Nasal Breathing Benefits
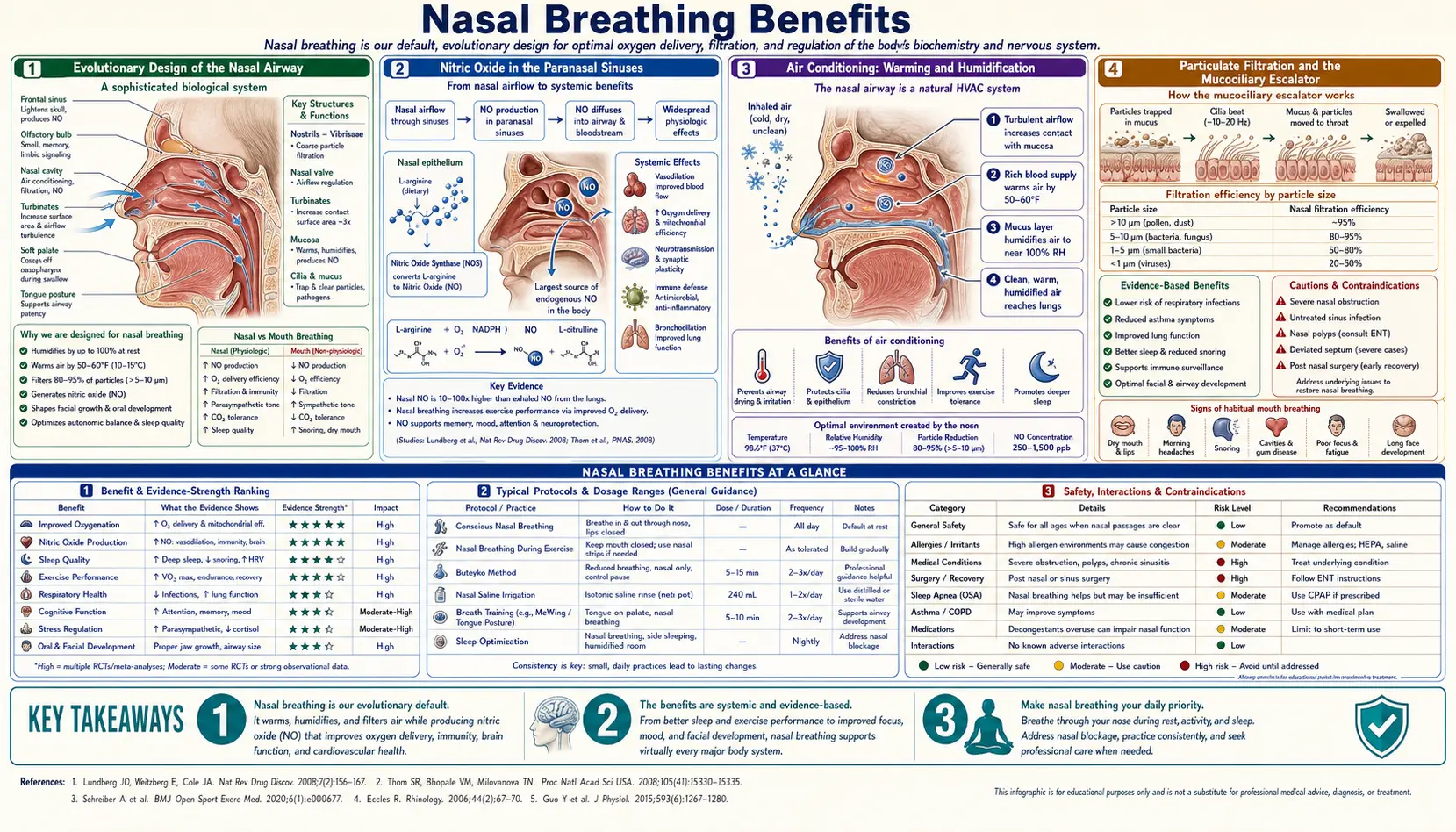
The nose is the body's designed primary airway, and the mouth is an emergency reserve channel. Every measurable parameter of gas exchange — humidification, warming, particulate filtration, nitric oxide delivery, expiratory resistance, carbon-dioxide tolerance, and even the timing of inspiration relative to the cardiac cycle — is optimized for nasal flow and degraded by oral flow. This deep dive walks through the eight major physiological functions of the nose during breathing, the experimental data that established each function, and the clinical consequences when habitual mouth breathing displaces nasal breathing as the dominant pattern.
