Aspirin & The Kidneys — Nephrotoxicity, AKI, and Renal Risk
Aspirin (acetylsalicylic acid) is one of the most widely consumed drugs in the world, taken by tens of millions daily for cardiovascular protection, pain, fever, and inflammation. Its effects on the kidneys are paradoxical: short-term low-dose use is generally well tolerated in healthy adults, yet aspirin shares the same fundamental mechanism — cyclooxygenase (COX) inhibition — that makes other non-steroidal anti-inflammatory drugs (NSAIDs) a leading cause of drug-induced acute kidney injury. This page summarizes the renal physiology, the documented nephrotoxic risks, and the practical situations in which aspirin can compromise kidney function.
Table of Contents
- Introduction: Why Kidneys Care About COX Inhibition
- Renal Physiology of Prostaglandins
- Acute Kidney Injury (AKI) from Aspirin and NSAIDs
- Analgesic Nephropathy & Papillary Necrosis
- The "Triple Whammy": NSAID + ACEi/ARB + Diuretic
- Aspirin in Chronic Kidney Disease (CKD)
- Low-Dose Aspirin (81 mg) — Does It Carry Less Risk?
- Aspirin in Dialysis Patients
- Pediatric Considerations & Reye's Syndrome
- Practical Guidance: Avoidance, Monitoring, Hydration
- References & Research Papers
- Connections
- Featured Videos
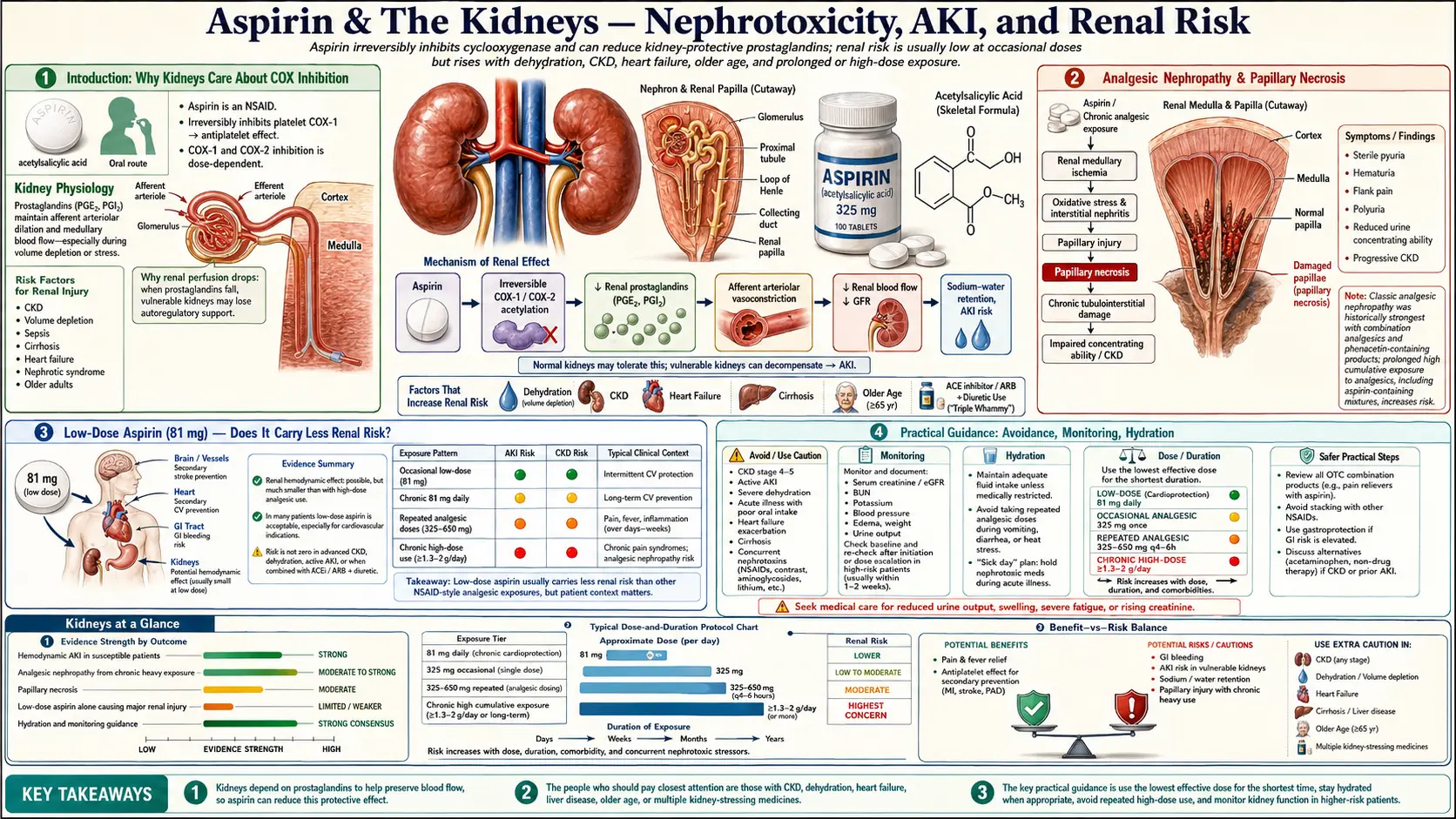
Introduction: Why Kidneys Care About COX Inhibition
Aspirin works by irreversibly acetylating cyclooxygenase enzymes (COX-1 and COX-2), blocking the conversion of arachidonic acid to prostaglandins and thromboxane. In platelets this produces the antithrombotic effect that underlies aspirin's cardiovascular benefit. In the kidneys, however, the same enzymes produce vasodilatory prostaglandins — chiefly prostaglandin E2 (PGE2) and prostacyclin (PGI2) — that maintain renal blood flow and glomerular filtration rate (GFR) under stress.
Under normal conditions, when a person is well-hydrated and has healthy kidneys, prostaglandins play only a minor role in regulating renal hemodynamics. But under conditions of effective volume depletion — dehydration, heart failure, cirrhosis, sepsis, hemorrhage, advanced age, or pre-existing CKD — circulating angiotensin II, norepinephrine, and vasopressin levels rise sharply and would constrict the renal vasculature. Prostaglandins counteract this by dilating the afferent arteriole and preserving glomerular perfusion. Inhibit COX with aspirin or another NSAID at this moment and the protective vasodilation disappears, GFR drops abruptly, and ischemic acute kidney injury can follow within hours to days.
Renal Physiology of Prostaglandins
The kidney expresses both COX-1 (constitutive in the medulla, vasculature, and glomerulus) and COX-2 (constitutive in the macula densa and medullary interstitial cells, induced by salt depletion and volume contraction). The renal prostaglandins they generate have several essential functions:
1. Afferent Arteriole Vasodilation
- PGE2 and PGI2 dilate the afferent arteriole, increasing blood flow into the glomerulus and supporting GFR
