Iron Overload and Iron Toxicity: Hemochromatosis, Acute Poisoning, and Diagnosis
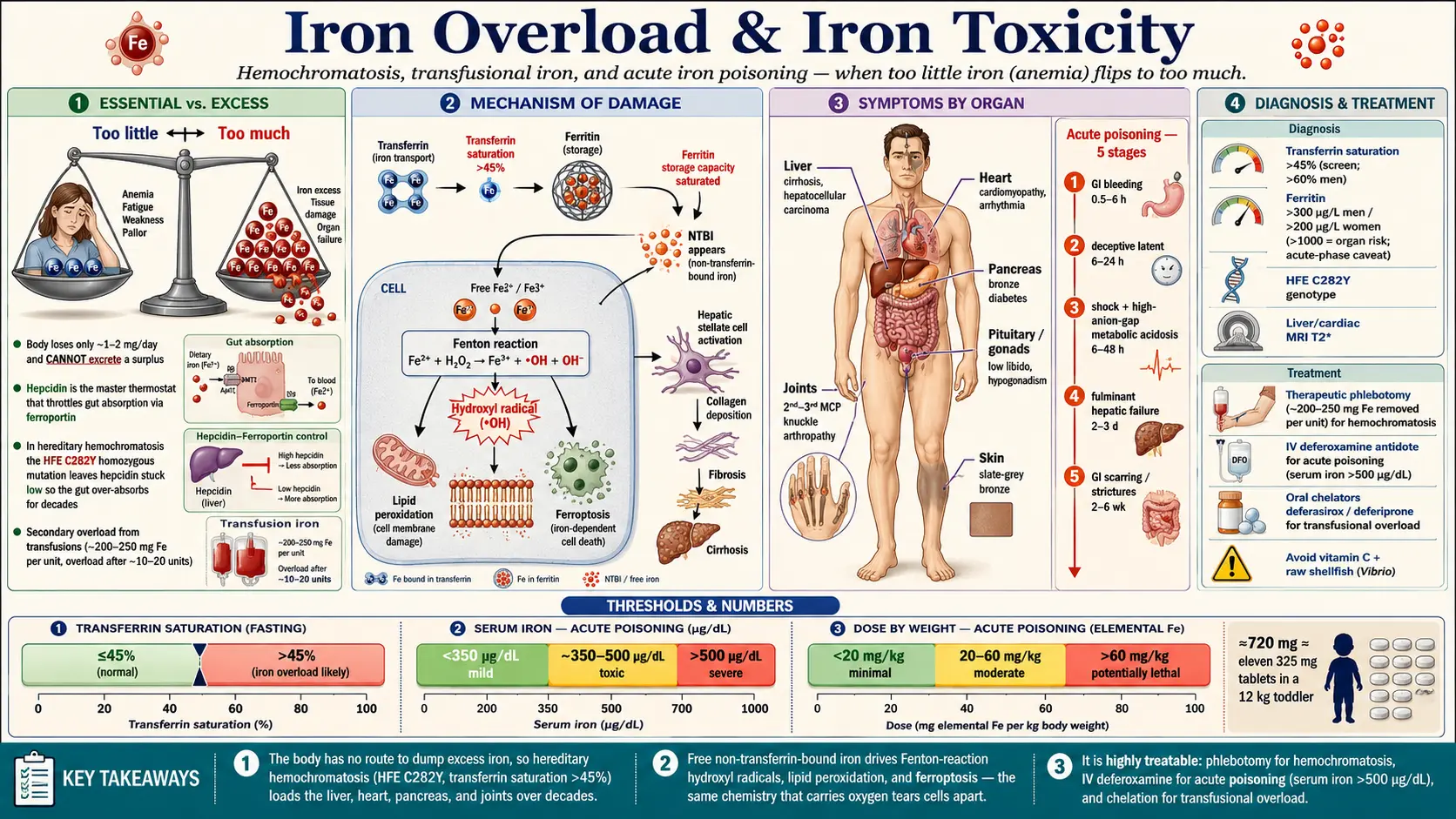
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Iron is essential for life — it carries oxygen in hemoglobin, runs the energy machinery in mitochondria, and powers dozens of enzymes. Our companion page on the nutrient, Iron (essential), covers why too little iron causes anemia, fatigue, and breathlessness. This page is the opposite story: what happens when the body holds too much iron. Iron is unusual because the body has no controlled way to shed a surplus — apart from small daily losses in shed gut and skin cells (about 1–2 mg a day), no hormone, kidney, or liver pathway actively excretes excess iron. Once it accumulates, it tends to stay.