Table of Contents
- Evolutionary Design of the Nasal Airway
- Nitric Oxide in the Paranasal Sinuses
- Air Conditioning: Warming and Humidification
- Particulate Filtration and the Mucociliary Escalator
- Expiratory Resistance and Functional Residual Capacity
- Carbon Dioxide Tolerance and the Bohr Effect
- Diaphragmatic Coupling and Vagal Tone
- The Nasal Cycle and Hemispheric Lateralization
- Consequences of Habitual Mouth Breathing
- Key Research Papers
- Connections
- Featured Videos
Evolutionary Design of the Nasal Airway
The human upper airway has two parallel channels: the nose, a narrow tortuous passage lined with specialized epithelium and richly vascularized turbinates, and the mouth, a wide unobstructed space designed for speech, mastication, and emergency airflow. The two channels merge in the oropharynx and continue together through the larynx and lower airway. This dual-channel arrangement is unusual among mammals — most obligate quadrupeds breathe almost exclusively through the nose, with the soft palate sealing off the mouth from the upper airway except during swallowing.
The shift to facultative oronasal breathing in humans is generally attributed to the evolution of speech, which requires open-mouth airflow modulated by the tongue, lips, and palate. The cost of that shift is that humans can default to mouth breathing during sleep, exercise, or nasal obstruction, with all of the physiological consequences enumerated below.
The nasal airway is not a simple tube. It contains three pairs of turbinates (inferior, middle, superior), the olfactory cleft, the openings of the paranasal sinuses, and a layer of pseudostratified ciliated columnar epithelium that produces approximately one liter of mucus per day. The cross-sectional area of the nasal valve — the narrowest point in the nose, located just behind the nostrils — is approximately 0.3-0.5 cm² per side. This small aperture is what generates the resistance that distinguishes nasal from oral breathing.
Nitric Oxide in the Paranasal Sinuses
The discovery that the paranasal sinuses continuously produce nitric oxide was published by Lundberg and colleagues in 1995 (Acta Physiologica Scandinavica) and remains one of the most consequential findings in upper-airway physiology. The maxillary sinuses produce the bulk of nasal NO, with smaller contributions from the ethmoid, frontal, and sphenoid sinuses. The concentration in the sinus cavities is in the parts-per-million range — orders of magnitude higher than the parts-per-billion levels found in exhaled lower-airway gas.
Nasal NO is inhaled with each nasal breath and exerts several documented effects in the lower airway:
- Bronchodilation. NO is a smooth-muscle relaxant; inhaled NO opens the small airways, modestly improving airflow.
- Pulmonary vasodilation. Inhaled NO selectively dilates pulmonary arterioles in ventilated alveoli, improving ventilation-perfusion matching. This is the basis for inhaled-NO therapy in persistent pulmonary hypertension of the newborn (iNO has been an FDA-approved drug since 1999).
- Antimicrobial activity. NO is a potent broad-spectrum antimicrobial that kills bacteria, viruses, and fungi via reactive nitrogen species. The sinus reservoir provides a continuous low-grade antimicrobial wash through the upper airway.
- Mucociliary stimulation. NO upregulates ciliary beat frequency in the airway epithelium, accelerating mucus clearance.
Mouth breathing bypasses the sinus NO reservoir entirely. The inspired air arrives at the lower airway without the bronchodilator, the vasodilator, or the antimicrobial wash. This is the single most consequential difference between nasal and oral breathing at the molecular level, and it is the mechanism most often cited in the popular literature on the topic.