- This effect becomes critical when systemic vasoconstrictors (angiotensin II, catecholamines) are elevated — without prostaglandin counter-regulation, the afferent arteriole would constrict and renal perfusion would collapse
- Aspirin and other COX inhibitors abolish this protective vasodilation, leaving the kidney exposed to unopposed vasoconstriction
2. Sodium and Water Handling
- Medullary prostaglandins inhibit sodium reabsorption in the thick ascending limb of the loop of Henle
- They antagonize the antidiuretic action of vasopressin in the collecting duct
- NSAID-induced prostaglandin loss therefore promotes sodium and water retention — a common mechanism of NSAID-related edema, weight gain, and worsening of heart failure or hypertension
3. Renin Release
- COX-2-derived prostaglandins at the macula densa stimulate renin secretion from the juxtaglomerular apparatus
- Chronic NSAID use can blunt renin release, occasionally causing hyporeninemic hypoaldosteronism with hyperkalemia — a recognized cause of NSAID-induced potassium retention
4. Patient Populations Most Dependent on Renal Prostaglandins
- Adults over age 65 (declining nephron mass and baseline GFR)
- Heart failure (reduced effective arterial volume, high circulating angiotensin II)
- Cirrhosis with ascites (hepatorenal physiology, splanchnic vasodilation)
- Pre-existing CKD of any cause
- Volume depletion: vomiting, diarrhea, diuretic therapy, hot-weather dehydration, surgical NPO status
- Sepsis or hypotension
- Concurrent use of ACE inhibitors, ARBs, or calcineurin inhibitors
Acute Kidney Injury (AKI) from Aspirin and NSAIDs
Drug-induced AKI accounts for roughly 20% of all hospital-acquired AKI cases, and NSAIDs — including aspirin at higher analgesic and anti-inflammatory doses — are consistently among the most frequently implicated agents. Several distinct patterns of NSAID-related kidney injury are recognized:
Hemodynamic (Pre-Renal) AKI
- The most common NSAID-induced renal syndrome
- Mechanism: loss of prostaglandin-mediated afferent arteriole vasodilation, reduced glomerular perfusion, fall in GFR
- Onset: hours to days after exposure, especially in volume-depleted or hemodynamically vulnerable patients
- Typically reversible if the drug is stopped early and volume is restored
- Bland urinalysis (no significant proteinuria, hematuria, or casts) is characteristic
Acute Interstitial Nephritis (AIN)
- An immune-mediated hypersensitivity reaction to the drug
- Onset typically weeks to months after starting the NSAID, but can occur with any agent
- Often presents with sterile pyuria, white-cell casts, eosinophiluria (variable), and sometimes the classic triad of fever, rash, and eosinophilia (less common with NSAIDs than with antibiotics)
- NSAID-induced AIN is uniquely associated with concurrent nephrotic-range proteinuria caused by minimal change disease — an unusual two-hit pattern
Acute Tubular Necrosis
- Severe or prolonged ischemia from sustained renal hypoperfusion can progress from reversible pre-renal physiology to overt tubular cell injury
- This is the mechanism by which NSAID exposure during sepsis, surgery, or contrast administration can produce a lasting drop in GFR
