Aspirin & Stroke Prevention
Aspirin (acetylsalicylic acid) occupies a uniquely double-edged position in stroke medicine. The same antiplatelet effect that reduces the risk of clot-driven ischemic stroke simultaneously increases the risk of bleeding — including hemorrhagic stroke. Understanding when aspirin helps, when it harms, and for whom the balance tips favorably is one of the most nuanced decisions in preventive cardiology and neurology. This article summarizes the landmark trial evidence across acute treatment, secondary prevention, and the increasingly cautious modern approach to primary prevention.
Table of Contents
- Introduction: The Two Faces of Stroke
- Mechanism: Irreversible COX-1 & TXA2 Blockade
- Acute Ischemic Stroke Treatment: IST & CAST
- Secondary Prevention After Stroke or TIA
- Primary Prevention: The Modern Picture
- Atrial Fibrillation: Why Aspirin Is Now Inadequate
- USPSTF 2022 Recommendation
- Hemorrhagic Stroke Risk Quantified
- Aspirin + Clopidogrel (DAPT) Duration
- Special Populations: Diabetes, Women, Elderly
- Practical Dosing & Acute Caveats
- References
- Connections
- Featured Videos
Introduction: The Two Faces of Stroke
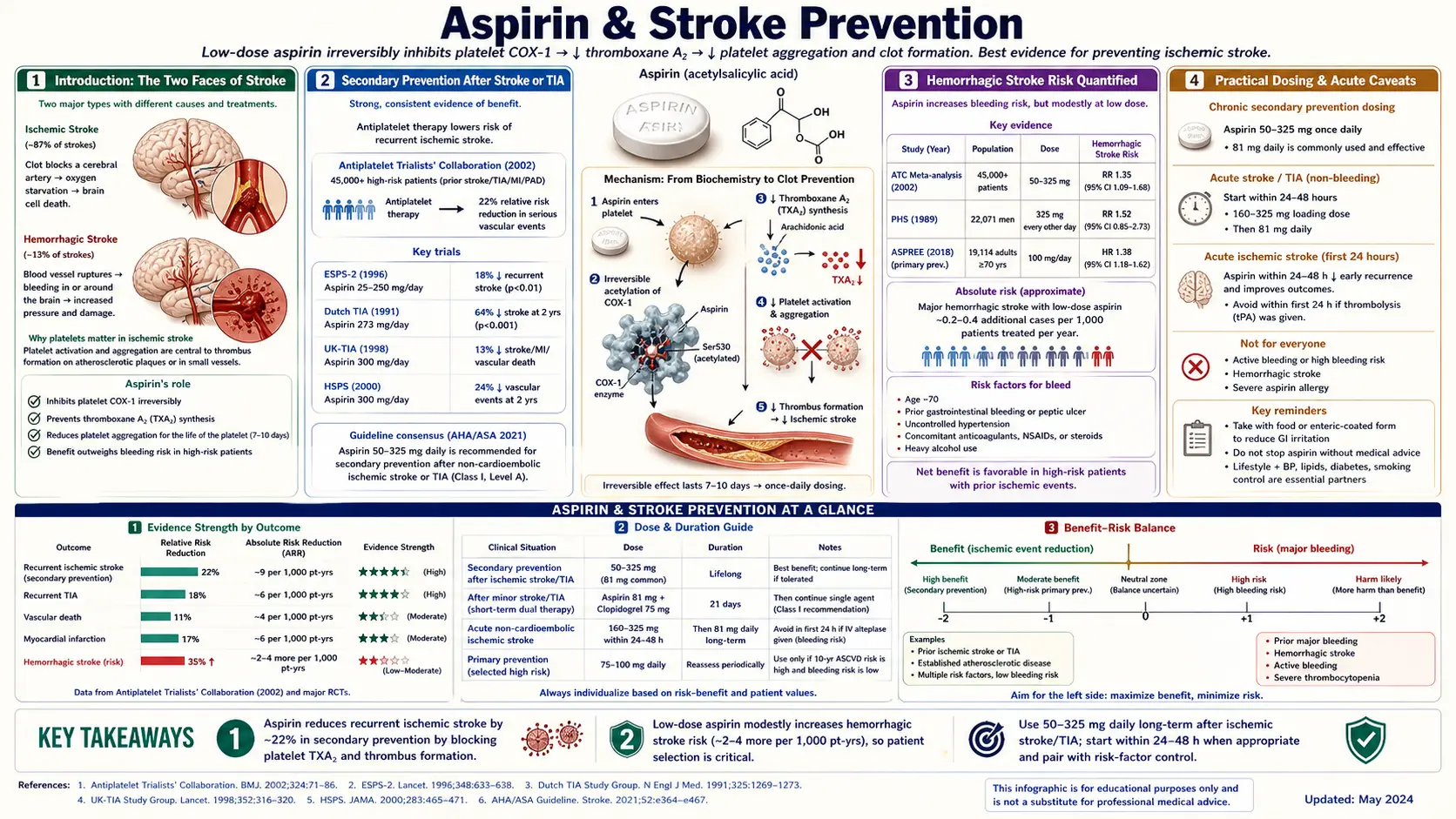
Stroke is not a single disease. Roughly 87% of strokes are ischemic — caused by a clot blocking a cerebral artery — while the remaining 13% are hemorrhagic, caused by rupture of a blood vessel and bleeding into or around the brain (intracerebral or subarachnoid hemorrhage). Aspirin's antiplatelet action opposes clot formation, which is why it can prevent and treat ischemic stroke. But that same effect impairs the platelet plug that seals a ruptured vessel, which is why aspirin can precipitate or worsen hemorrhagic stroke.
Because the clinical presentation of ischemic and hemorrhagic stroke can be identical at the bedside — both produce sudden focal neurological deficits — the treatment implications are enormous. Giving aspirin blindly to a patient with undiagnosed intracerebral hemorrhage can be catastrophic. This is why acute stroke protocols universally require brain imaging (non-contrast CT) to rule out hemorrhage before any antiplatelet or thrombolytic therapy is administered.