A related observation: patients with cystic fibrosis and primary ciliary dyskinesia have characteristically low nasal NO, which has been developed as a screening test for PCD. Conversely, patients with chronic sinusitis often have variable nasal NO that reflects the inflammatory state of the mucosa.
Air Conditioning: Warming and Humidification
The nasal turbinates have an enormous surface area relative to their volume — on the order of 150 cm² per side — and are lined with a dense capillary plexus that delivers warm blood at body temperature directly under the mucosal surface. As inspired air flows over this surface, it picks up heat and water vapor by simple physical transfer.
The measured performance is striking. At an ambient temperature of 22°C and 30% relative humidity (typical indoor air), inspired air reaching the nasopharynx after one nasal breath is approximately 32°C and 80% relative humidity. By the time it reaches the carina (the branch point of the trachea into the two mainstem bronchi), it is essentially fully conditioned at 37°C and 100% relative humidity. This conditioning is critical because the lower airway epithelium dries out and ciliary function fails if inspired air arrives cold or dry.
The mouth provides almost no conditioning. Oral air enters the oropharynx essentially at ambient temperature and humidity. The lower airway then has to do all the conditioning itself, with two negative consequences:
- Mucosal water loss. The lower-airway mucosa loses water to warm and humidify the dry inspired air, contributing to bronchial irritation, cough, and the well-described phenomenon of nocturnal mouth-breathing dry throat.
- Cold-induced bronchoconstriction. Cold air in the lower airway is a known trigger for exercise-induced bronchoconstriction in susceptible individuals. This is why winter outdoor exercise frequently provokes asthma symptoms in mouth breathers but rarely in nose breathers — the nasal conditioning eliminates the trigger.
Particulate Filtration and the Mucociliary Escalator
The nose is the body's primary air-filtration system. Three sequential mechanisms remove particulate matter from inspired air:
- Vibrissae (nasal hair). The coarse hairs at the entrance of each nostril trap large particles (greater than approximately 10 microns) by simple mechanical impaction.
- Mucus trapping. The mucus layer covering the entire nasal epithelium traps smaller particles (1-10 microns) by adhesion. The mucus contains lysozyme, lactoferrin, defensins, and secretory IgA, providing chemical as well as mechanical defense.
- Mucociliary escalator. The cilia beat in a coordinated wave at approximately 10-12 Hz, sweeping the mucus layer (and trapped particles) backward toward the nasopharynx, where it is swallowed and inactivated by gastric acid. Total nasal clearance time is approximately 10-20 minutes.
Mouth breathing bypasses all three filtration mechanisms. Particulate matter, allergens, viruses, and bacteria reach the lower airway directly. In urban environments with high particulate pollution (PM2.5, PM10), this represents a measurable increase in deposited particle dose to the lower lungs. For individuals with chronic exposure to occupational dusts, pollens, or air pollution, switching from mouth to nasal breathing materially reduces the airborne challenge to the lower airway.
Expiratory Resistance and Functional Residual Capacity
The nasal airway has approximately twice the airflow resistance of the open mouth at any given flow rate. This resistance is present on both inspiration and expiration. The expiratory component is functionally important: it creates a small back-pressure of approximately 2-4 cmH2O at end-expiration that helps maintain alveolar recruitment and functional residual capacity (FRC).
The mechanism is conceptually similar to (but much milder than) two well-known clinical interventions:
- Pursed-lip breathing in COPD. Patients with emphysema use pursed-lip breathing to create expiratory back-pressure that prevents collapse of the floppy small airways. Nasal expiration provides a similar (much smaller) effect.
- Low-level PEEP in mechanical ventilation. Intubated patients receive 3-5 cmH2O of positive end-expiratory pressure to prevent atelectasis. Nasal expiration provides a roughly comparable physiological back-pressure.
The clinical translation is that mouth breathers tend toward slightly lower FRC and slightly greater alveolar derecruitment than nose breathers, particularly during sleep when respiratory drive is reduced. This may contribute to the observation that mouth breathers have somewhat lower nocturnal oxygen saturation even in the absence of formal sleep apnea.