Reported Incidence
- Population-based cohort studies estimate that NSAID use roughly doubles the short-term risk of AKI hospitalization in older adults compared with non-users
- The absolute risk in healthy adults is small, but in patients over 65 with pre-existing CKD or heart failure the relative risk can rise three- to five-fold
- Risk is dose-dependent and rises sharply with higher anti-inflammatory dosing (≥ 1,200 mg/day of aspirin or equivalent NSAID load)
Analgesic Nephropathy & Papillary Necrosis
Analgesic nephropathy is a slowly progressive form of chronic kidney disease caused by the long-term, heavy use of combination analgesic preparations — classically those containing phenacetin, paracetamol (acetaminophen), aspirin, and caffeine in the same tablet. It was first described in Switzerland in the 1950s and became a major cause of end-stage renal disease in parts of Europe and Australia before phenacetin was withdrawn from the market in the 1970s and 1980s.
Pathology
- Renal papillary necrosis: ischemic and oxidative damage to the renal medullary papillae, which can slough into the urinary tract and cause obstruction or hematuria
- Chronic interstitial nephritis: tubulointerstitial inflammation, fibrosis, and tubular atrophy
- Bilateral, symmetric atrophy: shrunken kidneys with characteristic papillary calcifications visible on CT (the "garland sign")
Aspirin's Specific Role
- Phenacetin and its metabolite acetaminophen are now considered the principal nephrotoxic components of the historical combination analgesics
- Aspirin alone has weaker evidence as a sole cause of analgesic nephropathy, but it appears to potentiate phenacetin/acetaminophen toxicity by depleting glutathione and impairing medullary prostaglandin synthesis — the medulla relies on prostaglandins for its already marginal blood supply
- Heavy chronic users (often defined as a cumulative intake exceeding 2–3 kg over a lifetime, or daily use for many years) remain the population at risk
- Modern analgesic preparations no longer contain phenacetin, and the incidence of classical analgesic nephropathy has fallen sharply, but acetaminophen-NSAID combinations and chronic high-dose NSAID use can still produce a similar clinical picture
Risk of Urothelial Cancer
- Long-term phenacetin use is also associated with transitional cell carcinoma of the renal pelvis and ureter
- Whether aspirin alone shares this risk is uncertain; large cohort studies have not consistently shown an excess urothelial cancer risk from aspirin without phenacetin
The "Triple Whammy": NSAID + ACEi/ARB + Diuretic
The combination of an NSAID with both a renin-angiotensin system blocker (ACE inhibitor or angiotensin receptor blocker) and a diuretic is so consistently associated with AKI that it has been given a name in the nephrology and pharmacovigilance literature: the triple whammy. Each agent independently reduces a different compensatory mechanism the kidney relies on; together, they leave the glomerulus with no defense.
