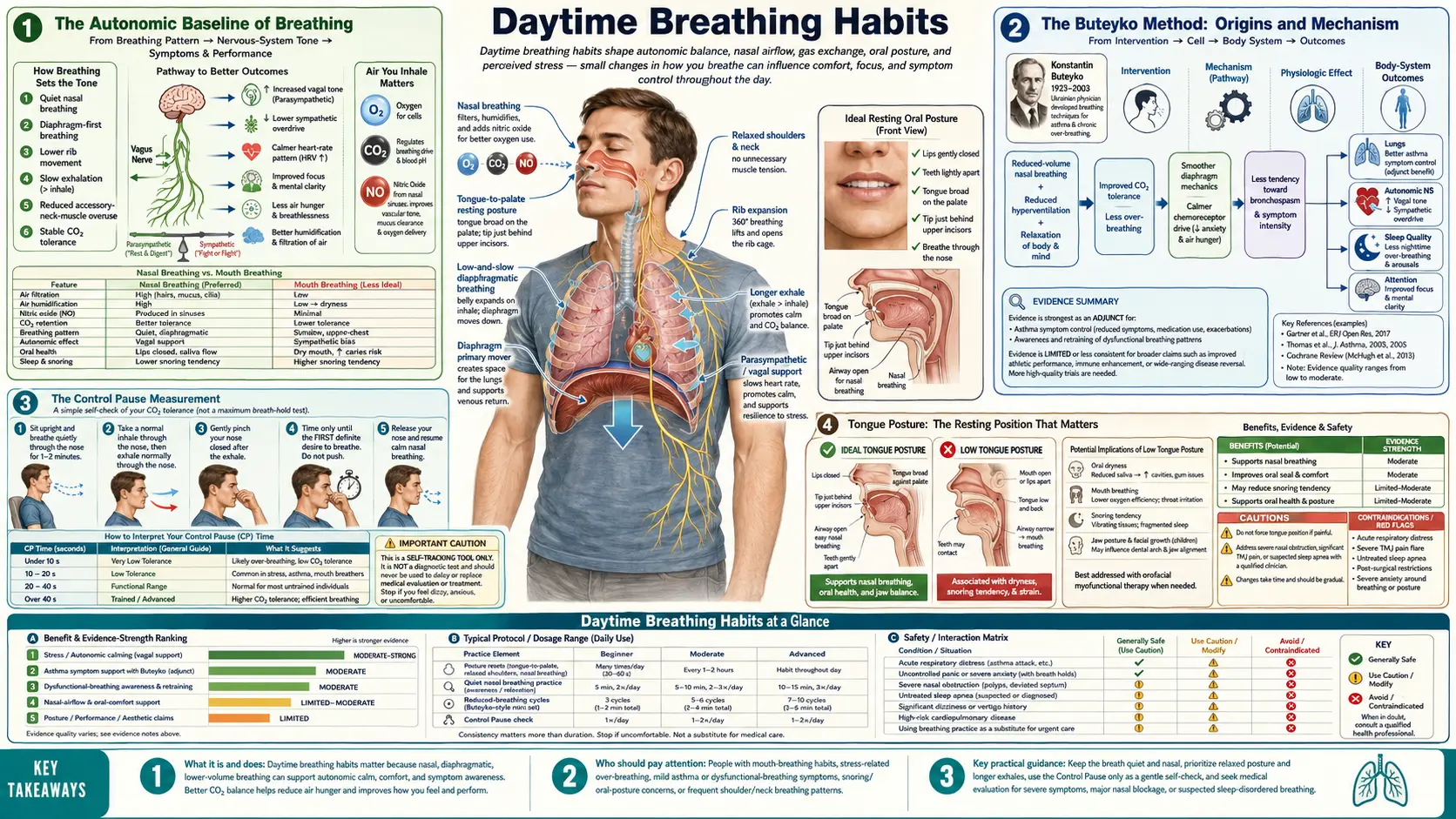
Daytime Breathing Habits
The single most overlooked point in the popular mouth-taping conversation is that nighttime taping rarely produces durable benefit if daytime breathing remains mouth-dominant. The autonomic baseline that determines whether the body defaults to nasal or oral breathing during sleep is set by the prevailing pattern during the 16 waking hours, not by the eight sleeping hours. Retraining that baseline is the higher-leverage intervention. This deep dive walks through the Buteyko Control Pause measurement, the tongue-posture work popularized by Mike Mew and the "mewing" community, slow diaphragmatic nasal breathing protocols, and the daytime practices that make nighttime taping unnecessary.