Carbon Dioxide Tolerance and the Bohr Effect
Mouth breathing is associated, on average, with chronic mild hyperventilation — the tidal volume tends to be slightly larger and the respiratory rate slightly higher than during nasal breathing. The cumulative effect is a slightly lower arterial PaCO2 (chronic hypocapnia) and a slightly higher pH (chronic respiratory alkalosis at the subclinical level).
The Buteyko method, developed by the Soviet physiologist Konstantin Buteyko in the 1950s, is built on the observation that chronic hyperventilation is associated with a wide range of symptoms (bronchoconstriction, vasoconstriction, panic-anxiety, sleep disturbance) via the Bohr effect:
- Bohr effect. Hemoglobin's affinity for oxygen is modulated by the local PaCO2. Higher CO2 (lower pH) decreases hemoglobin's oxygen affinity, releasing more oxygen to peripheral tissues. Conversely, hypocapnia from hyperventilation increases hemoglobin's oxygen affinity, so less oxygen is released to tissues despite high oxygen saturation. The paradox is that hyperventilation reduces peripheral oxygen delivery.
- CO2 as vasodilator. CO2 is a potent cerebral vasodilator. Hypocapnia from hyperventilation produces cerebral vasoconstriction, which can manifest as lightheadedness, brain fog, or in extreme cases syncope. This is the mechanism behind the classic paper-bag treatment of acute hyperventilation.
- CO2 and smooth muscle. CO2 relaxes airway and vascular smooth muscle generally. Chronic hypocapnia is associated with increased bronchial reactivity and is a documented contributor to asthma in some patients.
Nasal breathing, by virtue of its higher resistance, tends to produce slower deeper breaths with normal or slightly elevated PaCO2, restoring the Bohr-effect dynamics to baseline. The Daytime Breathing Habits deep dive walks through the Buteyko Control Pause measurement that is used to assess and track this.
Diaphragmatic Coupling and Vagal Tone
Nasal breathing is preferentially coupled with diaphragmatic (abdominal) movement, while mouth breathing tends to recruit accessory muscles of the chest and neck. The reason appears to be partly mechanical (the higher inspiratory resistance of the nose requires a more efficient pump, which is the diaphragm) and partly neurological (nasal afferent input modulates the brainstem respiratory pattern generator).
Diaphragmatic breathing increases vagal tone via several mechanisms:
- Slow deep inspiration stimulates pulmonary stretch receptors, which signal via the vagus nerve to inhibit the sympathetic nervous system.
- Diaphragmatic descent during inspiration applies gentle mechanical pressure on the abdominal viscera and the abdominal vagal trunk, which has been proposed as a mechanical vagal-stimulation mechanism.
- Slow nasal breathing at approximately 6 breaths per minute resonates with baroreflex frequency, maximizing heart-rate variability and producing the well-documented relaxation response.
The practical consequence is that nasal diaphragmatic breathing is associated with parasympathetic dominance (rest-and-digest), while chest-wall mouth breathing is associated with sympathetic dominance (fight-or-flight). Most patients who switch from chronic mouth breathing to obligate nasal breathing report a generalized reduction in baseline anxiety within several weeks, consistent with this vagal-tone mechanism.
The Nasal Cycle and Hemispheric Lateralization
The nasal turbinates exhibit a slow physiological cycle of alternating congestion and decongestion: one side is dominant for approximately 90-180 minutes, then the other side takes over. This nasal cycle was first described by Kayser in 1895 and is now well-documented in rhinomanometry studies. The mechanism involves alternating sympathetic vasoconstrictor tone to the venous sinusoids of the inferior turbinate.
A separate (and more speculative) line of research, summarized in work by David Shannahoff-Khalsa and others, has proposed that the nasal cycle is linked to a contralateral cerebral hemisphere activation cycle — left-nostril dominance correlating with right-hemisphere activity and vice versa. The autonomic correlate is that right-nostril breathing is associated with sympathetic activation and left-nostril breathing with parasympathetic activation. Yogic pranayama practices (Nadi Shodhana, alternate-nostril breathing) explicitly manipulate this asymmetry.
