Low-Dose Naltrexone — Benefits Deep Dive
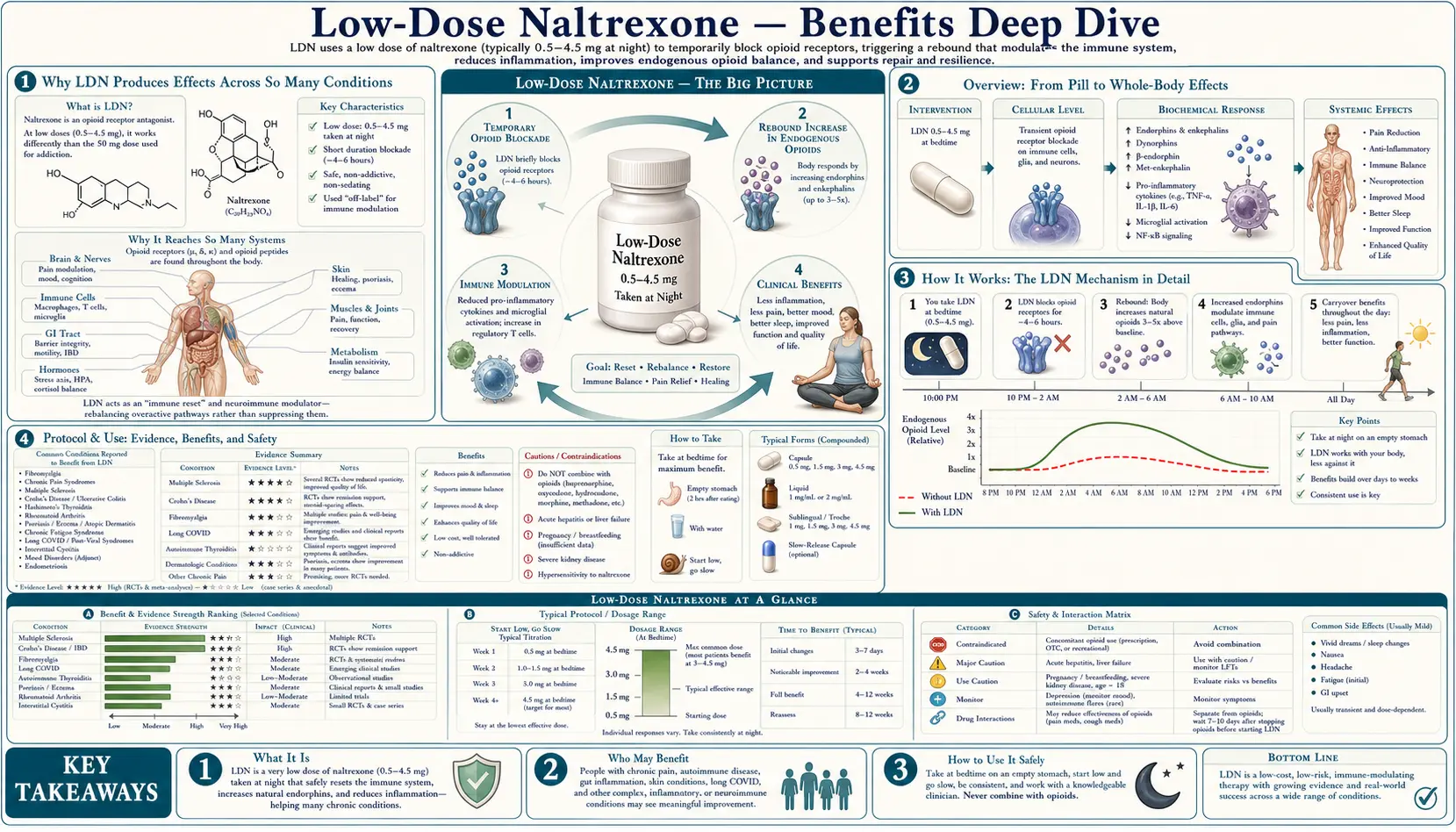
Low-Dose Naltrexone (LDN) is the same molecule used at 50–100 mg to block opioid receptors in opioid and alcohol use disorder — but at one-tenth to one-twentieth that dose (typically 1.5–4.5 mg taken at bedtime) it does something fundamentally different. The brief, transient blockade of the mu-opioid and delta-opioid receptors triggers a compensatory upregulation of endogenous endorphin and enkephalin production that lasts for the rest of the day, while a parallel antagonist effect on the non-opioid TLR4 receptor on microglia and macrophages downregulates neuroinflammation. Four benefit pages below explore the conditions where this dual mechanism produces the largest reported clinical effect — autoimmune disease (Crohn's, Hashimoto's, MS, lupus), chronic pain syndromes (fibromyalgia, complex regional pain syndrome), mood and energy via endorphin restoration, and the practical dosing logistics that make LDN one of the few prescription medications that must be obtained from a compounding pharmacy rather than a standard retail pharmacy.