“Iron overload” is an umbrella term for several conditions that all end in the same place — toxic iron deposited in vital organs — but arrive by very different roads. This page covers three distinct entities that are easy to confuse but must be told apart, because their causes, time courses, and treatments differ completely.
- Hereditary (genetic) hemochromatosis — a slow, lifelong condition, usually caused by inheriting two copies of a faulty HFE gene. The gut absorbs slightly too much iron year after year, and the surplus quietly builds up in the liver, heart, pancreas, joints, and hormone glands. It is often silent until middle age.
- Acute iron poisoning — a sudden, dose-dependent medical emergency that follows swallowing a large amount of iron at once. Historically it was one of the leading causes of poisoning deaths in young children, who mistook brightly colored adult iron tablets or prenatal vitamins for candy.
- Secondary (transfusional) iron overload — iron that accumulates because someone needs repeated blood transfusions, or because a diseased bone marrow drives the gut to absorb too much iron. People with certain chronic anemias — beta-thalassemia major, sickle cell disease, myelodysplastic syndromes — are most affected.
What ties all three together at the cellular level is a chemistry problem: when iron exceeds the body’s capacity to bind and store it safely, the unbound “free” iron becomes a powerful generator of reactive oxygen species — chemically aggressive molecules that damage cell membranes, proteins, and DNA. The organ that takes the most iron takes the most damage. This is why iron overload, left untreated, can end in cirrhosis, liver cancer, heart failure, and diabetes — yet it is also one of the most treatable causes of organ damage in medicine, because the surplus iron can often simply be removed.
2. Sources & Routes of Exposure
Iron reaches the body almost entirely by mouth. There is no meaningful inhaled or skin route for the conditions covered here (unlike many heavy metals). The question that matters is not whether you take in iron — everyone does — but how much, how fast, and whether the body’s normal “absorb less when stores are full” safety valve is working.
Dietary iron: heme and non-heme
Food iron comes in two forms. Heme iron (red meat, organ meats, seafood) is efficiently absorbed, around 15–35%. Non-heme iron (plants, grains, beans, fortified foods) is absorbed far less well, typically 2–20%, and its uptake is swayed by other foods — vitamin C boosts it, while tea, coffee, and calcium suppress it. A normal mixed diet delivers perhaps 10–20 mg a day, of which a healthy adult absorbs only about 1–2 mg. In hereditary hemochromatosis that careful brake is broken, so each day a little extra slips through — adding up to grams of stored iron over decades.
Supplements and the acute-poisoning hazard
The single most dangerous source of iron is the supplement bottle. What matters for poisoning is the amount of elemental iron, not the weight of the whole tablet. A 325 mg ferrous sulfate tablet contains about 65 mg of elemental iron (roughly 20% by weight); ferrous fumarate is about 33% elemental iron, ferrous gluconate about 12%. A toddler who swallows a handful of an adult’s prenatal vitamins can cross from a harmless dose into a lethal one in a single sitting — the reason iron supplements carry pediatric-poisoning warnings and child-resistant caps.
Transfusions and iron-loading anemias
Each unit of transfused red cells delivers roughly 200–250 mg of iron — more than a hundred days of normal dietary absorption, all at once. Because the body cannot excrete it, people who depend on regular transfusions accumulate iron relentlessly; clinically important overload typically appears after roughly 10–20 units. Separately, in some anemias the bone marrow is so overactive yet ineffective that it signals the gut to over-absorb iron even without any transfusion — iron-loading anemia.