The clinical relevance for mouth taping is that obligate nasal breathing preserves the natural nasal cycle, while mouth breathing bypasses it entirely. The reported subjective alertness benefit of nasal breathing during the day may relate in part to the maintenance of this autonomic cycling.
Consequences of Habitual Mouth Breathing
The negative consequences of chronic mouth breathing have been documented across multiple medical specialties:
- Orthodontic and craniofacial. Habitual mouth breathing in childhood is associated with the "long face syndrome" (anterior open bite, high-arched palate, retrognathic mandible, narrow maxilla). The mechanism is altered tongue posture: the tongue drops away from the palate, removing the gentle outward pressure that normally shapes maxillary growth. Harari et al. (American Journal of Orthodontics 2010) and Lin et al. quantified the effect in a meta-analysis.
- Dental. Mouth breathing dries out the oral cavity, reducing saliva production. Saliva contains buffers that neutralize acidic byproducts of oral bacteria and remineralization agents (calcium, phosphate). Mouth breathers have measurably higher rates of dental caries, gingivitis, and periodontal disease.
- Oral microbiome. Choi et al. (Sleep and Breathing 2015) measured intraoral pH and temperature during sleep with and without mouth breathing and found significant shifts in the microbial community structure. The implications for the oral microbiome and downstream systemic effects are an active area of research.
- Halitosis. The combination of dry mouth and altered microbial community is the most common cause of chronic morning halitosis.
- Sleep quality. Mouth breathers have higher rates of snoring, sleep fragmentation, and self-reported daytime sleepiness even in the absence of frank OSA.
- Cognitive and behavioral (in children). Bonuck et al. (Pediatrics 2012) demonstrated that sleep-disordered breathing (including habitual mouth breathing) at age 2.5 was associated with measurable neurobehavioral deficits at age 4 and 7.
For all of these reasons, the goal of mouth taping is not the tape itself — it is the restoration of obligate nasal breathing as the default pattern during sleep, with the tape acting as a behavioral training tool that becomes unnecessary once the new pattern is established.
Key Research Papers
- Lundberg JO, Weitzberg E, et al. Nitric oxide in exhaled air, paranasal sinus origin (Acta Physiol Scand 1995) — Search PubMed
- Lundberg JO. Nitric oxide and the paranasal sinuses (Anatomical Record 2008) — PMID 18951492
- Niinimaa V, Cole P, Mintz S, Shephard RJ. The switching point from nasal to oronasal breathing Search PubMed
- Cole P. Nasal and oral airflow resistances PubMed: Cole nasal/oral resistance
- Harari D, Redlich M, et al. The effect of mouth breathing versus nasal breathing on dentofacial development (American Journal of Orthodontics 2010) — Search PubMed
- Choi JE, Waddell JN, Lyons KM, Kieser JA. Intraoral pH and temperature during sleep with and without mouth breathing Search PubMed
- Lin L, Zhao T, Qin D, Hua F, He H. The impact of mouth breathing on dentofacial development PubMed: Mouth breathing meta-analysis
- Russo MA, Santarelli DM, O'Rourke D. The physiological effects of slow breathing in the healthy human Search PubMed
- Settipane RA. Nasal-pulmonary interactions PubMed: Nasal-pulmonary interactions
- Scadding G. Nitric oxide in the airways Search PubMed
- Lundberg JO. Airborne nitric oxide: inflammatory marker and aerocrine messenger Search PubMed
- Surda P, Putala M, et al. Mouth breathing and dryness in the upper respiratory tract PubMed: Surda mouth breathing
Connections
- Mouth Taping (Main Hub)
- Benefits Deep Dive Hub
- Snoring and Sleep Apnea
- Daytime Breathing Habits
- Cautions and Adaptation
- Breathwork
- Sleep Hygiene
- Oral Microbiome
- Obstructive Sleep Apnea
- Sinusitis
- All Remedies