Table of Contents
- The Autonomic Baseline of Breathing
- The Buteyko Method: Origins and Mechanism
- The Control Pause Measurement
- Tongue Posture: The Resting Position That Matters
- "Mewing" and Orthotropic Theory
- Diaphragmatic Breathing Mechanics
- Slow Breathing at 6 Breaths Per Minute
- Exercise with Nose-Only Breathing
- A Practical Daily Protocol
- Key Research Papers
- Connections
- Featured Videos
The Autonomic Baseline of Breathing
The brainstem respiratory pattern generator (the pre-Bötzinger complex in the medulla, with input from the parabrachial complex in the pons) sets a baseline respiratory rate and depth that the body defaults to in the absence of conscious override. This baseline is plastic — it can be modified by training over weeks to months, but it is highly resistant to acute intervention.
The relevant features of this baseline:
- Tidal volume and rate. Healthy resting tidal volume is approximately 500 mL with a rate of 12-16 breaths per minute, yielding minute ventilation of 6-8 L/min. Chronic mouth breathers tend toward larger tidal volume (700+ mL) and higher rate (18+ breaths/min), with minute ventilation in the 10-15 L/min range — well into the hyperventilation range during what they consider rest.
- End-tidal CO2. Healthy end-tidal CO2 (a proxy for arterial PaCO2) is approximately 40 mmHg. Chronic hyperventilators run in the 30-35 mmHg range, which over time resets the chemoreceptor threshold and perpetuates the hyperventilation pattern.
- Inspiration-to-expiration ratio. Resting I:E is approximately 1:2. Stressed/anxious breathers shift toward 1:1 or even inspiration-dominant 2:1 patterns. Slow relaxation breathing deliberately shifts to 1:3 or 1:4.
- Default nasal or oral. The brainstem also sets a default airway preference based on chronic learning. Patients with childhood adenoid hypertrophy, chronic allergic rhinitis, or chronic mouth breathing often retain an oral-default pattern even after the original obstruction is resolved.
Mouth taping addresses the eight sleeping hours. If the patient spends the other sixteen hours mouth-breathing, the brainstem default remains oral, and the tape is doing all the work to override a deeply ingrained pattern. The result is often poor sleep, tape removal during the night, or relapse to mouth breathing the moment the tape comes off. Retraining the daytime baseline so that nasal breathing is the autonomic default makes nighttime taping superfluous — the body simply continues nasal breathing into sleep on its own.
The Buteyko Method: Origins and Mechanism
Konstantin Buteyko was a Soviet physiologist (1923-2003) who developed his breathing method in the 1950s at the Institute of Experimental Biology and Medicine in Novosibirsk. His central observation was that asthma patients, anxiety patients, and patients with a wide range of chronic conditions all chronically hyperventilated — their minute ventilation at rest was 2-3 times the textbook normal of 6 L/min. Buteyko proposed that this chronic hyperventilation produced a low arterial PaCO2, which via the Bohr effect reduced peripheral oxygen delivery despite high oxygen saturation, and via the smooth-muscle effects of low CO2 produced bronchoconstriction (the asthma mechanism) and cerebral vasoconstriction (the anxiety mechanism).
The method itself is a graduated training program designed to normalize the chemoreceptor threshold and reduce minute ventilation back to physiological baseline. The core elements:
- Obligate nasal breathing. All breathing during the day and night through the nose. Mouth taping is sometimes used as an interim measure, but the goal is autonomic nasal default.
- Reduced-volume breathing. Conscious practice of breathing more slowly and shallowly than feels natural, deliberately tolerating mild air hunger as the chemoreceptor threshold resets.
- Control Pause exercises. Daily measurement and progressive extension of the breath-hold after normal exhale (see next section).
- Posture and movement. Upright posture, walking with breath-holds, and gentle exercise with nose-only breathing.