Why Each Component Matters
- Diuretic: contracts intravascular volume, raises circulating angiotensin II, and shifts the patient toward a prostaglandin-dependent state for maintenance of GFR
- ACEi or ARB: blocks angiotensin II's vasoconstriction of the efferent arteriole, lowering glomerular hydrostatic pressure
- NSAID (or aspirin at anti-inflammatory dose): blocks prostaglandin-mediated afferent arteriole vasodilation, lowering glomerular blood flow
- Net effect: simultaneous loss of preglomerular dilation and postglomerular constriction in a volume-contracted patient — glomerular filtration pressure collapses
Documented Risk
- A landmark BMJ cohort study (Lapi et al., 2013) found that triple therapy was associated with roughly a 31% increased rate of AKI compared with double therapy (RAS blocker + diuretic) without an NSAID, with the highest risk in the first 30 days of triple therapy
- Subsequent population-based analyses have consistently confirmed the elevated AKI risk, especially in elderly patients
- The combination is considered a major preventable cause of community-acquired AKI
Clinical Implications
- Patients on chronic ACEi/ARB plus diuretic therapy — including the very common heart failure and hypertension regimens — should avoid or minimize NSAID use
- Cardioprotective low-dose aspirin (81 mg) carries far less hemodynamic risk than full-dose NSAIDs but is not entirely benign in this population, particularly during dehydrating illness
- Sick-day rules for older patients on RAS blockers and diuretics commonly recommend temporarily holding all three agents during vomiting, diarrhea, or febrile illness
Aspirin in Chronic Kidney Disease (CKD)
Patients with established CKD face a difficult balance: they are at high cardiovascular risk and could benefit from antiplatelet therapy, but they are also more vulnerable to drug-induced kidney injury and bleeding. The evidence base for aspirin in CKD is therefore nuanced.
Cardiovascular Risk in CKD
- CKD multiplies cardiovascular risk: a patient with eGFR 30–60 mL/min/1.73 m2 has roughly twice the cardiovascular event rate of a person with normal kidney function, and risk rises further with worsening eGFR
- Cardiovascular disease, not progression to dialysis, is the leading cause of death in CKD
- This makes secondary prevention with aspirin highly attractive in principle
Bleeding Risk in CKD
- CKD causes a uremic platelet dysfunction even before dialysis is needed, increasing baseline bleeding risk
- Adding aspirin compounds this and produces a documented increase in major bleeding, particularly gastrointestinal
- The KDIGO controversies conferences and major guideline bodies have stopped short of recommending routine primary-prevention aspirin in CKD because the bleeding cost may equal or exceed the cardiovascular benefit
Renal Risk of Aspirin in CKD
- Low-dose aspirin (75–100 mg) has not been clearly shown to accelerate CKD progression in well-conducted long-term studies
- Higher-dose aspirin and other NSAIDs have been linked to faster eGFR decline in observational cohorts
- For patients with established cardiovascular disease and CKD, secondary-prevention aspirin is generally still considered net beneficial; for primary prevention in CKD without prior events, the calculus is much closer and individualized
Low-Dose Aspirin (81 mg) — Does It Carry Less Renal Risk?
The 81 mg "baby aspirin" tablet provides enough irreversible platelet COX-1 inhibition to deliver the antithrombotic effect, while exerting only modest systemic COX inhibition. The renal risk profile is correspondingly different from that of full-dose aspirin or other NSAIDs.
Evidence Summary
- Large randomized trials of low-dose aspirin for cardiovascular prevention (including the Physicians' Health Study, the Women's Health Study, ASPREE, and ASCEND) have not shown a meaningful excess of clinically significant renal events compared with placebo
- Some observational data suggest a small absolute increase in AKI episodes among elderly low-dose aspirin users, particularly those who are also on diuretics or RAS blockers
- Long-term studies of analgesic exposure consistently identify higher cumulative aspirin doses (typically > 500 mg/day for years) as the threshold above which CKD risk rises measurably
- Low-dose aspirin still carries the "triple whammy" risk if combined with a diuretic and an ACEi or ARB during volume depletion
Bottom Line on 81 mg
- For most adults with normal kidney function and adequate hydration, 81 mg daily poses minimal direct renal risk
- The renal risk becomes meaningful when combined with other COX inhibitors (such as ibuprofen for pain), with RAS blockade, with diuretics, or with significant volume depletion
- The dominant adverse effect of low-dose aspirin remains gastrointestinal bleeding, not nephrotoxicity
Aspirin in Dialysis Patients
Patients on chronic hemodialysis or peritoneal dialysis represent a distinct population in which the trade-off between cardiovascular protection and bleeding is sharpest.