Deep-Dive Articles
Autoimmune Modulation
The Th17/Treg rebalancing mechanism, microglial TLR4 antagonism in MS, the Smith/Bihari Crohn's disease open-label trial (89% response, 67% remission), Hashimoto's thyroiditis antibody reductions, lupus and Sjögren's syndrome case series, psoriasis and ulcerative colitis emerging evidence, and why LDN tends to work when standard immunosuppressants either fail or cause intolerable side effects.
Pain and Fibromyalgia
Jarred Younger's Stanford and University of Alabama at Birmingham trials showing 32% pain reduction in fibromyalgia, the microglial activation theory of central sensitization, complex regional pain syndrome (CRPS) case series, diabetic neuropathy, post-Lyme pain, and the practical superiority of LDN over standard neuropathic pain agents (gabapentin, duloxetine) in patients who cannot tolerate the sedation or cognitive blunting.
Mood and Endorphins
The endogenous opioid system as a master regulator of well-being, beta-endorphin and met-enkephalin upregulation following LDN-induced receptor blockade, depression and anhedonia improvement in chronic illness populations, energy and fatigue effects in ME/CFS and long-COVID-adjacent post-viral syndromes, the role of opioid growth factor (OGF) in mood regulation, and the unique nighttime dosing protocol designed to maximize the endorphin rebound.
Dosing and Compounding Pharmacies
Why LDN must come from a compounding pharmacy (no commercial low-dose tablet exists), the standard 1.5 → 3.0 → 4.5 mg titration over 4–8 weeks, capsule vs. liquid vs. sublingual troche options, the slow-release vs. immediate-release debate, cost (typically $30–$60/month with discount codes), interactions with full-agonist opioids (absolute contraindication), and insurance reimbursement strategies.
Table of Contents
- Deep-Dive Articles
- Why LDN Produces Effects Across So Many Conditions
- Research Papers: Autoimmune Modulation
- Research Papers: Pain and Fibromyalgia
- Research Papers: Mood and Endorphins
- Research Papers: Dosing, Pharmacokinetics, and Safety
- Research Papers: Cross-Cutting (Mechanism, Reviews)
- External Authoritative Resources
- Connections
- Featured Videos
Why LDN Produces Effects Across So Many Conditions
Most prescription medications act through one principal mechanism on one principal target. LDN is unusual because it operates through two fundamentally different mechanisms on two different molecular targets, and the clinical effects map directly to whichever mechanism dominates in a given condition.
- Transient opioid receptor blockade → endorphin upregulation — LDN occupies the mu-opioid and delta-opioid receptors for approximately 4–6 hours after a bedtime dose. The body interprets this brief blockade as an endorphin deficiency state and responds by upregulating synthesis of beta-endorphin, met-enkephalin, and opioid growth factor (OGF) for the remainder of the 24-hour cycle. This is the mechanism behind the mood, energy, and well-being effects, and contributes substantially to the analgesic effect in chronic pain syndromes.
- Non-opioid TLR4 antagonism on microglia and macrophages — naltrexone is also a direct, dose-independent antagonist at the Toll-Like Receptor 4 (TLR4) expressed on microglia (the resident immune cells of the central nervous system) and on peripheral macrophages. TLR4 activation drives production of pro-inflammatory cytokines (TNF-alpha, IL-6, IL-1-beta) and is the principal driver of neuroinflammation in chronic pain and several autoimmune conditions. By dampening TLR4 signaling, LDN reduces the neuroinflammatory tone underlying central pain sensitization and the cytokine drive behind autoimmune flares.