For long-term prevention, the calculus is different but still delicate. Aspirin provides a modest absolute risk reduction in ischemic events and a modest absolute increase in major bleeding events. Whether the net benefit is positive depends heavily on baseline stroke risk, baseline bleeding risk, age, and whether the patient already has established cardiovascular or cerebrovascular disease.
Mechanism: Irreversible COX-1 & TXA2 Blockade
Aspirin's antiplatelet effect stems from irreversible acetylation of cyclooxygenase-1 (COX-1) at serine 529, inactivating the enzyme for the entire 7–10 day lifespan of the platelet. Platelets are anucleate and cannot synthesize new COX-1, so a single low dose produces a durable effect. The downstream consequence is suppression of thromboxane A2 (TXA2), a potent platelet aggregator and vasoconstrictor.
Why This Favors Ischemic Stroke Prevention
- Most ischemic strokes originate from platelet-rich thrombi — either atherothrombotic (formed on ruptured atherosclerotic plaques in the carotid, vertebral, or intracranial arteries) or embolic from the heart or aortic arch.
- Suppressing TXA2-driven aggregation reduces the likelihood that a small platelet nidus progresses to an occlusive thrombus.
- Even low doses (75–100 mg/day) achieve near-complete platelet COX-1 inhibition because the effect is cumulative and irreversible.
Why This Raises Bleeding Risk
- The same TXA2 suppression impairs the primary hemostatic response at sites of vascular injury.
- Aspirin also inhibits COX-1 in the gastric mucosa, reducing protective prostaglandins and increasing the risk of upper-GI bleeding — the most common serious aspirin toxicity.
- Intracranial small-vessel disease, cerebral amyloid angiopathy, and hypertension-driven microvascular damage all create fragile vessels; aspirin amplifies the consequences of rupture.
