Aspirin & Cancer Prevention: Colorectal Cancer, Lynch Syndrome & Adjuvant Therapy
Few drugs have had as strange and winding a relationship with cancer as aspirin. A century-old pain reliever originally developed for fever and inflammation, aspirin has accumulated three decades of epidemiological, clinical-trial, and mechanistic evidence suggesting it can reduce the incidence of colorectal cancer and perhaps a handful of other gastrointestinal malignancies. For people with Lynch syndrome — a hereditary colorectal cancer predisposition — the evidence is strong enough that aspirin is now part of mainstream clinical guidance. For the average-risk adult, the picture is much murkier, and the 2022 reversal of the U.S. Preventive Services Task Force recommendation has made clear just how delicate the balance between bleeding risk and cancer benefit really is.
Table of Contents
- Introduction — The 30-Year Colorectal Cancer Story
- Biological Rationale: COX-2, Prostaglandins & Platelets
- Observational Evidence: Nurses' Health & Health Professionals Studies
- Randomized Trial Evidence: Pooled Cardiovascular Trials (Rothwell)
- CAPP2: Aspirin for Lynch Syndrome
- The Add-Aspirin Adjuvant Trial
- USPSTF: The 2016 Recommendation & 2022 Walk-Back
- Other Cancers with Possible Signals
- Dose, Duration & Timing
- Adjuvant Aspirin & the PIK3CA-Mutant Hypothesis
- Risk-Benefit Framing: Bleeding vs. Cancer Reduction
- Practical Guidance & Patient Selection
- References
- Connections
- Featured Videos
Introduction — The 30-Year Colorectal Cancer Story
The hypothesis that aspirin might prevent cancer dates to the late 1980s, when case-control and cohort studies began to notice that regular aspirin users had lower rates of colorectal cancer than non-users. Over the following three decades, what started as a curious epidemiological signal has become one of the most thoroughly investigated pharmacological cancer-prevention hypotheses in medicine. Three streams of evidence have converged:
- Observational cohorts — large prospective studies (Nurses' Health Study, Health Professionals Follow-Up Study, and others) consistently found a 20–40% reduction in colorectal cancer incidence among long-term regular aspirin users.
- Post-hoc analyses of cardiovascular trials — when Peter Rothwell and colleagues pooled long-term follow-up from randomized trials originally designed to test aspirin for heart attack and stroke prevention, they found substantial reductions in cancer death, particularly for gastrointestinal cancers.
- Dedicated cancer-prevention trials — CAPP2 tested aspirin in Lynch syndrome carriers and found a durable reduction in colorectal cancer incidence after long follow-up.
Yet this apparent convergence hides genuine uncertainty. The Aspirin in Reducing Events in the Elderly (ASPREE) trial, a large primary-prevention study in older adults, found no cancer benefit — and actually raised concerns about increased cancer mortality in the aspirin arm. The USPSTF, which issued a qualified recommendation for aspirin as colorectal cancer prevention in 2016, reversed course in 2022 after new data failed to confirm earlier estimates of benefit. Aspirin for cancer prevention is no longer a recommendation for most adults — but for Lynch syndrome, it has gone from experimental to standard-of-care consideration.
Biological Rationale: COX-2, Prostaglandins & Platelets
Aspirin is not a targeted anticancer drug in the conventional sense. It is an irreversible inhibitor of the cyclooxygenase (COX) enzymes — COX-1 and COX-2 — which produce prostaglandins from arachidonic acid. The anti-cancer hypothesis rests on three interlocking mechanisms:
1. COX-2 in Colorectal Carcinogenesis
COX-2 is rarely expressed in normal colonic epithelium but is dramatically upregulated in colorectal adenomas and carcinomas. This upregulation is one of the earliest molecular events in the adenoma-to-carcinoma sequence and drives several pro-tumor effects:
- Increased production of prostaglandin E2 (PGE2), which promotes proliferation, inhibits apoptosis, and stimulates angiogenesis
- Suppression of antitumor immune responses through PGE2-mediated effects on T cells and macrophages
- Enhanced invasion and metastasis through upregulation of matrix metalloproteinases
By inhibiting COX-2 — even with the relatively modest potency of low-dose aspirin — the tumor microenvironment becomes less hospitable to malignant transformation.