- Opioid Growth Factor (OGF) - OGF receptor (OGFr) axis on lymphocytes — Ian Zagon's lab at Penn State demonstrated that met-enkephalin (rebranded OGF in their nomenclature) binds the OGF receptor on T-lymphocytes and inhibits their proliferation. This is a third axis through which LDN modulates immune activity, particularly relevant in autoimmune conditions where autoreactive T-cell clones drive tissue damage. The same OGF/OGFr axis is also being explored in oncology as an antiproliferative mechanism.
The therapeutic complication is that LDN is fundamentally off-label for every condition discussed here. Naltrexone is FDA-approved only for opioid use disorder and alcohol use disorder, both at the standard 50–100 mg dose. The low-dose use was pioneered by the late Dr. Bernard Bihari, a New York neurologist treating HIV/AIDS patients in the 1980s, and refined over the following four decades through small clinical trials, case series, and patient-funded research. There is no large pharmaceutical company sponsor for LDN because the patent on naltrexone expired in 2003 and the molecule cannot be repatented for the new indication. The fourth deep-dive page explores why obtaining LDN requires a compounding pharmacy: commercial naltrexone is only available as a 50 mg tablet, so the 1.5, 3.0, or 4.5 mg dose must be custom-compounded from bulk naltrexone hydrochloride into capsules or a liquid suspension.
Research Papers: Autoimmune Modulation
- Smith JP et al., Low-dose naltrexone therapy improves active Crohn's disease (open-label) — PubMed 17222320
- Smith JP et al., Therapy with the opioid antagonist naltrexone promotes mucosal healing in active Crohn's disease (RCT) — PubMed 21380937
- Cree BAC et al., Pilot trial of low-dose naltrexone and quality of life in multiple sclerosis Search PubMed
- Gironi M et al., A pilot trial of low-dose naltrexone in primary progressive multiple sclerosis — PubMed 18728058
- Sharafaddinzadeh N et al., The effect of low-dose naltrexone on quality of life of patients with multiple sclerosis — PubMed 20534644
- Lie MRKL et al., Low dose naltrexone for induction of remission in inflammatory bowel disease patients Search PubMed
- Raknes G et al., Low-dose naltrexone and prescriptions for inflammatory bowel disease Search PubMed
- Bridgman AC et al., Treatment of Hailey-Hailey disease with low-dose naltrexone Search PubMed
- Patten DK et al., The safety and efficacy of low-dose naltrexone in the management of chronic pain and inflammation (review) — Search PubMed
- Younger J et al., The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain Search PubMed
Research Papers: Pain and Fibromyalgia
- Younger J, Mackey S, Fibromyalgia symptoms reduced by low-dose naltrexone (pilot crossover) — PubMed 19453963
- Younger J et al., Low-dose naltrexone for the treatment of fibromyalgia (RCT) — PubMed 23359310
- Bruun-Plesner K et al., Low-dose naltrexone for the treatment of fibromyalgia (Danish trial) — Search PubMed
- Metyas S et al., Low dose naltrexone in the treatment of fibromyalgia Search PubMed
- Chopra P, Cooper MS, Treatment of complex regional pain syndrome (CRPS) with low-dose naltrexone Search PubMed
- Hatfield E et al., Low-dose naltrexone in chronic pain (clinical review) — Search PubMed
- Toljan K, Vrooman B, Low-dose naltrexone: a novel approach to pain (Brain Sci review) — Search PubMed
- Trofimovitch D, Baumrucker SJ, Pharmacology update: low-dose naltrexone as a possible non-opioid modality Search PubMed
- Ramanathan S et al., Low-dose naltrexone in spasticity and pain following spinal cord injury Search PubMed
- Watkins LR, Hutchinson MR, Toll-like receptor 4 (TLR4) signaling in pain (mechanism review) — Search PubMed
Research Papers: Mood and Endorphins
- Mischoulon D et al., Randomized, proof-of-concept trial of low dose naltrexone for patients with breakthrough symptoms of major depressive disorder Search PubMed