Acute Ischemic Stroke Treatment: IST & CAST
Two parallel megatrials published in 1997 established that aspirin, given within 48 hours of acute ischemic stroke, modestly reduces recurrent stroke and death. Together they enrolled approximately 40,000 patients — the largest acute-stroke antiplatelet dataset ever assembled.
International Stroke Trial (IST, 1997)
- Enrolled 19,435 patients with suspected acute ischemic stroke within 48 hours of onset.
- Factorial design: aspirin 300 mg/day vs no aspirin, and subcutaneous heparin vs no heparin, for 14 days or until discharge.
- Aspirin produced a significant reduction in recurrent ischemic stroke within 14 days (2.8% vs 3.9%) with no significant excess of hemorrhagic stroke.
- At 6 months, aspirin was associated with a small but meaningful reduction in death or dependency.
Chinese Acute Stroke Trial (CAST, 1997)
- Enrolled 21,106 patients with acute ischemic stroke within 48 hours at 413 Chinese hospitals.
- Aspirin 160 mg/day vs placebo for up to 4 weeks.
- Aspirin reduced early mortality (3.3% vs 3.9%) and recurrent ischemic stroke (1.6% vs 2.1%).
- A small absolute increase in hemorrhagic stroke was outweighed by the reduction in ischemic events.
Pooled Interpretation
Combined, IST and CAST demonstrate that early aspirin (160–300 mg) within 48 hours of ischemic stroke prevents approximately 9 deaths or recurrent strokes per 1,000 patients treated in the first few weeks. Current guidelines recommend aspirin 160–325 mg within 24–48 hours of ischemic stroke onset, after hemorrhage has been excluded by imaging and after any tPA has been completed (aspirin is held for 24 hours post-thrombolysis).
Secondary Prevention After Stroke or TIA
Once a patient has had an ischemic stroke or transient ischemic attack (TIA), the risk of a recurrent event is substantial — approximately 10–20% within the first year without treatment. This is the population in which antiplatelet therapy provides the clearest net benefit.
Antithrombotic Trialists' Collaboration Meta-Analyses
- The Antithrombotic Trialists' (ATT) Collaboration pooled individual-patient data from dozens of randomized trials of antiplatelet therapy.
- In secondary prevention populations (prior MI, stroke, or TIA), antiplatelet therapy reduced serious vascular events by approximately 22% relative risk reduction, translating to roughly 36 fewer vascular events per 1,000 patients treated over about 2 years.
- The benefit in recurrent stroke prevention was clear: approximately 25 fewer nonfatal strokes per 1,000 secondary-prevention patients treated.
- Major extracranial bleeding was roughly doubled but the absolute excess was small compared with the event reduction.
CHANCE Trial (2013) — Minor Stroke/High-Risk TIA
- Enrolled 5,170 Chinese patients with minor ischemic stroke (NIHSS ≤ 3) or high-risk TIA (ABCD2 ≥ 4) within 24 hours of onset.
- Short-term dual antiplatelet therapy: clopidogrel 300 mg loading + 75 mg/day plus aspirin 75 mg/day for 21 days, then clopidogrel alone to 90 days, vs aspirin alone.
- DAPT reduced 90-day stroke recurrence from 11.7% to 8.2% (HR 0.68) with no significant increase in moderate or severe bleeding.
POINT Trial (2018) — Replication in Western Population
- Enrolled 4,881 patients with minor stroke or high-risk TIA in the US, Canada, Europe, Australia, and New Zealand.
- Aspirin + clopidogrel (600 mg load, then 75 mg/day) for 90 days vs aspirin alone.
- DAPT reduced major ischemic events from 6.5% to 5.0% (HR 0.75) but increased major hemorrhage from 0.4% to 0.9%.
- Prespecified analysis suggested most benefit accrued within the first 21 days — supporting a 21-day DAPT window rather than 90 days.
Current practice after minor stroke or high-risk TIA: aspirin plus clopidogrel for 21 days (loading dose then daily), followed by long-term single-agent antiplatelet therapy.