2. Platelet-Tumor Interactions
A mechanism that has gained increasing attention involves platelets. Circulating tumor cells recruit and activate platelets, which cloak them from immune surveillance, help them survive shear stress in the bloodstream, and promote their extravasation into metastatic niches. Low-dose aspirin irreversibly acetylates platelet COX-1, shutting down thromboxane A2 production and impairing platelet aggregation for the life of the platelet (approximately 7–10 days). This platelet-centric mechanism is particularly attractive because:
- It explains why even very low doses (75–100 mg daily) — insufficient to fully inhibit tissue COX-2 — might still reduce metastasis
- It aligns with Rothwell's finding that aspirin reduced cancer-related death and distant metastasis, not just incidence
- Platelets are implicated in seeding liver metastases from colorectal cancer, the dominant site of CRC metastatic failure
3. Effects on the Adenoma-to-Carcinoma Sequence
Randomized trials in patients with prior adenomas have shown that aspirin reduces recurrent adenoma formation — suggesting it acts at an early, pre-malignant stage rather than only on established tumors. The combined mechanisms may also include modulation of Wnt/β-catenin signaling, inhibition of NF-κB, and direct effects on cancer stem cells.
Observational Evidence: Nurses' Health & Health Professionals Follow-Up Studies
Two of the most influential datasets in the aspirin-cancer literature come from long-running Harvard-based cohorts. Andrew Chan and colleagues published a landmark analysis in the New England Journal of Medicine in 2007 combining data from the Nurses' Health Study (NHS) and the Health Professionals Follow-Up Study (HPFS). Key findings:
- Regular aspirin use (≥2 standard tablets per week) was associated with a statistically significant reduction in colorectal cancer incidence
- The benefit was dose-dependent — higher weekly doses produced larger reductions
- The benefit emerged only after at least 10 years of regular use — a finding consistent across multiple observational studies
- The protective association was strongest for cancers overexpressing COX-2, supporting the mechanistic hypothesis
Subsequent analyses of the same cohorts extended the findings to other gastrointestinal cancers and showed an interaction with tumor molecular features — notably PIK3CA mutation status and mismatch-repair status. Observational studies have the well-known limitation that regular aspirin users may differ systematically from non-users (healthier lifestyles, better healthcare access), but the consistency of the finding across cohorts, its dose- and duration-dependence, and its alignment with biological plausibility made it hard to dismiss as confounding alone.
Randomized Trial Evidence: Pooled Cardiovascular Trials (Rothwell)
The single most influential body of randomized evidence for aspirin and cancer came not from cancer-prevention trials but from long-term follow-up of cardiovascular trials. Between 2010 and 2012, Peter Rothwell and colleagues at Oxford published a series of papers in The Lancet pooling individual-patient data from randomized trials of aspirin for cardiovascular prevention, then extending follow-up many years beyond the original trial periods.
Rothwell et al., Lancet 2010 (Long-Term Colorectal Cancer)
- Pooled four trials of daily aspirin (mean duration 6 years; median follow-up 18.3 years)
- Aspirin reduced 20-year colorectal cancer incidence by approximately 24% and colorectal cancer mortality by approximately 35%
- The benefit was greatest for proximal (right-sided) colon cancers, which are poorly detected by sigmoidoscopy
- A dose of 75 mg daily appeared sufficient — higher doses did not add benefit
Rothwell et al., Lancet 2011 (Death from Any Cancer)
- Pooled eight trials (25,570 patients) of daily aspirin
- Aspirin reduced death from any cancer by approximately 21% during the trial periods, with benefit increasing over time
- 20-year risk of cancer death was reduced across multiple solid tumor types, with the strongest signals in gastrointestinal cancers
- Latency: the benefit for cancer death began emerging around 5 years of treatment and grew thereafter
Rothwell et al., Lancet 2012 (Cancer Incidence & Metastasis)
- Pooled 51 randomized trials to examine effects on cancer incidence, mortality, and non-vascular death
- Daily aspirin reduced the risk of being diagnosed with distant metastases by approximately 30–40%, particularly for adenocarcinomas
- The reduction in metastasis was detectable even during the trial periods — earlier than incidence reductions — supporting the platelet-centric mechanism
These analyses transformed the conversation. They showed that the observational findings were not merely confounded lifestyle artifacts — randomized assignment to aspirin produced real, sustained reductions in cancer outcomes in long-term follow-up. They also raised the cancer story from one of prevention alone to one of possible metastasis suppression, suggesting aspirin might have a role in treating, not just preventing, cancer.