Other and historical sources
Cast-iron cookware adds a small, generally beneficial amount of iron to food. A historical curiosity, “African iron overload,” was once linked to beer fermented in iron drums and is now understood to involve both the dietary load and genetic susceptibility. High-dose vitamin C is an indirect contributor: it sharply increases non-heme iron absorption and mobilizes stored iron, which is why people with overload are told to avoid high-dose vitamin C supplements.
3. Toxicokinetics
To understand iron overload you have to understand a master switch hormone called hepcidin, made by the liver. Hepcidin is the body’s thermostat for iron. When stores are high, the liver makes more hepcidin, which shuts the gut’s iron “export door” (a protein called ferroportin) and locks iron inside cells — absorption falls. When stores are low or the marrow is hungry for iron, hepcidin drops, ferroportin opens, and more iron enters the blood. This single feedback loop explains most of what goes right — and wrong — in iron handling.
How the body normally keeps iron safe
Absorbed iron is loaded onto a blood carrier protein called transferrin, which delivers it to the marrow, liver, and other tissues. Inside cells, iron not in immediate use is locked away in ferritin, a hollow protein shell that holds it in a chemically inert form. As long as iron stays bound to transferrin and ferritin, it is essentially harmless. The danger begins only when these safe-storage systems are saturated.
What goes wrong in hereditary hemochromatosis
In the common HFE-related form, the faulty gene leaves the liver unable to raise hepcidin properly. With the thermostat stuck low, the gut keeps absorbing iron as if the body were always deficient, and over years blood transferrin becomes increasingly saturated. Once transferrin is full, a toxic fraction called non-transferrin-bound iron (NTBI) appears in the circulation. NTBI is taken up greedily and uncontrollably by the liver, heart, and endocrine glands — precisely the organs that suffer in hemochromatosis — and because it is not safely chaperoned, it is the form that drives oxidative injury.
The kinetics of acute poisoning
A massive single dose overwhelms the system in hours, not years. Iron is directly corrosive to the gut lining, causing the early bleeding and vomiting. Absorbed iron quickly saturates transferrin, and the excess circulates as free, reactive iron that floods the liver and other organs. Because there is no rapid excretion route, the body cannot dump the surplus — the only fast way to remove it medically is a chelating drug that grabs free iron so the kidneys can flush it out. That is the core reason acute poisoning is so dangerous: a lot of toxic iron, nowhere for it to go.
Why men and women differ
Menstruation and pregnancy cause regular iron loss, which partly protects pre-menopausal women from hemochromatosis. As a result, men with the same genetic risk typically develop symptoms a decade or more earlier than women, who often do not present until after menopause. This is one of the clearest examples in medicine of how routine physiological blood loss can be protective.
4. Mechanism of Toxicity
Iron’s usefulness and its danger come from the same property: it readily flips between two chemical states, ferrous (Fe2+) and ferric (Fe3+), gaining and losing an electron. That electron-shuffling is what lets iron carry oxygen and run enzymes — but unleashed, the very same chemistry tears cells apart.
The Fenton reaction and reactive oxygen species
When free iron meets hydrogen peroxide — a normal byproduct of metabolism — it drives the Fenton reaction, producing the hydroxyl radical, one of the most destructive reactive oxygen species known. Unlike many free radicals the body neutralizes routinely, the hydroxyl radical reacts almost instantly with whatever it touches, and there is no specific enzyme to mop it up. In a healthy person this is harmless, because almost all iron is safely bound; the Fenton reaction only runs out of control once transferrin and ferritin are saturated and free iron is loose.
Lipid peroxidation and ferroptosis
The hydroxyl radical attacks the fatty membranes wrapping every cell and organelle, setting off a chain reaction called lipid peroxidation — one damaged fat molecule corrupts its neighbor, and the damage spreads like a spark along a fuse. The membrane loses integrity, internal machinery leaks, and the cell can die. Scientists now recognize a specific form of iron-driven cell death, ferroptosis, in which iron-dependent lipid peroxidation is the lethal event — helping explain why overload damages tissues steadily even without obvious inflammation or infection.
