Strontium Deficiency: What the Evidence Shows
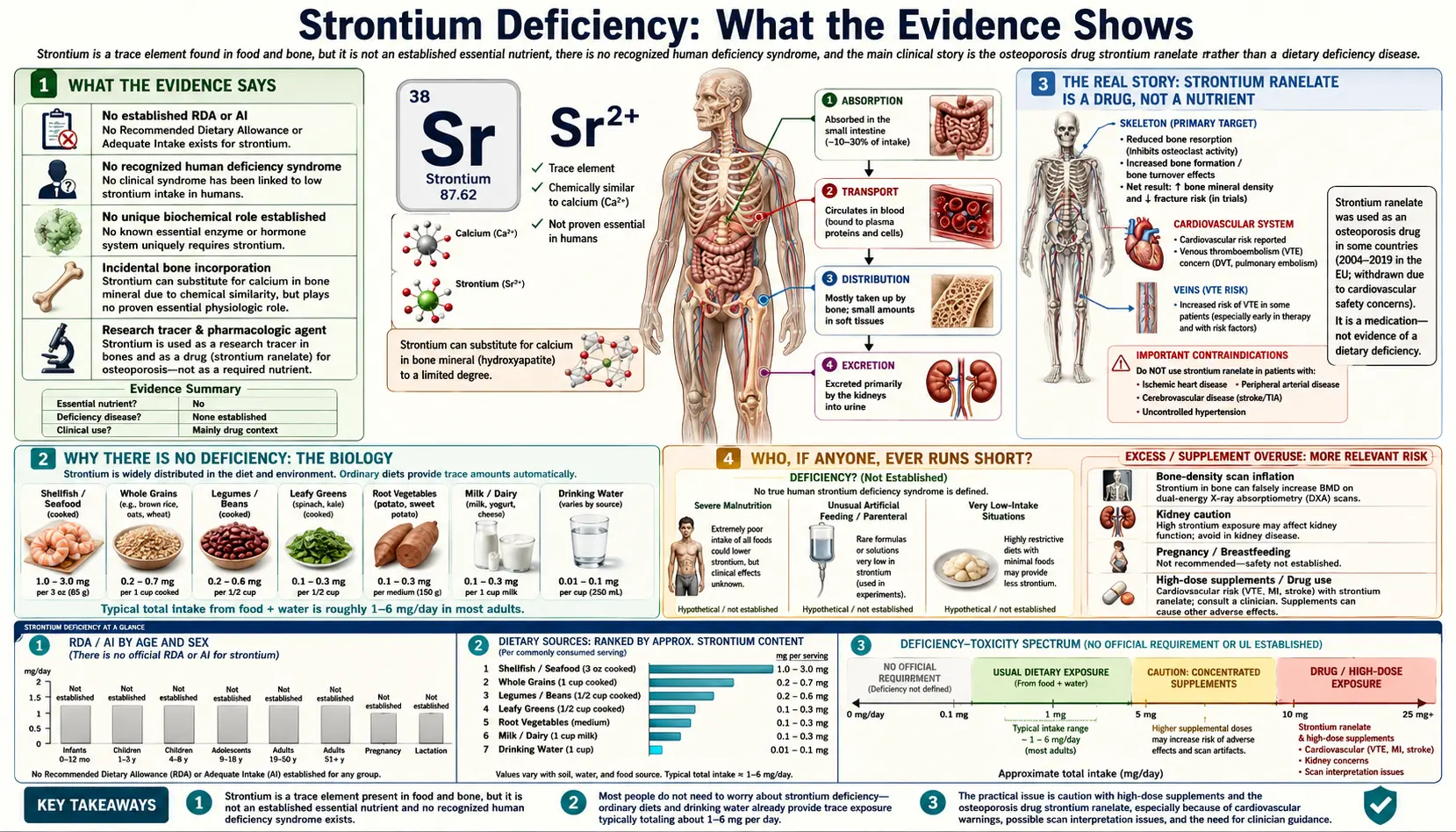
Here is the honest bottom line, stated plainly so you can stop worrying about it: there is no such thing as strontium deficiency in humans. Strontium is not an essential nutrient — your body has no known job that requires it, there is no recommended intake, no blood test that defines a "low" level, and no recognized deficiency disease. You will never be told you are "low in strontium," because the concept does not exist in medicine. The reason strontium comes up at all in bone-health conversations is something different and easily confused with a nutrient story: a prescription drug called strontium ranelate, which delivers a pharmacological — that is, drug-sized, far above dietary — dose of strontium and was studied for osteoporosis. That drug is not a vitamin you are missing; it is a medication with real benefits in fracture studies and real safety limits (including a heart-attack signal) that led regulators to restrict it. This page exists to set the record straight: to explain why there is no deficiency to correct, what the everyday trace of strontium in your food and bones actually is, who (if anyone) ever runs genuinely short, and what the sensible, low-key thing to do is — which, for almost everyone, is nothing.