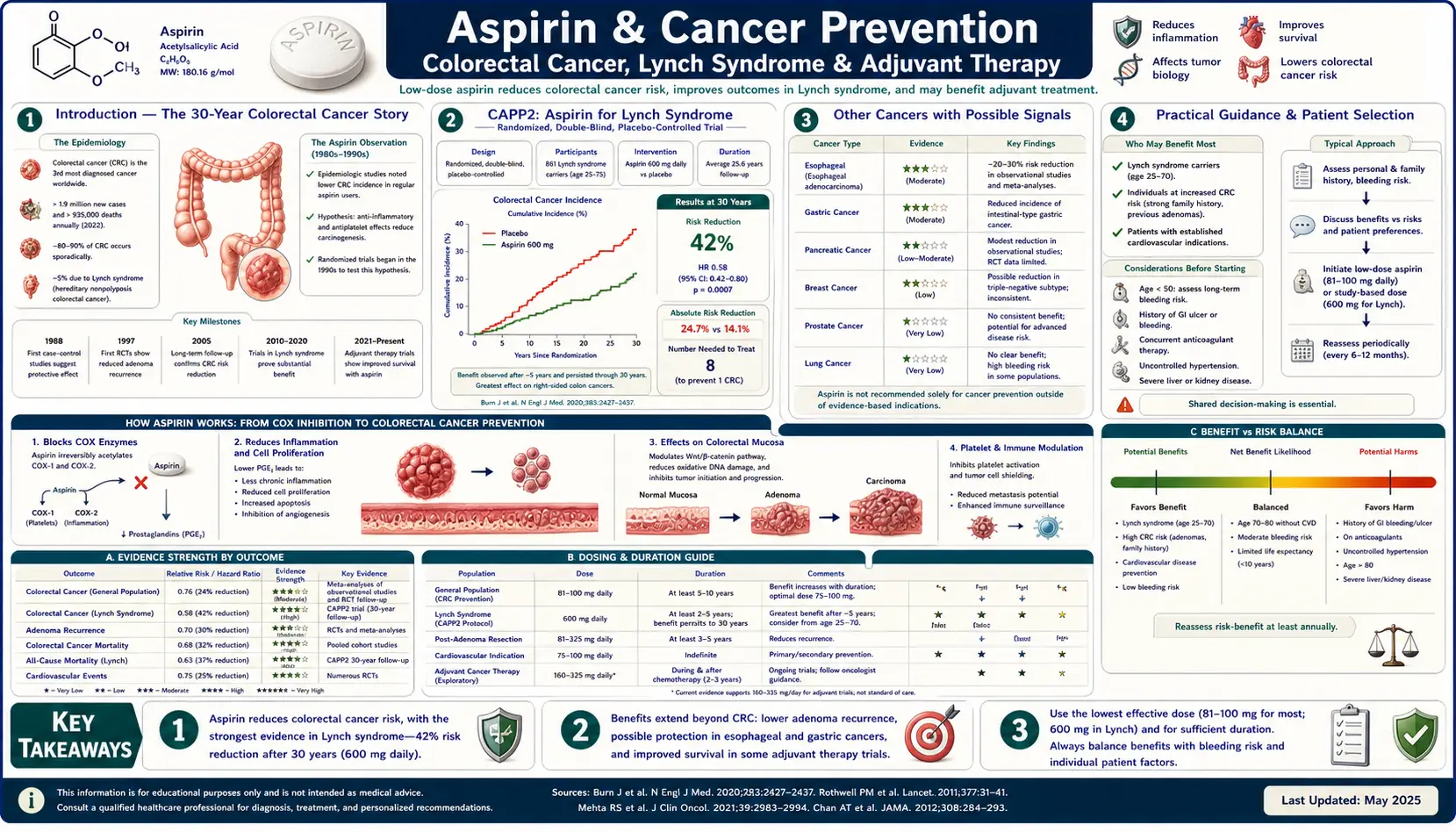
CAPP2: Aspirin for Lynch Syndrome
Lynch syndrome (hereditary nonpolyposis colorectal cancer) is caused by germline mutations in DNA mismatch-repair genes (MLH1, MSH2, MSH6, PMS2, or EPCAM) and confers a lifetime colorectal cancer risk of roughly 50–80%. Because affected individuals are at such high baseline risk, they are an ideal population in which to test chemoprevention — a small relative risk reduction translates into a large absolute benefit, and the risk-benefit calculus tilts much more favorably than in the general population.