Fibrosis: how slow injury becomes scarring
In chronic overload the damage is gradual but relentless. As liver cells are repeatedly injured by oxidative stress, the liver’s repair cells (hepatic stellate cells) activate and lay down collagen scar tissue. Over years this progresses to fibrosis and finally cirrhosis. Iron also appears to promote cancer-causing DNA damage, which is why a cirrhotic, iron-loaded liver carries a markedly increased risk of hepatocellular carcinoma (primary liver cancer). The same oxidative-and-scarring process plays out in heart muscle and the pancreas, with different visible consequences.
Why some organs and not others
Iron does not deposit evenly. The organs that take up the most non-transferrin-bound iron — the liver, heart, pancreatic islet cells, anterior pituitary, and certain joints — are the ones that fail. Tissues with limited ability to repair, such as heart muscle and the insulin-producing beta cells of the pancreas, are especially vulnerable, which is why cardiomyopathy and diabetes are such characteristic complications.
5. Symptoms & Health Effects
The symptoms of iron overload depend entirely on which of the three entities is at work. Chronic hemochromatosis damages organs silently over decades; acute poisoning unfolds over hours to days in five recognizable stages. Both are detailed below.
Chronic hemochromatosis: an organ-by-organ tour
The early symptoms are frustratingly vague — fatigue, weakness, joint aches, low mood, loss of sex drive — which is exactly why hemochromatosis is so often missed until middle age. As iron accumulates, specific organ damage emerges:
- Liver. The liver is usually the first and most heavily loaded organ. Early on, the liver may simply be enlarged; over time, iron drives fibrosis and then cirrhosis. A cirrhotic, iron-loaded liver carries a substantially increased risk of hepatocellular carcinoma. Abnormal liver enzymes on a routine blood test are a common first clue. See also our overview of liver disease.
- Heart. Iron in the heart muscle causes cardiomyopathy — the heart may become dilated and weak (poor pumping) or stiff and restrictive (poor filling) — and disturbs the heart’s electrical system, producing arrhythmias and palpitations. Heart failure from iron overload can be reversible if iron is removed early, which makes recognizing it crucial.
- Pancreas — “bronze diabetes.” Iron deposited in the insulin-producing beta cells impairs insulin output, causing diabetes. Combined with the characteristic slate-grey or bronze skin tone (from iron-stimulated melanin and iron deposition in the skin), the classic pairing earned the historical name bronze diabetes. The skin discoloration is often most visible on sun-exposed areas.
- Pituitary and gonads. Iron in the anterior pituitary blunts the hormone signals that drive the sex glands, causing hypogonadism: in men, low libido, erectile dysfunction (impotence), and shrinking of the testes; in women, irregular or absent periods and early menopause. Loss of libido is frequently one of the earliest symptoms, though patients rarely volunteer it.
- Joints. Iron arthropathy classically affects the second and third metacarpophalangeal joints — the “knuckle” joints of the index and middle fingers — producing a distinctive ache and stiffness sometimes called the “iron fist” handshake sign. Larger joints (hips, knees) can also be affected, and the joint damage, unlike most other complications, often does not reverse with iron removal.
Men typically present earlier than women because menstrual blood loss is protective, and the disease is often clinically silent until the 40s or 50s, by which point years of iron loading have already occurred. This is why family screening matters so much — a relative may be detected and treated before any organ damage.
Acute iron poisoning: the five classic stages
Acute poisoning follows a textbook sequence. The danger is that the deceptive second stage can fool both patient and clinician into a false sense of security:
- Stage 1 — Gastrointestinal (about 0.5 to 6 hours). Iron is directly corrosive to the gut. The first signs are vomiting, abdominal pain, and diarrhea — classically with hematemesis (vomiting blood) and bloody, dark stools from gut bleeding. Severe fluid loss in this stage can itself cause shock. A child who swallowed iron and is not vomiting within six hours is unlikely to have taken a serious dose.
