Apnea
- Sleep Hygiene
- Breathwork
- Sinusitis
- Atrial Fibrillation
- Hypertension