Table of Contents
- What the Evidence Says
- Why There Is No Deficiency: The Biology
- The Real Story: Strontium Ranelate Is a Drug, Not a Nutrient
- Who, If Anyone, Ever Runs Short
- Is There a Test for “Low Strontium”?
- What to Do (Almost Always: Nothing Special)
- When to Talk to a Doctor
- Related Nutrients and Pages
- Key Research Papers
- Connections
- Featured Videos
What the Evidence Says
Let us be candid, because vague language is exactly how supplement marketing slips an "essential" claim past you. Strontium is not classified as an essential element for humans. An essential nutrient is one your body genuinely needs — remove it from the diet and a specific, reproducible deficiency disease appears (think scurvy from missing vitamin C, or rickets from missing vitamin D). Strontium fails that test on every count:
- There is no recognized human deficiency syndrome. No cluster of symptoms, no disease, no condition has ever been shown to result from getting "too little" strontium. You cannot be diagnosed with strontium deficiency because the diagnosis does not exist.
- There is no Recommended Dietary Allowance (RDA), no Adequate Intake (AI), and no Dietary Reference Intake of any kind. The bodies that set nutrient requirements have not established one for strontium, precisely because no requirement has been demonstrated.
- There is no defined biochemical role. Strontium is not a known cofactor for any enzyme, not a structural requirement for any tissue, and not part of any hormone or signaling pathway your body must run. Whatever strontium ends up in your bones gets there because it chemically resembles calcium and tags along — not because the bone needs it.
- Everyone already has some, with no effort. Strontium is a common element in soil, water, and food, so it is ubiquitous in the diet at trace levels. Typical intakes run on the order of a couple of milligrams a day, and a small fraction of that settles into the skeleton over a lifetime. There is simply no dietary scenario in which a person eating ordinary food runs out.
You may have seen strontium described, in older or speculative writing, as a "possibly beneficial ultratrace element." That phrasing reflects laboratory and animal observations that strontium can interact with bone tissue — not evidence that humans require it or that a deficiency state exists. Reviews of strontium biology are clear on the distinction: strontium's effects on bone are interesting and even useful pharmacologically, but they do not make it a dietary essential, and no human deficiency has been described (Pors Nielsen, 2004). It is correct, and genuinely useful to you, for this page to say so directly rather than manufacture a problem.
If a product or article is trying to sell you on "correcting a strontium deficiency," that is a red flag in itself: it is asserting a condition that medicine does not recognize.
Why There Is No Deficiency: The Biology
To understand why you can't be deficient in strontium, it helps to know what strontium is and how it behaves in the body. Strontium (chemical symbol Sr) sits directly below calcium on the periodic table, which is the whole key to the story. Elements in the same column behave chemically alike, and to your body's bone-building machinery, strontium looks like a slightly heavier, slightly clumsier version of calcium.
Here is a useful analogy. Imagine your skeleton is built from a specific brand of brick — calcium. Strontium is a near-identical brick from a different factory: it fits in the same slots, so when it happens to be lying around, the masons (your bone cells) will occasionally lay one into the wall. But the building was never designed for the substitute brick, the supply of real calcium bricks is what the plans call for, and the structure does not depend on the substitute being present at all. That is why strontium accumulates in bone — it gets incorporated into the mineral crystal alongside calcium — without ever being something the bone requires. About 99% of the body's strontium ends up in the skeleton and teeth, riding along the same handling pathways the body uses for calcium (Pors Nielsen, 2004).
Two consequences follow directly, and together they explain the absence of any deficiency:
- Nothing in your physiology is waiting on strontium. Because strontium has no dedicated function — no enzyme that needs it, no process that stalls without it — removing it would not break anything. A deficiency only exists when a missing ingredient causes a malfunction. With strontium there is no machine to jam.