The CAPP2 trial (Colorectal Adenoma/carcinoma Prevention Programme 2), led by John Burn at Newcastle, was designed to test exactly this question.
CAPP2 Design
- Population: 861 Lynch syndrome carriers enrolled across 43 international centers
- Intervention: 600 mg aspirin daily vs. placebo, with a separate resistant-starch arm
- Minimum treatment duration: at least 2 years (mean ~25 months)
- Primary endpoint: colorectal cancer incidence
CAPP2 Results — Burn et al., Lancet 2011
The initial per-protocol analysis at a mean of 55.7 months of follow-up found that aspirin reduced colorectal cancer incidence in Lynch syndrome carriers who took aspirin for at least 2 years. The effect was not apparent in intention-to-treat analysis at short follow-up, because the benefit appeared delayed — a pattern already familiar from the cardiovascular-trial pooled analyses.
CAPP2 Long-Term Follow-Up — Burn et al., Lancet 2020
The 2020 update, with a planned 10-year follow-up, was decisive:
- Participants who received aspirin for at least 2 years had a roughly 50% reduction in colorectal cancer incidence compared with placebo
- The benefit was durable, persisting long after treatment was stopped
- The effect was consistent across mismatch-repair gene types
- Overall cancer reduction (all Lynch-associated tumors) was also significant
CAPP2 moved aspirin from hypothesis to recommendation in Lynch syndrome. UK NICE guidance and multiple international society statements now support considering daily aspirin in Lynch syndrome carriers as part of the overall cancer-prevention strategy, alongside surveillance colonoscopy. The ongoing CaPP3 trial is attempting to refine the dose, comparing 100 mg, 300 mg, and 600 mg daily to identify the lowest effective dose — a critical question given that 600 mg carries meaningful bleeding risk.
The Add-Aspirin Adjuvant Trial
If aspirin can prevent cancer and reduce metastasis in epidemiological and mechanistic studies, can it improve survival in patients who already have cancer? That is the question of the Add-Aspirin trial — a large, international, randomized, placebo-controlled adjuvant trial that enrolls patients who have completed standard curative treatment for early-stage solid tumors.
Add-Aspirin Design
- Sponsor: MRC Clinical Trials Unit at University College London, with sites in the UK, India, and Ireland
- Population: patients with non-metastatic colorectal, breast, gastro-esophageal, and prostate cancers after completion of primary treatment
- Design: a randomized, double-blind comparison of 100 mg aspirin daily, 300 mg aspirin daily, and placebo for 5 years, with separate cohorts (and separate primary endpoints) for each tumor type
- Primary endpoints: disease-free survival (colorectal, breast, gastro-esophageal) and biochemical recurrence-free survival (prostate)
- Enrollment target: approximately 11,000 patients across all four cohorts — one of the largest adjuvant trials ever conducted
Add-Aspirin is designed with a pragmatic run-in period to exclude patients who cannot tolerate aspirin, and it tests two doses to begin resolving the dose-response question directly. Interim results have not yet matured across all cohorts; the trial's outputs over the coming years will be among the most important in the aspirin-and-cancer story. If Add-Aspirin shows a survival benefit, aspirin could be repurposed as an inexpensive adjuvant therapy with broad applicability. If it is negative, it will significantly narrow the case for aspirin beyond Lynch syndrome.
USPSTF: The 2016 Recommendation & 2022 Walk-Back
In 2016, the U.S. Preventive Services Task Force issued a qualified recommendation (Grade B for some adults, Grade C for others) supporting low-dose aspirin for the primary prevention of cardiovascular disease and colorectal cancer in adults aged 50–59 at elevated 10-year cardiovascular risk, willing to take aspirin for at least 10 years, and without increased bleeding risk. This was the closest the aspirin-for-cancer hypothesis ever came to formal endorsement for average-risk adults.
What Changed in 2022
In April 2022, the USPSTF substantially revised its recommendation:
- The Task Force withdrew the colorectal cancer prevention benefit from its rationale for recommending aspirin
- It concluded that the evidence was insufficient to support aspirin initiation specifically for colorectal cancer prevention in average-risk adults
- It recommended against initiating low-dose aspirin for primary CVD prevention in adults aged 60 and older, and only a small-net-benefit (Grade C) for adults 40–59 with ≥10% 10-year CVD risk
Why the Reversal?