Primary Prevention: The Modern Picture
Primary prevention refers to aspirin use in individuals who have never had a cardiovascular or cerebrovascular event. Three large trials published in 2018 dramatically reshaped this space, narrowing or eliminating the net benefit that had been assumed for decades.
ARRIVE (2018) — Moderate-Risk Patients
- Enrolled 12,546 adults with moderate estimated cardiovascular risk (no diabetes, no prior CVD) across Europe and the US.
- Aspirin 100 mg/day vs placebo over median 5 years.
- No significant difference in the primary composite of cardiovascular death, MI, unstable angina, stroke, or TIA (4.3% vs 4.5%).
- Gastrointestinal bleeding doubled with aspirin (0.97% vs 0.46%).
ASCEND (2018) — Adults with Diabetes
- Enrolled 15,480 adults with diabetes but no established cardiovascular disease.
- Aspirin 100 mg/day vs placebo, median 7.4 years follow-up.
- Serious vascular events reduced modestly (8.5% vs 9.6%, rate ratio 0.88).
- Major bleeding increased to a similar degree (4.1% vs 3.2%, rate ratio 1.29).
- The authors concluded that the absolute benefits were "largely counterbalanced" by the bleeding hazard.
ASPREE (2018) — Healthy Older Adults
- Enrolled 19,114 community-dwelling adults age ≥70 (or ≥65 in US minorities) without prior CVD, dementia, or disability.
- Aspirin 100 mg/day vs placebo, median 4.7 years.
- No reduction in cardiovascular events; a significant increase in major hemorrhage (8.6 vs 6.2 events per 1,000 person-years).
- Unexpectedly, all-cause mortality was higher in the aspirin group, largely driven by cancer deaths — a signal that remains debated but strongly argues against aspirin initiation in healthy older adults.
Collectively, these trials show that in contemporary practice — with widespread statin use, blood pressure control, and smoking cessation reducing baseline cardiovascular risk — the absolute benefit of aspirin in primary prevention has shrunk to the point where it is often outweighed by bleeding harm.
Atrial Fibrillation: Why Aspirin Is Now Inadequate
Atrial fibrillation (AF) is a leading cause of cardioembolic ischemic stroke, producing strokes that are typically larger, more disabling, and more often fatal than non-AF strokes. Historically aspirin was considered a reasonable alternative to warfarin for lower-risk AF patients. That view has been abandoned.
- Meta-analyses show aspirin reduces AF-related stroke by only about 19%, compared with approximately 64% reduction with warfarin and similar or better reduction with direct oral anticoagulants (DOACs: apixaban, rivaroxaban, dabigatran, edoxaban).
- DOACs produce less intracranial hemorrhage than warfarin and substantially more effective stroke prevention than aspirin, with comparable or lower major bleeding overall.
- Current AHA/ACC/HRS and ESC guidelines recommend oral anticoagulation (preferably a DOAC) for AF patients with CHA2DS2-VASc scores ≥ 2 in men or ≥ 3 in women. Aspirin is no longer recommended as stroke prophylaxis for AF.
This is one of the most important practical points in modern stroke prevention: a patient with AF who is taking "just aspirin" is undertreated and should be reassessed for anticoagulation unless a specific contraindication exists.
USPSTF 2022 Recommendation
The US Preventive Services Task Force updated its aspirin guidance in April 2022, reflecting the ARRIVE/ASCEND/ASPREE evidence. The recommendation marked a significant retreat from earlier, more permissive guidance.
Age 40–59 with ≥10% 10-Year CVD Risk
- Grade C recommendation: the decision to initiate low-dose aspirin "should be an individual one." Persons who are not at increased bleeding risk and are willing to take daily aspirin may obtain a small net benefit.
- The net benefit is described as "small" and declines with advancing age as bleeding risk rises.
Age ≥60
- Grade D recommendation: the USPSTF recommends against initiating low-dose aspirin for primary prevention of CVD in adults 60 and older.