- Calcium does all the actual structural work. The mineral your bones genuinely depend on is calcium, partnered with phosphate, and supported by vitamin D (which controls calcium absorption) and vitamin K2 (which helps direct calcium into bone). Strontium is, at most, a passenger in that system. So the meaningful question for bone is never "am I getting enough strontium?" but "am I getting enough calcium, vitamin D, and the rest of the bone-supporting nutrients?" — see the Calcium overview and the osteoporosis nutrition page on Calcium, Vitamin D, and Protein Intake.
There is one more reason a "low strontium" worry makes no biological sense: because strontium and calcium share the same transport machinery, your strontium status simply tracks your calcium intake and your environment. If you eat and drink normally, you take in strontium automatically; the body neither hoards it as if it were precious nor suffers when intake is modest. It is along for the ride.
The Real Story: Strontium Ranelate Is a Drug, Not a Nutrient
Almost all genuine medical interest in strontium traces to one thing, and it is essential to separate it from any nutrient idea: strontium ranelate, a prescription medication once used for severe osteoporosis. This is the single biggest source of confusion, because it lets supplement sellers borrow the credibility of real fracture trials and quietly imply that your body needs strontium. It does not. Here is the honest picture.
It is a drug-sized dose, far above anything dietary. Strontium ranelate delivered roughly 680 mg of elemental strontium per day — hundreds of times the few milligrams you get from food. At that pharmacological dose, strontium stops being a passive passenger and starts actively influencing bone cells. Laboratory work suggests it does two things at once: it modestly nudges bone-building cells (osteoblasts) to do more, while restraining bone-removing cells (osteoclasts) — a "dual action" that, on paper, tips the balance toward bone formation (Marie, 2006). This is a drug effect at a drug dose, not evidence of a nutrient your diet is short on.
The fracture trials were real. In large randomized, placebo-controlled trials in postmenopausal women with osteoporosis, strontium ranelate reduced fractures. The SOTI trial showed a reduction in new vertebral (spine) fractures over three years (Meunier et al., 2004), and the TROPOS trial showed a reduction in nonvertebral fractures, including a benefit in hip-fracture risk among higher-risk women (Reginster et al., 2005). Earlier dose-finding work had already pointed to these effects (Meunier et al., 2002). So the benefit was not imaginary.
But the bone-density numbers were partly an illusion — and the safety record forced a retreat. Two cautions matter enormously and are exactly what marketing leaves out:
- Inflated DEXA readings. Because strontium is a heavier atom than calcium, it absorbs X-rays more strongly. When it deposits in bone, a DEXA bone-density scan reads higher — partly because of the strontium itself, not purely because there is more real bone. A large share of the apparent "bone density gain" on these scans was an artifact of the strontium atom, which is why fracture outcomes, not density numbers, are the honest measure of any bone drug.
- A cardiovascular safety signal. Pooled analyses of the trials found an increased risk of heart attack (myocardial infarction) and other cardiovascular events in people taking strontium ranelate. A nationwide registry study likewise examined cardiovascular outcomes in treated patients (Abrahamsen et al., 2013). On the strength of this signal, the European Medicines Agency restricted the drug to severe osteoporosis in patients who could not use other treatments and who had no history of heart or circulatory disease — and the manufacturer ultimately withdrew it from the market. It is not a current first-line osteoporosis therapy.
The takeaway is the heart of this page: the strontium ranelate story is a pharmacology story with genuine benefits and genuine risks at a high dose — it is not, and was never, evidence that ordinary people are "deficient" in strontium or need to supplement it. Over-the-counter "strontium for bones" products (often strontium citrate) are sometimes marketed by leaning on the ranelate trials, but they are not the studied drug, are not regulated as a medicine, will still inflate your DEXA reading (potentially misleading you and your doctor), and carry the same unresolved cardiovascular question without the trial oversight. For the full evidence review, see the main Strontium for Bone Health page; for what actually works for bones, see Osteoporosis and its treatment deep-dives.