Several developments drove the change:
- ASPREE trial (2018) — in adults 70 and older (65+ for some U.S. minority groups), low-dose aspirin did not reduce cardiovascular events and was associated with increased all-cause mortality, with an unexpected signal of increased cancer-related death
- ARRIVE and ASCEND — two other primary-prevention trials published in 2018 showed smaller cardiovascular benefits than older trials and meaningful bleeding harms
- Updated modeling suggested that the long latency required to see cancer benefit (5–10+ years) combined with immediate bleeding risk produced a narrower net benefit than previously estimated — especially in older adults, whose bleeding risk rises sharply
Importantly, the USPSTF recommendation applies to average-risk primary prevention. It does not apply to Lynch syndrome, to patients with established cardiovascular disease (for whom secondary prevention with aspirin remains standard), or to patients with other strong indications. The 2022 update is a narrowing of the average-risk case, not a rejection of aspirin's cancer-prevention biology.
Other Cancers with Possible Signals
Colorectal cancer has the strongest evidence base, but observational and pooled trial data have generated signals for several other malignancies. The quality of evidence varies considerably.
Esophageal & Gastric Cancers
- Observational cohorts consistently associate regular aspirin use with reduced esophageal adenocarcinoma incidence (roughly 30–40% reduction in some analyses)
- Rothwell's pooled analyses also suggest reduced mortality from upper GI cancers
- The AspECT trial (aspirin plus esomeprazole in Barrett's esophagus) reported modest improvements in a composite endpoint but did not show large individual-endpoint effects
- Evidence quality: moderate — consistent observational signal, limited dedicated RCT data
Pancreatic Cancer
- Evidence is inconsistent. Some cohort studies suggest modest reductions with long-term aspirin use; others find no effect
- Case-control studies are vulnerable to recall bias for this rapidly fatal cancer
- Evidence quality: low — not a basis for clinical action
Ovarian Cancer
- Pooled analyses of observational cohorts (NHS, HPFS, and others) suggest an approximately 10–20% reduction in epithelial ovarian cancer incidence with regular low-dose aspirin use
- Mechanism may relate to suppressed inflammation in ovarian surface epithelium
- Evidence quality: moderate observational, no dedicated RCT
Prostate Cancer
- Evidence is mixed. Some cohorts suggest modest reductions in lethal prostate cancer (not indolent disease), consistent with an antimetastatic effect
- The prostate cohort of the Add-Aspirin trial is the best prospective test
- Evidence quality: inconclusive
Breast Cancer
- Observational studies show mixed and generally small effects on incidence
- The breast cohort of Add-Aspirin is testing the adjuvant question directly
- Evidence quality: inconclusive for incidence, pending RCT data for adjuvant use
The overall picture: colorectal cancer has the strongest and most reproducible evidence. The other gastrointestinal cancers have plausible, moderate signals. Non-GI cancers are largely speculative without RCT confirmation. None of these signals is currently strong enough to justify aspirin use for non-GI cancer prevention outside a clinical trial.
Dose, Duration & Timing
A striking feature of the cancer-prevention evidence is how slowly it matures. Unlike cardiovascular benefits, which begin within months, cancer benefits from aspirin take years to become visible in the data.
Duration — The 5-to-10-Year Rule
- Observational studies: colorectal cancer reduction typically only detectable after 10+ years of regular use
- Rothwell pooled trials: cancer mortality reductions emerged around 5 years of treatment, growing thereafter
- CAPP2 Lynch syndrome: benefit required at least 2 years of treatment and persisted for ≥10 years after cessation
This long latency is one of the key arguments against initiating aspirin for cancer prevention in older adults: if meaningful benefit requires 10 years, a 75-year-old starting aspirin has only a modest probability of living long enough to realize the benefit, while immediate bleeding risk is high.
Dose
- 75–100 mg daily (low-dose): sufficient for cardiovascular prevention and appears sufficient for colorectal cancer prevention in the pooled Rothwell analyses. This is the dose used in most primary-prevention trials (ASPREE, ASCEND, ARRIVE) and in the lower arm of Add-Aspirin.
- 300–325 mg daily (intermediate): the other arm of Add-Aspirin; also used in some historical trials.
- 600 mg daily (high): the dose used in CAPP2; effective for Lynch syndrome but with meaningful bleeding risk. CaPP3 is actively testing whether lower doses provide equivalent benefit.