The method has the most evidence for asthma. Bowler et al. (1998), Cooper et al. (2003), McHugh et al. (2003), and Bruton and Lewith (2005 systematic review) all documented meaningful reductions in inhaler use, exacerbation frequency, and asthma symptoms with structured Buteyko training compared with controls. The evidence in other indications (anxiety, sleep apnea, hypertension) is thinner and largely from non-randomized case series.
The most accessible modern resource is Patrick McKeown's Buteyko Clinic International, which has trained thousands of practitioners worldwide and published several popular books (The Oxygen Advantage, Close Your Mouth). Mike Maher and others have produced freely available video instruction on YouTube.
The Control Pause Measurement
The Control Pause (CP) is Buteyko's simple and reproducible measurement of CO2 tolerance. The protocol:
- Sit upright, relaxed, breathing normally through the nose for 2-3 minutes
- At the end of a normal, unforced exhale (not a deep exhale), pinch the nose closed
- Start a stopwatch
- Hold the breath until you feel the first definite urge to breathe (not until maximum endurance)
- Release the nose and resume normal nasal breathing — the first breath after release should feel smooth and unforced, not a gasp. If you gasp or take an oversized first breath, you held too long and the measurement is invalid.
The number of seconds is the Control Pause. Buteyko's benchmarks:
- CP < 10 seconds: severe chronic hyperventilation, typically associated with active asthma, panic disorder, or sleep apnea
- CP 10-20 seconds: moderate hyperventilation, common in mouth breathers and chronic snorers
- CP 20-40 seconds: mild hyperventilation or low-normal CO2 tolerance
- CP 40-60 seconds: healthy normal CO2 tolerance
- CP > 60 seconds: excellent CO2 tolerance, characteristic of trained breath workers, athletes, and Buteyko practitioners
The CP is meant to be measured daily, on waking before any food or stimulants, and trended over weeks. Progress is typically slow but steady — 1-2 seconds per week is realistic with consistent practice. A CP that doubles from 15 to 30 seconds over 6 months is a meaningful change in chemoreceptor threshold and usually correlates with subjective reductions in anxiety, snoring, exercise-induced bronchoconstriction, and daytime mouth breathing.
The CP also has prognostic value for nighttime mouth taping. Patients with CP under 15 seconds frequently cannot tolerate full mouth closure during sleep — they wake repeatedly with air hunger and tear the tape off. Patients with CP over 30 seconds tape easily and usually find they no longer need the tape after a few weeks because nasal breathing has become the autonomic default.
Tongue Posture: The Resting Position That Matters
The position of the tongue at rest is closely linked to whether the mouth defaults to open or closed. The physiologically correct resting tongue posture, sometimes called the "myofunctional rest position," is:
- The entire tongue (not just the tip) resting against the roof of the mouth, with light suction holding it against the palate
- The tip of the tongue resting just behind the upper front teeth at the alveolar ridge (the "palatine spot" where saying the letter "N" places the tongue)
- The teeth lightly together or separated by 1-2 mm (not clenched, not gapped widely)
- The lips lightly sealed
In this resting posture, the mouth is mechanically sealed for nasal breathing. The tongue physically blocks the oral airway by occupying the entire oral cavity, and the lip seal prevents air leak around the teeth.
Chronic mouth breathers usually have an aberrant resting tongue posture: the tongue rests on the floor of the mouth, the jaw drops slightly open, and the lips remain parted. This posture mechanically encourages mouth breathing because the oral airway is open. Recognizing and correcting the tongue posture during the day is, for many patients, more effective than mouth taping at night.
The simplest awareness exercise: throughout the day, periodically check — is my tongue on the roof of my mouth or on the floor? Is my mouth closed or slightly open? Most people who do this discover that their tongue is on the floor and their mouth is parted 80% of the time. Conscious correction, repeated dozens of times per day for several weeks, gradually shifts the autonomic default.
"Mewing" and Orthotropic Theory
The popular term "mewing" refers to the resting tongue-posture work developed by the British orthodontists John Mew and Mike Mew (father and son). Their orthotropic theory holds that craniofacial development — specifically the forward and outward growth of the maxilla — is shaped by the constant low-grade outward pressure of the tongue against the palate. Loss of correct tongue posture (from chronic mouth breathing, pacifier use, thumb sucking, soft modern diets requiring little chewing) leads to underdevelopment of the maxilla, narrow palate, retrognathic mandible, crowded teeth, and the "long face syndrome" with associated obstructive sleep-disordered breathing.