- Stage 2 — Latent or “deceptive recovery” (about 6 to 24 hours). The GI symptoms ease and the patient appears to improve. This apparent recovery is dangerous and misleading: iron is being absorbed and silently distributed to the organs while the patient looks better. Serious poisonings should be observed in hospital through this window, not sent home.
- Stage 3 — Shock and metabolic acidosis (roughly 6 to 48 hours). Free iron now causes circulatory collapse (shock), and a characteristic high–anion-gap metabolic acidosis develops as iron poisons cellular energy production and lactic acid builds up. Hepatotoxicity (liver injury) begins. This is the stage where untreated patients deteriorate rapidly.
- Stage 4 — Fulminant hepatic failure (about 2 to 3 days). Massive iron uptake by the liver can cause acute liver failure — jaundice, bleeding from clotting failure, confusion, and low blood sugar. Hepatic failure is a leading cause of death in serious iron poisoning.
- Stage 5 — Late gastrointestinal scarring (about 2 to 6 weeks). Survivors of the corrosive early injury can develop scar tissue in the stomach and intestine, leading to strictures and gastric outlet obstruction — narrowing that blocks the passage of food and may require surgery.
Estimating severity by dose
Risk in acute poisoning tracks the amount of elemental iron swallowed, judged against body weight:
- Less than 20 mg/kg — usually no symptoms or only mild GI upset.
- 20–60 mg/kg — moderate toxicity expected; medical assessment is warranted.
- Greater than 60 mg/kg — potentially severe to lethal; this is a true emergency requiring hospital care.
To make these numbers concrete: a 12 kg toddler reaches the potentially lethal 60 mg/kg threshold at roughly 720 mg of elemental iron — only about eleven 325 mg ferrous sulfate tablets. This is why a spilled bottle of adult iron pills is a genuine pediatric emergency.
Secondary (transfusional) overload
The organ damage in transfusional overload mirrors hemochromatosis — liver fibrosis, cardiomyopathy, diabetes, and endocrine failure — but the heart is often the organ that determines survival in transfusion-dependent patients, and iron-related cardiomyopathy was historically the leading cause of death in beta-thalassemia major before effective iron chelation became standard. Because the underlying anemia is incurable in many cases, the iron load is ongoing and must be managed for life.
6. Diagnosis & Laboratory Testing
Diagnosing iron overload is one of the success stories of modern laboratory medicine: a couple of inexpensive blood tests can raise the alarm, a genetic test can confirm the most common cause, and an MRI scan can measure organ iron without a biopsy. The tests differ sharply between the slow chronic forms and the acute emergency, so they are presented separately. (Our Lab Tests section explains many of these markers in more depth.)
Chronic overload: the first-line blood tests
- Serum ferritin reflects the body’s total iron stores: the higher it climbs, the more iron is stored. In adults, ferritin is usually reported in micrograms per liter (µg/L, equivalent to ng/mL). Values above about 200 µg/L in women and 300 µg/L in men prompt a look for overload, and markedly elevated levels (often >1000 µg/L) raise concern for organ damage. The crucial caveat: ferritin is also an acute-phase reactant, meaning it rises with infection, inflammation, liver injury, alcohol, and obesity. A high ferritin alone does not prove iron overload — it must be interpreted alongside transferrin saturation.
- Transferrin saturation is the most specific early screen for hereditary hemochromatosis. It is the percentage of the blood’s iron-carrying capacity that is actually filled with iron, calculated from serum iron and total iron-binding capacity. Measured fasting, a transferrin saturation above 45% raises suspicion of hemochromatosis; it is a highly sensitive marker and often becomes abnormal before ferritin does. Very high saturations (>60% in men, >50% in women) are strongly suggestive.