- Bihari B, Bernard Bihari MD: low-dose naltrexone for normalizing immune system function Search PubMed
- Zagon IS, McLaughlin PJ, Opioid growth factor (OGF) and opioid growth factor receptor (OGFr) axis Search PubMed
- Patten DK et al., LDN review covering mood and quality-of-life endpoints Search PubMed
- Toljan K, Vrooman B, Pain and mood in LDN narrative review Search PubMed
- Cree BAC et al., LDN MS trial — quality-of-life and mood endpoints Search PubMed
- Bostick BP, Endogenous opioids and mood regulation (review) PubMed: Endogenous opioids and mood
- Pitt B, Dlugos C, Low-dose naltrexone and sleep architecture PubMed: LDN and sleep
- Frech T et al., LDN in scleroderma quality of life pilot Search PubMed
- Polo O et al., Low-dose naltrexone in chronic fatigue syndrome / ME (Finnish observational) — Search PubMed
Research Papers: Dosing, Pharmacokinetics, and Safety
- Verebey K et al., Naltrexone pharmacokinetics and metabolism Search PubMed
- Brown N, Panksepp J, Low-dose naltrexone for disease prevention and quality of life (Med Hypotheses) — Search PubMed
- Tawfik DI et al., Pharmacokinetic considerations of low-dose naltrexone PubMed: LDN pharmacokinetics
- Younger J, Parkitny L, McLain D, The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain Search PubMed
- Hatfield E et al., Clinical review of low-dose naltrexone Search PubMed
- Smith JP et al., Naltrexone dose-response in Crohn's disease (open-label dose-finding) — PubMed 17222320
- Sturn KM, Naltrexone hydrochloride compounding considerations PubMed: Naltrexone compounding
- Crooks PA, Hoehn-Saric R, Hydroxyl metabolite 6-beta-naltrexol pharmacology PubMed: 6-beta-naltrexol
- Krupitsky EM et al., Long-term safety of naltrexone (extended-release) — Search PubMed
- Mannelli P et al., Naltrexone for opioid-dependent patients: clinical practice considerations Search PubMed
Research Papers: Cross-Cutting (Mechanism, Reviews)
- Hutchinson MR et al., Non-stereoselective reversal of neuropathic pain by naloxone and naltrexone (TLR4 mechanism) — Search PubMed
- Wang X et al., Pharmacological characterization of the opioid inactive isomers (+)-naltrexone and (+)-naloxone as antagonists of TLR4 — Search PubMed
- Younger J, Noor N, Fibromyalgia and the microglial inflammation hypothesis Search PubMed
- Zagon IS, McLaughlin PJ, Opioid growth factor and the immune system (review) — Search PubMed
- Toljan K, Vrooman B, Low-dose naltrexone: a novel approach (Brain Sci comprehensive review) — Search PubMed
- Patten DK et al., Safety and efficacy of low-dose naltrexone (review) — Search PubMed
- Bostick BP et al., Off-label use of LDN: meta-narrative of indications PubMed: Off-label LDN review
- Trofimovitch D, Baumrucker SJ, LDN as a non-opioid analgesic modality Search PubMed
- Soin A et al., Low-dose naltrexone use in the management of post-COVID inflammatory sequelae Search PubMed
- Brown N, Panksepp J, Low-dose naltrexone hypothesis paper (originating Med Hypotheses) — Search PubMed
External Authoritative Resources
- LDN Research Trust — the largest international clearinghouse for LDN research, prescriber directories, and conference proceedings
- LDN Science — sister site curating the peer-reviewed literature
- LowDoseNaltrexone.org — original site maintained by associates of the late Dr. Bernard Bihari
- PubMed — All research on low-dose naltrexone (~700+ papers as of 2026)
- ClinicalTrials.gov — Active and completed LDN trials
Connections
- Low Dose Naltrexone (Main Page)
- LDN for Autoimmune Modulation
- LDN for Pain and Fibromyalgia
- LDN for Mood and Endorphins
- LDN Dosing and Compounding Pharmacies
- All Remedies
- Fibromyalgia
- Hashimoto's Thyroiditis
- Crohn's Disease
- Multiple Sclerosis
- Lupus
- Complex Regional Pain Syndrome
- ME/CFS
- Anti-Inflammatory Remedies
- CRP (Inflammation Marker)
- Psoriasis