The clinical Mew approach in children is the "Biobloc" appliance, which aims to encourage forward maxillary growth. In adults, the orthotropic position is that the skeletal pattern is largely fixed but that resting tongue posture and breathing pattern can still be corrected, with secondary benefits for daytime alertness, sleep quality, and the soft-tissue facial appearance.
The orthotropic theory is not part of mainstream orthodontic teaching, and the long-term skeletal claims in adults are not well-supported by randomized data. However, the tongue-posture component — that the tongue should rest against the palate and the lips should rest sealed — is consistent with the orofacial myology and speech-language pathology literature, and is a useful daytime practice regardless of the larger theory.
The mainstream-medicine equivalent is myofunctional therapy, an established discipline practiced by speech-language pathologists and physical therapists specifically trained in orofacial muscle retraining. Camacho et al. (Sleep 2015) published a meta-analysis showing modest reductions in AHI with structured myofunctional therapy for OSA, particularly in children.
Diaphragmatic Breathing Mechanics
Diaphragmatic breathing — sometimes called "belly breathing" or "abdominal breathing" — is the natural breathing pattern of healthy infants and is the most efficient pattern at rest. The diaphragm descends on inspiration, displacing the abdominal viscera downward and outward, while the lower ribs flare slightly. The upper chest does not visibly move at rest. This pattern uses approximately 70% of the muscular effort of breathing for approximately 80% of the air movement — high mechanical efficiency.
The dysfunctional alternative is chest-wall breathing, sometimes called "clavicular breathing" or "thoracic breathing." The upper chest visibly rises with each breath, the shoulders elevate, and the accessory muscles of inspiration (scalenes, sternocleidomastoid, pectoralis minor) are recruited even at rest. The diaphragm contributes minimally. This pattern is mechanically inefficient (high muscular cost per liter of air), is associated with chronic neck and shoulder tension, and tends to drive faster shallower breathing — the hyperventilation pattern.
The simplest assessment: place one hand on the upper chest, one hand on the belly just below the ribs. Breathe normally for 30 seconds. Which hand moves more? If the upper chest hand moves more, the pattern is dysfunctional chest-wall breathing. If the belly hand moves more, the pattern is functional diaphragmatic breathing. Most chronic mouth breathers will discover they are chest-wall breathing.
Correction: deliberately practice 5-10 minutes per day of slow nasal breathing with conscious belly expansion on inspiration and belly relaxation on expiration. Do this lying supine initially (gravity assists), then progress to seated, then standing. The autonomic baseline shifts toward diaphragmatic dominance after 2-4 weeks of consistent practice.
Slow Breathing at 6 Breaths Per Minute
Slow breathing at approximately 6 breaths per minute (10-second cycle: roughly 4 seconds in, 6 seconds out) has been extensively studied in the heart-rate-variability biofeedback literature. The mechanism is that 6 breaths per minute (0.1 Hz) is the resonant frequency of the human baroreflex loop — the time constant of arterial baroreceptor feedback to the brainstem cardiovascular center. Breathing at this frequency maximally amplifies the natural respiratory sinus arrhythmia (heart rate accelerates during inhale, decelerates during exhale), producing the largest possible heart-rate variability.
High HRV is associated with parasympathetic dominance, lower cortisol, lower blood pressure, improved mood, and improved cognitive performance. Lehrer and Gevirtz (Frontiers in Psychology 2014) reviewed the substantial literature on resonant-frequency breathing biofeedback. Russo et al. (Breathe 2017) summarized the broader physiological effects of slow breathing in healthy humans.
The practical protocol: 5-20 minutes per day of slow nasal diaphragmatic breathing at approximately 6 breaths per minute. A metronome or paced-breathing app helps maintain the rhythm. Done in the morning before stimulants, or in the evening before bed, the practice progressively shifts the autonomic baseline toward parasympathetic dominance and reduces the chronic sympathetic activation associated with chronic mouth breathing and chest-wall breathing.