Confirming the cause: HFE genetic testing
When the blood tests suggest overload, HFE genotyping looks for the responsible mutations. The classic genetic diagnosis is C282Y homozygosity — two copies of the C282Y variant — which accounts for the great majority of hereditary hemochromatosis in people of Northern European ancestry. A second variant, H63D, is much less likely to cause clinical overload on its own; the “compound heterozygote” (one C282Y and one H63D) sometimes loads iron but is far less penetrant. An important nuance is that not everyone with two C282Y copies develops disease — penetrance is incomplete, especially in women — so genetics is interpreted together with the iron studies, not in isolation. Genetic confirmation also enables family screening of first-degree relatives.
Measuring organ iron: MRI and biopsy
Once overload is established, the next question is how much iron is in the organs. Liver MRI using R2* or T2* relaxometry (commercial methods include FerriScan) can quantify liver iron concentration non-invasively, replacing the liver biopsy that was once routine. Crucially, dedicated cardiac MRI (T2*) can measure heart iron, which does not always track with liver iron — a patient can have a dangerously iron-loaded heart with only modest liver loading, so the heart must be assessed in its own right, especially in transfusional overload. Liver biopsy is now reserved for selected cases — for example, to stage fibrosis or measure the hepatic iron concentration and hepatic iron index directly when imaging and genetics leave the picture unclear.
Acute iron poisoning: a different toolkit
In the emergency setting, ferritin and genetics are irrelevant; the tests are aimed at gauging how much iron was absorbed and how sick the patient is:
- Serum iron level. Measured in micrograms per deciliter (µg/dL), this is the key number, drawn to catch the peak roughly 4 to 6 hours after ingestion (later for extended-release products). As a rough guide, peak levels above about 350 µg/dL predict systemic toxicity, and levels above 500 µg/dL indicate severe poisoning with risk of shock and liver failure. A normal serum iron must be timed correctly to be reassuring, because a level drawn too early or too late can be falsely low.
- Venous blood gas and lactate. These detect the high–anion-gap metabolic acidosis of stage 3 and track its severity; a worsening acidosis signals systemic iron toxicity.
- Abdominal X-ray. Some iron tablets are radiopaque and show up as bright pills on a plain abdominal radiograph, confirming ingestion and revealing pills still in the gut that may need to be cleared. A negative X-ray does not rule out poisoning, however, because many liquid and chewable iron preparations are not radiopaque.
- Supporting labs. Glucose, white blood cell count, liver enzymes, kidney function, and clotting studies all help judge severity — high glucose and a high white-cell count have historically been associated with significant iron ingestion, and rising liver enzymes flag developing hepatotoxicity.
7. Treatment & Management
Iron overload is, unusually, one of the most treatable causes of organ damage in medicine — the surplus iron can often simply be removed. The right method depends entirely on which entity is being treated.
Hereditary hemochromatosis: phlebotomy first
The cornerstone treatment is therapeutic phlebotomy — the same procedure as donating blood. Because each unit of blood removed carries away roughly 200–250 mg of iron locked in its hemoglobin, regularly removing blood forces the body to draw down its iron stores to make new red cells. A typical induction schedule removes one unit weekly or twice weekly until ferritin and transferrin saturation fall into the target range, followed by lifelong maintenance phlebotomy every few months to keep iron from re-accumulating. Phlebotomy is cheap, effective, and — if started before cirrhosis or diabetes develop — can give a person with hemochromatosis a normal life expectancy. Fatigue, skin color, and early heart and liver changes often improve; established cirrhosis and joint damage usually do not reverse, which is the argument for early diagnosis.
When phlebotomy is not feasible — for instance in someone who is also anemic and cannot spare the blood — iron chelation drugs (deferasirox, deferoxamine, or deferiprone) are used instead. These bind iron and let the body excrete it.
Lifestyle and dietary measures
People with hemochromatosis are advised to:
- Avoid iron supplements and iron-fortified products, and avoid high-dose vitamin C supplements, which increase iron absorption and mobilize stored iron (see Vitamin C).
- Limit alcohol, which compounds iron’s toxicity to the liver and accelerates progression to cirrhosis.