- Evidence indicates the net benefit is negligible to negative because bleeding risk increases with age.
Patients Already on Aspirin
The USPSTF did not recommend stopping aspirin in patients already taking it for primary prevention; that decision should be individualized with a clinician, weighing current risk factors, bleeding history, and patient preference. Patients taking aspirin for secondary prevention (after MI, stroke, or stent placement) were not covered by this recommendation — they should continue as indicated by their cardiovascular or neurological team.
Hemorrhagic Stroke Risk Quantified
Aspirin increases hemorrhagic stroke risk, but the absolute magnitude is small and must be weighed against the ischemic stroke reduction.
- Meta-analyses estimate aspirin increases hemorrhagic stroke risk by approximately 0.03% per year (about 3 additional intracranial hemorrhages per 10,000 patient-years).
- The ATT primary prevention meta-analysis found hemorrhagic stroke increased from 0.07% to 0.10% per year with aspirin — an absolute excess of 3 events per 10,000 person-years.
- Total stroke was essentially unchanged in primary prevention because the ischemic reduction and hemorrhagic increase nearly cancelled; the net-benefit argument in primary prevention therefore rested on myocardial infarction reduction, not stroke reduction.
- Risk factors that amplify hemorrhagic risk on aspirin: uncontrolled hypertension, advanced age, cerebral amyloid angiopathy, prior intracranial hemorrhage, concomitant anticoagulation, chronic kidney disease, and heavy alcohol use.
In secondary prevention after ischemic stroke, the ischemic benefit dominates and the small hemorrhagic increase is worth accepting. In primary prevention, particularly in older adults, the ratio shifts unfavorably.
Aspirin + Clopidogrel (DAPT) Duration
Dual antiplatelet therapy combining aspirin and clopidogrel is more potent than either alone but carries greater bleeding risk. Getting the duration right is critical.
Minor Stroke or High-Risk TIA
- Based on CHANCE and POINT, DAPT is given for 21 days, followed by single-agent antiplatelet therapy (typically aspirin or clopidogrel alone).
- Beyond 21 days, bleeding risk continues to accumulate while incremental ischemic benefit diminishes.
Symptomatic Intracranial Atherosclerotic Disease
- Based on the SAMMPRIS trial and subsequent analyses, DAPT is typically extended to 90 days after ischemic events attributed to intracranial stenosis ≥70%, given the very high early recurrence risk.
After Cardiac Stenting
- DAPT duration after coronary stenting is determined by cardiology, typically 6–12 months for drug-eluting stents, and may be shortened or extended based on bleeding vs ischemic risk.
- In stroke patients with concurrent cardiac stents, coordination between neurology and cardiology teams is essential.
Long-Term DAPT Is Generally Avoided
The MATCH and CHARISMA trials showed that chronic (beyond 3 months) DAPT after stroke does not provide meaningful additional ischemic benefit and significantly increases major and intracranial bleeding. Long-term DAPT in stroke patients should be reserved for specific indications, not used routinely.
Special Populations: Diabetes, Women, Elderly
Diabetes
- ASCEND demonstrated that in diabetes without established CVD, the benefit of aspirin is quantitatively similar to the bleeding harm.
- Current ADA guidance considers aspirin for primary prevention only in adults with diabetes at increased cardiovascular risk, after discussion of bleeding risk — not as a routine recommendation.
- For secondary prevention in diabetes, aspirin remains clearly indicated.
Women
- Historically, sex-stratified analyses suggested aspirin had a stronger stroke-prevention signal in women and a stronger MI-prevention signal in men, but contemporary trials (including the Women's Health Study) show the differences are modest.
- The USPSTF 2022 recommendation does not differ by sex.
- Aspirin has a distinct role in preventing preeclampsia in high-risk pregnancies (low-dose aspirin starting 12–28 weeks gestation) — a separate indication from cerebrovascular prevention.