Exercise with Nose-Only Breathing
One of the most effective ways to extend nasal breathing capacity and retrain the chemoreceptor threshold is to exercise with the mouth deliberately closed. Walking, easy jogging, cycling, and resistance training can all be done with nose-only breathing once the practitioner has built tolerance.
The protocol popularized by Patrick McKeown (The Oxygen Advantage) and by Brian Mackenzie (The Art of Breath):
- Start with low-intensity activity (walking) with mouth taped or consciously closed
- If air hunger becomes uncomfortable, slow down rather than open the mouth
- Build to 30-60 minutes of continuous nose-only walking
- Progress to easy jogging with nose-only breathing
- Build to higher intensities over weeks to months
The training adaptations include reduced minute ventilation at any given workload, increased CO2 tolerance (higher Control Pause), improved nasal patency from repeated airflow stimulation, and improved exercise economy. Athletic performance does not noticeably suffer in trained nose breathers, and there is anecdotal evidence (though limited controlled data) that nose-only training improves endurance performance via CO2-tolerance and Bohr-effect mechanisms.
This is also one of the most effective tongue-posture retrainers: maintaining a sealed lip during exercise requires correct tongue position, and the practice generalizes to the resting daytime pattern.
A Practical Daily Protocol
A consolidated daytime practice for someone interested in eventually replacing mouth taping with autonomic nasal default:
- On waking: measure Control Pause before any food, drink, or stimulant. Log the number.
- Morning (5-10 min): slow nasal diaphragmatic breathing at approximately 6 breaths per minute, lying or seated.
- Throughout the day: tongue-posture awareness checks every 30-60 minutes. Tongue on palate, lips sealed, teeth lightly together.
- During exercise: walk or jog 20-30 minutes with mouth closed. Build tolerance progressively.
- Conversations and screen work: consciously breathe through the nose between sentences. Notice and correct any drift to mouth breathing.
- Evening (5-10 min): repeat slow nasal diaphragmatic breathing as a wind-down before sleep.
- At sleep: mouth tape if desired and if no contraindications (see Cautions and Adaptation).
- Weekly: trend the Control Pause. Goal is steady increase of 1-2 seconds per week.
Patients who follow this protocol for 6-12 weeks frequently find that the nighttime tape becomes unnecessary — the body has shifted to nasal default and continues nasal breathing into sleep without external prompting. The tape was a temporary scaffold; the underlying retraining is the durable change.
Key Research Papers
- Bruton A, Lewith GT. The Buteyko breathing technique for asthma: a review Search PubMed
- Bowler SD, Green A, Mitchell CA. Buteyko breathing techniques in asthma: a blinded RCT (Medical Journal of Australia 1998) — Search PubMed
- Cooper S, Oborne J, et al. Effect of Buteyko and pranayama breathing in asthma Search PubMed
- McHugh P, Aitcheson F, Duncan B, Houghton F. Buteyko Breathing Technique for asthma Search PubMed
- Courtney R, Cohen M. Investigating the claims of Konstantin Buteyko Search PubMed
- Russo MA, Santarelli DM, O'Rourke D. The physiological effects of slow breathing in the healthy human (Breathe 2017) — Search PubMed
- Lehrer PM, Gevirtz R. Heart rate variability biofeedback: how and why does it work? — PMID 25101026
- Jerath R, et al. Self-regulation of breathing as a primary treatment for anxiety — PMID 25869930
- Brown RP, Gerbarg PL. Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression — PMID 15750381
- Camacho M, Certal V, Abdullatif J, Zaghi S, Ruoff CM, Capasso R, Kushida CA. Myofunctional therapy to treat OSA: a systematic review and meta-analysis (Sleep 2015) — PMID 25348130
- Guimarães KC, Drager LF, Genta PR, Marcondes BF, Lorenzi-Filho G. Effects of oropharyngeal exercises on moderate OSA Search PubMed
- Diaftari Iharbjornsdottir D, et al. Orofacial myofunctional therapy for sleep-disordered breathing PubMed: Myofunctional therapy SDB
Connections
- Mouth Taping (Main Hub)
- Benefits Deep Dive Hub
- Nasal Breathing Benefits
- Snoring and Sleep Apnea
- Cautions and Adaptation
- Breathwork
- Sleep Hygiene
- Asthma
- Anxiety Disorders
- Obstructive Sleep Apnea
- All Remedies