- Moderate red and organ meat, the richest sources of well-absorbed heme iron, though diet alone cannot substitute for phlebotomy.
- Avoid raw shellfish. This is a specific, life-saving precaution: iron-overloaded people are dangerously susceptible to Vibrio vulnificus, a bacterium in raw oysters and seafood that thrives on excess iron and can cause fatal bloodstream infection.
Acute iron poisoning: an emergency protocol
Acute poisoning is managed in a hospital, ideally with poison-control input, and care escalates with severity:
- Decontamination. Activated charcoal does not bind iron and is unhelpful. When radiopaque tablets are seen on X-ray, whole-bowel irrigation — flushing the gut with a polyethylene glycol solution — can sweep pills through before more iron is absorbed.
- Chelation with intravenous deferoxamine. This is the antidote for serious poisoning. Deferoxamine binds free iron to form a complex the kidneys excrete, classically turning the urine a brick-red or “vin rosé” color — a visible sign that the drug is removing iron. It is given for severe symptoms, shock, acidosis, or a serum iron above roughly 500 µg/dL.
- Aggressive supportive care in an intensive-care setting — intravenous fluids for shock, correction of acidosis, blood products for bleeding, and support for failing liver and kidneys. In the most severe cases, liver transplantation has been used for fulminant hepatic failure.
Transfusional overload: lifelong chelation
People with transfusion-dependent anemias cannot be treated by phlebotomy — they are already anemic — so the mainstay is ongoing iron chelation therapy. Oral agents (deferasirox, deferiprone) and the older infused agent (deferoxamine) are matched to the patient and to where the iron has deposited; deferiprone, for instance, is particularly good at removing iron from the heart. Treatment is guided by serial ferritin and by liver and cardiac MRI, and it continues for as long as transfusions do. The advent of effective chelation transformed beta-thalassemia major from a disease that killed in adolescence into one compatible with decades of life.
8. Prevention & Risk Reduction
Prevention looks different for each entity — you cannot prevent the genes you inherit, but you can catch genetic overload early; you can almost entirely prevent childhood poisoning with simple safety steps; and you can anticipate transfusional overload before it harms organs.
Catching hereditary hemochromatosis early
Because hemochromatosis is silent for years yet fully treatable, early detection is the whole game. The key opportunities are:
- Family screening. When one person is diagnosed with C282Y homozygosity, first-degree relatives (parents, siblings, children) should be offered transferrin saturation, ferritin, and HFE testing. A relative caught and treated before any organ loads with iron can avoid the disease entirely — this is among the highest-value screening in all of medicine.
- Acting on incidental clues. An unexplained high ferritin or transferrin saturation, abnormal liver tests, early arthritis of the index- and middle-finger knuckles, unexplained diabetes with a bronze complexion, or unexplained cardiomyopathy should all prompt iron studies.
- Avoiding iron and high-dose vitamin C supplements in anyone known to be at genetic risk, even before iron has accumulated.
Preventing childhood iron poisoning
Acute pediatric iron poisoning is almost entirely preventable. Public-health measures — child-resistant packaging, unit-dose blister packs for high-strength iron, and pediatric warning labels — have substantially reduced deaths since the 1990s. At home:
- Store iron supplements and prenatal vitamins locked away and out of children’s reach, in their original child-resistant containers.
- Remember that prenatal vitamins, common in households with a new baby, are a frequent culprit because they are high-dose and often left on a nightstand.
- If a child may have swallowed iron, contact a poison-control center immediately — even if the child seems well, because of the deceptive latent stage. In the United States, the Poison Help line is 1-800-222-1222.
Anticipating transfusional overload
For people who will need long-term transfusions, overload is predictable, so it is monitored from the outset. Ferritin is tracked, and liver and cardiac MRI are used to measure organ iron before damage occurs, with chelation started at the appropriate threshold (often after roughly 10–20 transfusions or once ferritin rises persistently). Anticipatory monitoring — rather than waiting for symptoms — is what prevents the heart and liver complications that once shortened these patients’ lives.