Timing
Whether aspirin should be taken morning or evening, with or without food, has no established cancer-prevention implications. Enteric coating may reduce gastric irritation but does not appear to alter cancer-prevention efficacy. Consistency of long-term use matters more than timing.
Adjuvant Aspirin & the PIK3CA-Mutant Hypothesis
A provocative 2012 New England Journal of Medicine paper from Liao, Lochhead, Nishihara, Ogino, Chan, and colleagues suggested that the benefit of aspirin in colorectal cancer patients might be largely restricted to tumors with PIK3CA mutations. In their analysis of NHS/HPFS cohort data:
- Regular aspirin use after colorectal cancer diagnosis was associated with markedly improved cancer-specific survival in patients with PIK3CA-mutant tumors
- No similar benefit was observed in PIK3CA-wild-type tumors
- The hypothesis: PI3K signaling upregulates COX-2 and PGE2, creating a pathway where aspirin's COX inhibition is particularly effective
If confirmed, PIK3CA status would be the first molecular biomarker for aspirin benefit — a precision-medicine rationale for post-diagnosis aspirin in a defined subgroup (roughly 15–20% of colorectal cancers). However:
- Subsequent observational studies have produced inconsistent results
- The Add-Aspirin colorectal cohort is designed to allow pre-specified subgroup analysis by PIK3CA status
- As of 2025, routine clinical PIK3CA testing in colorectal cancer to guide aspirin use is not standard practice — the hypothesis remains promising but unconfirmed
The ASCOLT trial (Aspirin for Dukes C and High-Risk Dukes B Colorectal Cancer) is another dedicated adjuvant trial in post-surgical colorectal cancer patients that may further clarify this question.
Risk-Benefit Framing: Bleeding vs. Cancer Reduction
Any discussion of aspirin for cancer prevention is incomplete without the bleeding risk. Long-term low-dose aspirin roughly doubles the risk of major gastrointestinal bleeding and modestly increases the risk of hemorrhagic stroke. In absolute terms:
- For a 60-year-old adult at average cardiovascular and cancer risk, the absolute risk of a major bleed over 10 years on low-dose aspirin is on the order of 1–2%
- Bleeding risk rises steeply with age — an 80-year-old has roughly triple the bleeding risk of a 50-year-old
- Concurrent use of NSAIDs, anticoagulants, SSRIs, or corticosteroids further increases bleeding risk
- Helicobacter pylori infection is a potentiator of aspirin-related GI bleeding and should ideally be eradicated before long-term aspirin initiation
The Patient-Selection Problem
The ideal candidate for aspirin chemoprevention is someone with:
- High baseline cancer risk (Lynch syndrome is the paradigm)
- Low bleeding risk (no prior GI bleeding, no H. pylori, no concurrent bleeding-potentiating drugs, younger age)
- Sufficient life expectancy to accrue the 5–10-year latency benefit
- Genuine willingness and ability to take aspirin consistently for a decade or more
This describes a relatively narrow slice of the population. It describes Lynch syndrome carriers well. It describes average-risk 70-year-olds poorly — which is exactly why ASPREE failed to find benefit and why the USPSTF walked back its recommendation.
Practical Guidance & Patient Selection
This section is intended as a framework for patient-physician conversations — not a substitute for individualized medical advice.
Lynch Syndrome — the Clearest Case
For confirmed Lynch syndrome carriers, guidance from UK NICE and multiple international societies now supports considering daily aspirin as part of cancer-prevention strategy, in addition to surveillance colonoscopy. Typical considerations:
- Dose: pending CaPP3 results, 600 mg daily is the CAPP2 dose, though many clinicians use lower doses (100–300 mg) to balance bleeding risk
- Start age: often considered at age 25–30 or at the start of surveillance colonoscopy
- Duration: at least 2 years is the minimum supported by CAPP2; longer is reasonable in absence of bleeding
- Requires a physician with genetics/oncology familiarity — not a self-directed decision
Average-Risk Primary Prevention — Not Recommended
Based on 2022 USPSTF guidance and subsequent evidence, initiating aspirin solely for colorectal cancer prevention in average-risk adults is no longer recommended. Screening colonoscopy (or equivalent) remains the cornerstone of CRC prevention at average risk.
Established Cardiovascular Disease
Patients already on aspirin for established cardiovascular disease (secondary prevention after MI, stroke, coronary stenting, etc.) may derive ancillary cancer-prevention benefit as a bonus, but cancer prevention is not by itself a reason to continue or discontinue aspirin — the cardiovascular indication governs.