Who, If Anyone, Ever Runs Short
Because strontium is not essential, "running short" is not a meaningful clinical event — there is no function to lose. The honest answer to "who is deficient?" is "no one, in any way that matters." But to be thorough and to address the edge cases people sometimes ask about, here is where unusually low strontium exposure can occur, and why none of it amounts to a deficiency requiring treatment:
- Total parenteral nutrition (TPN). People fed entirely by vein receive carefully formulated solutions. Strontium is not a required additive because it is not an essential element, so long-term TPN can result in very low strontium intake — with no observed deficiency consequence. This is the clearest demonstration that the body does fine without dietary strontium.
- Very low-mineral diets or distilled-water environments. Since much dietary strontium rides along with calcium-containing foods and mineral-containing water, an extremely restricted diet lowers strontium intake too. Again, no deficiency state results — the relevant risk in such diets is inadequate calcium, vitamin D, and other genuine nutrients, not strontium.
- Geographic and dietary variation. Strontium content in food and water varies a great deal by region and soil. This produces a wide normal range of body strontium across populations with no corresponding "deficiency" in low-strontium areas — further evidence that there is no threshold below which something goes wrong.
Notice the pattern: in every situation where strontium intake is low, the documented health concerns are about other nutrients (especially calcium and vitamin D) or about the underlying illness — never about the strontium itself. That is exactly what you would expect for a non-essential element.
Is There a Test for “Low Strontium”?
People sometimes ask whether a blood test or hair-mineral analysis can reveal a strontium deficiency. The candid answer is that there is no clinical test for strontium status, because there is no status to measure against. A few points worth knowing:
- No reference range exists. Standard panels such as the Comprehensive Metabolic Panel do not measure strontium at all — they track the electrolytes and minerals that genuinely matter clinically (sodium, potassium, calcium, and so on). Specialized labs can measure strontium in blood, urine, or bone, but these are used in research and in toxicology (for example, after industrial exposure or to study the bone of patients who took strontium ranelate), not to diagnose a deficiency.
- Hair and "intracellular mineral" tests are not validated for this. Reports that flag you as "low in strontium" from a hair analysis or similar test are not medically meaningful: there is no established healthy target, so a number cannot be "too low." Such results are sometimes used to justify selling supplements; treat them with skepticism.
- If strontium does show up in testing, the question is usually the opposite. Where strontium measurement matters clinically, the concern is typically excess exposure or interpreting bone scans in someone who has taken strontium — topics covered on the companion Strontium Toxicity page — not a shortfall.
What to Do (Almost Always: Nothing Special)
This is the practical, low-key part, and it is short by design. For the overwhelming majority of people, the correct action regarding "strontium deficiency" is to recognize that it isn't a thing and redirect that energy toward what genuinely protects bone.
- Do not supplement strontium to "prevent deficiency." There is no deficiency to prevent. Routine strontium supplements are not recommended for healthy people, they will distort any future DEXA scan, and they carry the unresolved cardiovascular question discussed above without the oversight of the original drug trials.
- Get the real bone nutrients instead. If bone health is your goal, the evidence points to adequate calcium (food first — dairy such as milk and yogurt, plus leafy greens and fortified foods), sufficient vitamin D, vitamin K2, adequate protein, and weight-bearing exercise. See Calcium, Vitamin D, and Protein Intake and Weight-Bearing and Resistance Exercise.
- Eat normally and the trace takes care of itself. An ordinary, varied diet supplies the small amount of strontium that ends up in your skeleton with no planning required. You do not need a "high-strontium" food list, and you do not need to track it.
- If you have osteoporosis, talk about proven treatments. Effective, well-studied options for fracture prevention — and how they are chosen — are covered on the Osteoporosis hub, including bisphosphonates and denosumab, romosozumab, and teriparatide. That conversation, not a strontium product, is the right path.
In short: there is nothing to correct, nothing to monitor, and nothing to buy. That is a good-news ending, not a gap in your care.
When to Talk to a Doctor
Because strontium deficiency is not a real condition, there are no "deficiency symptoms" to watch for. But the topics that bring people to this page — bone health and any use of strontium products — do have moments that warrant a conversation with a clinician. Reach out to your doctor if any of the following apply:
- You are taking, or considering, an over-the-counter strontium supplement. Mention it before your next bone-density scan, because strontium will inflate the reading and can mislead the interpretation of your bone health and your treatment decisions.
- You took strontium ranelate (or a strontium supplement) and have cardiovascular risk. Given the heart-attack signal that led regulators to restrict the drug, anyone with a history of heart disease, stroke, peripheral artery disease, or uncontrolled high blood pressure should discuss stopping strontium and review safer bone options.