A note on the general public
For most healthy adults, ordinary dietary iron poses no overload risk — the hepcidin thermostat handles it. The sensible precaution is simply not to take iron supplements without a medical reason: iron treats a documented deficiency, not a routine “tonic.” Anyone considering long-term supplementation should have their iron status checked first.
9. Related Topics
- Iron (essential) — the companion page on iron as a vital nutrient: deficiency, anemia, and how much we actually need.
- Heavy Metals — overview of toxic metals and how their poisoning differs from iron overload.
- Manganism — another essential mineral that becomes neurotoxic in excess.
- Cirrhosis — the liver scarring that untreated iron overload can cause.
- Liver Disease — broader context for the hepatic complications of overload.
- Cardiomyopathy — iron-loaded heart muscle and its consequences.
- Diabetes — the “bronze diabetes” of pancreatic iron deposition.
- Anemia — the iron-loading and transfusion-dependent anemias behind secondary overload.
- Vitamin C — why high-dose vitamin C is discouraged in iron overload.
- Lab Tests — ferritin, transferrin saturation, and the other markers used to diagnose overload.
10. Key Research Papers
- Fleming RE, Ponka P. Iron Overload in Human Disease. New England Journal of Medicine. 2012;366(4):348–359. doi:10.1056/NEJMra1004967
- Powell LW, Seckington RC, Deugnier Y. Haemochromatosis. The Lancet. 2016;388(10045):706–716. doi:10.1016/S0140-6736(15)01315-X
- Bacon BR, Adams PC, Kowdley KV, Powell LW, Tavill AS. Diagnosis and management of hemochromatosis: 2011 Practice Guideline by the American Association for the Study of Liver Diseases. Hepatology. 2011;54(1):328–343. doi:10.1002/hep.24330
- European Association for the Study of the Liver. EASL clinical practice guidelines for HFE hemochromatosis. Journal of Hepatology. 2010;53(1):3–22. doi:10.1016/j.jhep.2010.03.001
- Andrews NC. Disorders of Iron Metabolism. New England Journal of Medicine. 1999;341(26):1986–1995. doi:10.1056/NEJM199912233412607
- Camaschella C, Nai A, Silvestri L. Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica. 2020;105(2):260–272. doi:10.3324/haematol.2019.232124
- Ganz T. Hepcidin and iron regulation, 10 years later. Blood. 2011;117(17):4425–4433. doi:10.1182/blood-2011-01-258467
- Wang C-Y, Babitt JL. Liver iron sensing and body iron homeostasis. Blood. 2019;133(1):18–29. doi:10.1182/blood-2018-06-815894
- Marsella M, Borgna-Pignatti C. Transfusional Iron Overload and Iron Chelation Therapy in Thalassemia Major and Sickle Cell Disease. Hematology/Oncology Clinics of North America. 2014;28(4):703–727. doi:10.1016/j.hoc.2014.04.004
- Ganz T. Anemia of Inflammation (ferritin as an acute-phase reactant). New England Journal of Medicine. 2019;381(12):1148–1157. doi:10.1056/NEJMra1804281
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Hemochromatosis. U.S. National Institutes of Health. niddk.nih.gov
- MedlinePlus. Hemochromatosis. U.S. National Library of Medicine. medlineplus.gov
- MedlinePlus Medical Encyclopedia. Iron overdose. U.S. National Library of Medicine. medlineplus.gov
- Office of Dietary Supplements (ODS). Iron — Health Professional Fact Sheet. U.S. National Institutes of Health. ods.od.nih.gov
Connections
- Iron (essential)
- Manganism
- Heavy Metals
- Lead
- Cadmium
- Copper
- Zinc
- Manganese
- Vitamin C
- Cirrhosis
- Liver Disease
- Cardiomyopathy
- Diabetes
- Anemia
- Lab Tests
- All Minerals
- Hemochromatosis — the inherited disorder behind most primary iron overload.