Colorectal Cancer Survivors
For patients who have completed curative treatment for colorectal cancer, post-diagnosis aspirin is a reasonable discussion point — but outside of a trial (such as Add-Aspirin or ASCOLT), the decision should be individualized based on bleeding risk, PIK3CA status if available, and other comorbidities. It is not yet standard adjuvant therapy.
Other Settings
- Familial adenomatous polyposis (FAP): aspirin is not a substitute for colectomy; its role is adjunctive and off-label
- Barrett's esophagus: aspirin plus PPI has modest supportive data from AspECT; decisions are individualized
- Non-GI cancer prevention: not supported by evidence outside clinical trials
References
Rothwell Pooled Analyses of Cardiovascular Trials
- Rothwell PM, Wilson M, Elwin CE, et al. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet. 2010;376(9754):1741-1750.
- Rothwell PM, Fowkes FG, Belch JF, Ogawa H, Warlow CP, Meade TW. Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet. 2011;377(9759):31-41.
- Rothwell PM, Wilson M, Price JF, Belch JF, Meade TW, Mehta Z. Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers during randomised controlled trials. Lancet. 2012;379(9826):1591-1601.
- Rothwell PM, Price JF, Fowkes FG, et al. Short-term effects of daily aspirin on cancer incidence, mortality, and non-vascular death: analysis of the time course of risks and benefits in 51 randomised controlled trials. Lancet. 2012;379(9826):1602-1612.
CAPP2 — Lynch Syndrome
- Burn J, Gerdes AM, Macrae F, et al. Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: an analysis from the CAPP2 randomised controlled trial. Lancet. 2011;378(9809):2081-2087.
- Burn J, Sheth H, Elliott F, et al. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: a double-blind, randomised, placebo-controlled trial. Lancet. 2020;395(10240):1855-1863.
Observational Cohort Evidence (Nurses' Health & HPFS)
- Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. New England Journal of Medicine. 2007;356(21):2131-2142.
- Chan AT, Giovannucci EL, Meyerhardt JA, Schernhammer ES, Curhan GC, Fuchs CS. Long-term use of aspirin and nonsteroidal anti-inflammatory drugs and risk of colorectal cancer. JAMA. 2005;294(8):914-923.
- Liao X, Lochhead P, Nishihara R, et al. Aspirin use, tumor PIK3CA mutation, and colorectal-cancer survival. New England Journal of Medicine. 2012;367(17):1596-1606.
Add-Aspirin Trial
- Coyle C, Cafferty FH, Rowley S, et al. ADD-ASPIRIN: A phase III, double-blind, placebo controlled, randomised trial assessing the effects of aspirin on disease recurrence and survival after primary therapy in common non-metastatic solid tumours. Contemporary Clinical Trials. 2016;51:56-64.
- MRC Clinical Trials Unit at UCL. Add-Aspirin Trial — official trial information page.
USPSTF Recommendations
- Bibbins-Domingo K; U.S. Preventive Services Task Force. Aspirin Use for the Primary Prevention of Cardiovascular Disease and Colorectal Cancer: U.S. Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine. 2016;164(12):836-845.
- US Preventive Services Task Force; Davidson KW, Barry MJ, Mangione CM, et al. Aspirin Use to Prevent Cardiovascular Disease: US Preventive Services Task Force Recommendation Statement. JAMA. 2022;327(16):1577-1584.
Contemporary Primary-Prevention Trials (Context for USPSTF Walk-Back)
- McNeil JJ, Nelson MR, Woods RL, et al. Effect of Aspirin on All-Cause Mortality in the Healthy Elderly (ASPREE). New England Journal of Medicine. 2018;379(16):1519-1528.
- ASCEND Study Collaborative Group; Bowman L, Mafham M, Wallendszus K, et al. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. New England Journal of Medicine. 2018;379(16):1529-1539.
Connections
- Aspirin Overview
- Cancer
- Aspirin Health Benefits
- Aspirin Side Effects
- Anti-Inflammatory Diet
- Metastatic Cancers
- Fenbendazole
- Heart Attack Prevention
- Aspirin and the Kidneys
- Stroke Prevention
- Coffee and Cancer Prevention
- Cardiovascular Disease
- Stroke
- Selenium and Cancer Prevention
- Colorectal Cancer — the malignancy with the strongest aspirin chemoprevention evidence, from the Rothwell pooled trials to CAPP2.