Cardiovascular Burden
- Cardiovascular mortality in dialysis patients is roughly 10–20 times higher than in the age-matched general population
- Sudden cardiac death, myocardial infarction, and stroke are the leading causes of death
Bleeding Burden
- Uremic platelet dysfunction is severe in dialysis-dependent patients
- Heparin exposure during hemodialysis sessions adds further bleeding risk
- Dialysis patients have notably higher rates of GI bleeding and intracranial hemorrhage than the general population
What the Evidence Shows
- Dialysis patients have been systematically excluded from most major aspirin cardiovascular outcome trials, so high-quality randomized data are sparse
- Observational studies and meta-analyses suggest that aspirin in dialysis patients does reduce major cardiovascular events but at the cost of an increase in major bleeding, with overall mortality benefit uncertain
- For dialysis patients with established coronary disease, aspirin is generally continued; for primary prevention, the decision is individualized and many nephrologists do not recommend it
- Aspirin does not directly worsen residual kidney function in anuric or near-anuric dialysis patients, since the hemodynamic mechanism that drives NSAID-induced AKI is no longer relevant once the kidneys have failed; the concern shifts entirely to bleeding
Pediatric Considerations & Reye's Syndrome
Aspirin is contraindicated in children and adolescents recovering from viral illnesses because of its association with Reye's syndrome — a rare but devastating disorder of acute hepatic failure and non-inflammatory encephalopathy. Although Reye's syndrome is fundamentally hepatic-cerebral rather than renal, it has metabolic features relevant to the broader question of aspirin pharmacology in children.
Pathophysiology
- Reye's syndrome involves diffuse mitochondrial injury, particularly in hepatocytes and neurons, with microvesicular hepatic steatosis, hyperammonemia, and cerebral edema
- Affected children typically have a preceding viral illness (classically influenza or varicella) and a history of aspirin or salicylate exposure
- The mitochondrial injury appears to involve impaired beta-oxidation of fatty acids and inhibition of oxidative phosphorylation
- Cytochrome P450 (CYP) enzymes contribute to salicylate metabolism, and immature pediatric CYP activity may produce reactive intermediates that worsen mitochondrial stress during viral illness
Renal Involvement
- Reye's syndrome itself can include renal tubular dysfunction with proximal tubular wasting of amino acids and phosphate
- Hypovolemia and hepatic failure can produce hepatorenal physiology and secondary AKI
- These renal manifestations are secondary to the systemic illness rather than direct aspirin nephrotoxicity
Practical Rule
- Aspirin should not be used in children or teenagers under 19 with viral illnesses, fever of unknown cause, or chickenpox
- Acetaminophen and ibuprofen are the standard pediatric antipyretics — though both also carry their own renal cautions, particularly in dehydrated febrile children
- The rare exceptions in which children are prescribed aspirin (Kawasaki disease, certain rheumatic and post-cardiac-surgery indications) are managed by pediatric specialists
Practical Guidance: Avoidance, Monitoring, Hydration
Patients Who Should Generally Avoid Aspirin (or Use With Specialist Input)
- Adults with eGFR < 30 mL/min/1.73 m2, except where cardiovascular indications outweigh bleeding risk
- Patients with active or recent gastrointestinal bleeding
- Patients with decompensated heart failure or cirrhosis with ascites
- Anyone with a history of NSAID-induced AKI, interstitial nephritis, or papillary necrosis
- Children and adolescents with viral illness (Reye's syndrome risk)
- Pregnant patients in the third trimester (NSAID and aspirin use can constrict the fetal ductus arteriosus and impair fetal renal function with oligohydramnios; low-dose aspirin used for preeclampsia prevention is given earlier in pregnancy under obstetric supervision)
Sick-Day Rules
- During acute vomiting, diarrhea, or febrile illness, temporarily hold any NSAID, ACE inhibitor or ARB, diuretic, SGLT2 inhibitor, and metformin until oral intake is restored
- Low-dose cardioprotective aspirin is sometimes continued at the prescriber's discretion, but the threshold for holding it lowers if dehydration is significant
- Resume medications once eating, drinking, and urine output have returned to normal
Monitoring
- For patients on chronic aspirin who develop new AKI risk factors, baseline serum creatinine and a follow-up measurement within 1–2 weeks of any change in regimen are reasonable
- In hospitalized patients receiving aspirin alongside other nephrotoxins or contrast, daily creatinine monitoring is standard
- Older patients on chronic NSAIDs of any kind should have annual eGFR and urine albumin assessments
Hydration and Concurrent Medications
- Adequate hydration is the single most important modifiable factor for reducing aspirin- and NSAID-related AKI
- Avoid stacking NSAIDs — do not combine cardioprotective aspirin with daily ibuprofen, naproxen, diclofenac, or topical diclofenac in large amounts
- If pain control is needed in a patient who must remain on aspirin, acetaminophen at appropriate doses is generally preferred from a renal-safety standpoint, with awareness of its hepatic considerations
- Coffee consumption has been associated with a modestly lower incidence of AKI in observational studies (Johns Hopkins ARIC analysis), and adequate caffeine-free fluid intake supports renal perfusion — but neither is a substitute for sound prescribing
References & Research Papers
Renal Prostaglandins & NSAID Mechanism
- Search PubMed
- Clive DM, Stoff JS. Renal syndromes associated with nonsteroidal antiinflammatory drugs. New England Journal of Medicine. 1984;310(9):563-572.