Elderly
- ASPREE showed no cardiovascular benefit and significant bleeding harm in healthy adults ≥70 starting aspirin de novo.
- Falls risk, polypharmacy, renal impairment, and frailty all amplify aspirin harm in older adults.
- For secondary prevention, age alone is not a reason to stop aspirin, but bleeding risk should be continuously reassessed.
Practical Dosing & Acute Caveats
Chronic Antiplatelet Dosing
- 81 mg/day (low-dose, "baby aspirin") is the standard for chronic antiplatelet therapy in both primary and secondary prevention.
- Higher maintenance doses (162–325 mg/day) do not provide additional antiplatelet efficacy but do increase gastrointestinal bleeding.
- Enteric-coated formulations reduce gastric symptoms but do not clearly reduce serious upper-GI bleeding in randomized data.
Acute MI: Chewable 325 mg
- In suspected acute myocardial infarction, a single non-enteric-coated 325 mg aspirin should be chewed to accelerate absorption; ISIS-2 demonstrated this produces a 23% reduction in vascular mortality at 5 weeks.
- Chewing bypasses slow gastric dissolution and achieves therapeutic platelet inhibition within minutes.
Acute Stroke: Rule Out Hemorrhage First
- Do not give aspirin to a patient with suspected acute stroke until brain imaging has excluded intracerebral hemorrhage.
- The clinical presentations of ischemic and hemorrhagic stroke are indistinguishable at the bedside; a non-contrast head CT is mandatory before any antiplatelet or thrombolytic therapy.
- If intravenous thrombolysis (alteplase or tenecteplase) is given, aspirin is held for 24 hours to avoid compounding hemorrhage risk.
- Once hemorrhage is excluded and any thrombolysis is complete, 160–325 mg aspirin is given within 24–48 hours of symptom onset, then transitioned to long-term single-agent or brief DAPT per CHANCE/POINT protocols.
Stopping Aspirin
- Abrupt discontinuation of chronic aspirin in secondary prevention patients has been associated with a rebound in ischemic events in observational data.
- Perioperative aspirin management is individualized: continued for most low-bleeding-risk surgeries in secondary-prevention patients, held for neurosurgical and high-bleeding-risk procedures.
References
- ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. Lancet. 1988;2(8607):349-360.
- International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19,435 patients with acute ischaemic stroke. Lancet. 1997;349(9065):1569-1581.
- Search PubMed
- Antithrombotic Trialists' (ATT) Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373(9678):1849-1860.
- Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack (CHANCE). N Engl J Med. 2013;369(1):11-19.
- Johnston SC, Easton JD, Farrant M, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA (POINT). N Engl J Med. 2018;379(3):215-225.
- Gaziano JM, Brotons C, Coppolecchia R, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet. 2018;392(10152):1036-1046.
- ASCEND Study Collaborative Group. Effects of aspirin for primary prevention in persons with diabetes mellitus. N Engl J Med. 2018;379(16):1529-1539.
- McNeil JJ, Wolfe R, Woods RL, et al. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly (ASPREE). N Engl J Med. 2018;379(16):1509-1518.
- US Preventive Services Task Force. Aspirin use to prevent cardiovascular disease: US Preventive Services Task Force recommendation statement. JAMA. 2022;327(16):1577-1584.
- Chimowitz MI, Lynn MJ, Derdeyn CP, et al. Stenting versus aggressive medical therapy for intracranial arterial stenosis (SAMMPRIS). N Engl J Med. 2011;365(11):993-1003.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH). Lancet. 2004;364(9431):331-337.
Connections
- Aspirin Overview
- Stroke
- Aspirin for Heart Attack Prevention
- Aspirin Health Benefits
- Aspirin Side Effects
- Oral Microbiome
- Anti-Inflammatory Diet
- Diabetes
- Atrial Fibrillation
- Cardiovascular Disease
- Hypertension
- Aspirin and Cancer Prevention
- Aspirin and the Kidneys
- Preeclampsia