- Nasrallah R, Hassouneh R, Hébert RL. Chronic kidney disease: targeting prostaglandin E2 receptors. American Journal of Physiology — Renal Physiology. 2014;307(3):F243-F250.
NSAID-Induced AKI & Triple Whammy
- Lapi F, Azoulay L, Yin H, Nessim SJ, Suissa S. Concurrent use of diuretics, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers with non-steroidal anti-inflammatory drugs and risk of acute kidney injury: nested case-control study. BMJ. 2013;346:e8525.
- Search PubMed
- Schneider V, Levesque LE, Zhang B, Hutchinson T, Brophy JM. Association of selective and conventional nonsteroidal antiinflammatory drugs with acute renal failure: a population-based, nested case-control analysis. American Journal of Epidemiology. 2006;164(9):881-889.
- Nderitu P, Doos L, Jones PW, Davies SJ, Kadam UT. Non-steroidal anti-inflammatory drugs and chronic kidney disease progression: a systematic review. Family Practice. 2013;30(3):247-255.
Analgesic Nephropathy & Papillary Necrosis
- De Broe ME, Elseviers MM. Analgesic nephropathy. New England Journal of Medicine. 1998;338(7):446-452.
- Search PubMed
- Mihatsch MJ, Khanlari B, Brunner FP. Obituary to analgesic nephropathy — an autopsy study. Nephrology Dialysis Transplantation. 2006;21(11):3139-3145.
Aspirin in CKD & Cardiovascular Prevention
- McNeil JJ, Wolfe R, Woods RL, et al. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly (ASPREE). New England Journal of Medicine. 2018;379(16):1509-1518.
- ASCEND Study Collaborative Group. Effects of aspirin for primary prevention in persons with diabetes mellitus. New England Journal of Medicine. 2018;379(16):1529-1539.
- Palmer SC, Di Micco L, Razavian M, et al. Effects of antiplatelet therapy on mortality and cardiovascular and bleeding outcomes in persons with chronic kidney disease: a systematic review and meta-analysis. Annals of Internal Medicine. 2012;156(6):445-459.
- Jardine MJ, Ninomiya T, Perkovic V, et al. Aspirin is beneficial in hypertensive patients with chronic kidney disease: a post-hoc subgroup analysis of a randomized controlled trial. Journal of the American College of Cardiology. 2010;56(12):956-965.
Low-Dose Aspirin Renal Safety
Reye's Syndrome & Pediatric Aspirin
- Hurwitz ES, Barrett MJ, Bregman D, et al. Public Health Service study on Reye's syndrome and medications. Report of the pilot phase. New England Journal of Medicine. 1985;313(14):849-857.
- Belay ED, Bresee JS, Holman RC, Khan AS, Shahriari A, Schonberger LB. Reye's syndrome in the United States from 1981 through 1997. New England Journal of Medicine. 1999;340(18):1377-1382.
Connections
- Aspirin Overview
- Celery Juice and Kidney Disease
- Aspirin for Heart Attack Prevention
- Aspirin Health Benefits
- Aspirin Side Effects
- NAC (N-Acetylcysteine)
- Mercury
- Kidney Disease
- Acute Kidney Injury
- eGFR
- Kidney Function Tests
- Heart Failure
- Hypertension
- Aspirin and Cancer Prevention
- Aspirin for Stroke Prevention
- Creatinine
- Coffee
- Kidney Injury