- You have been told you have low bone density or have had a fragility fracture. This deserves a proper workup and an evidence-based treatment plan — see Osteoporosis — rather than self-treating with strontium.
- You suspect industrial or environmental strontium exposure (an occupational setting, contaminated water). That is a question of potential excess, covered on the Strontium Toxicity page, and worth raising with your doctor or an occupational-health specialist.
- A test labeled you “deficient” in strontium. Bring it in so a clinician can explain why that result is not clinically meaningful before you spend money acting on it.
For genuine, time-sensitive bone or fracture concerns, follow the guidance on the disease pages rather than anything on this nutrient-myth page.
Related Nutrients and Pages
Strontium's whole significance comes from its chemical kinship with calcium and its place in the bone-health conversation. These pages cover the things that actually matter for bone — and the other side of the strontium story:
- Calcium — the genuinely essential structural mineral of bone, and the element strontium imitates. Start here for real bone nutrition.
- Vitamin D — controls how much calcium you absorb; a true and common deficiency, unlike strontium.
- Vitamin K2 — helps direct calcium into bone rather than soft tissue.
- Magnesium — another essential mineral involved in bone and in calcium/vitamin D metabolism.
- Strontium Toxicity — the other leg of the strontium story: excess and exposure, which is where strontium measurement actually matters.
- Osteoporosis — the condition strontium ranelate was studied for, with evidence-based treatments that work.
Key Research Papers
- Pors Nielsen S (2004). The biological role of strontium. Bone;35(3):583-588. — DOI: 10.1016/j.bone.2004.04.026
- Meunier PJ, Roux C, Seeman E, Ortolani S, Badurski JE, et al. (2004). The effects of strontium ranelate on the risk of vertebral fracture in women with postmenopausal osteoporosis (SOTI). New England Journal of Medicine;350(5):459-468. — DOI: 10.1056/NEJMoa022436
- Reginster JY, Seeman E, De Vernejoul MC, Adami S, Compston J, et al. (2005). Strontium ranelate reduces the risk of nonvertebral fractures in postmenopausal women with osteoporosis: Treatment of Peripheral Osteoporosis (TROPOS) study. Journal of Clinical Endocrinology & Metabolism;90(5):2816-2822. — DOI: 10.1210/jc.2004-1774
- Meunier PJ, Slosman DO, Delmas PD, Sebert JL, Brandi ML, et al. (2002). Strontium ranelate: dose-dependent effects in established postmenopausal vertebral osteoporosis — a 2-year randomized placebo-controlled trial. Journal of Clinical Endocrinology & Metabolism;87(5):2060-2066. — DOI: 10.1210/jc.87.5.2060
- Marie PJ (2006). Strontium ranelate: a dual mode of action rebalancing bone turnover in favour of bone formation. Current Opinion in Rheumatology;18(Suppl 1):S11-S15. — DOI: 10.1097/01.bor.0000229522.89546.7b
- Abrahamsen B, Grove EL, Vestergaard P (2014). Nationwide registry-based analysis of cardiovascular risk factors and adverse outcomes in patients treated with strontium ranelate. Osteoporosis International;25(2):757-762. — DOI: 10.1007/s00198-013-2469-4
- European Medicines Agency / PRAC (2014). Recommendation to restrict the use of strontium ranelate (Protelos/Osseor) due to cardiovascular risk. EMA review. — PubMed (cardiovascular-safety literature)
- Strontium dietary intake and essentiality status in humans (no established requirement). — PubMed (intake & essentiality)
PubMed Topic Searches
- PubMed — Is strontium an essential element in human nutrition?
- PubMed — Strontium ranelate osteoporosis fracture trials
- PubMed — Strontium ranelate cardiovascular safety
- PubMed — Strontium and DEXA bone-density measurement artifact
- PubMed — Stable strontium, calcium, and bone metabolism
Connections
- Strontium for Bone Health (Overview)
- Strontium Toxicity
- Calcium
- Calcium Deficiency
- Magnesium
- Vitamin D3
- Vitamin K2
- Osteoporosis
- Calcium, Vitamin D, and Protein Intake
- DEXA Scan, T-Score, and Z-Score Explained
- Bisphosphonates for Osteoporosis
- Denosumab, Romosozumab, and Teriparatide
- Weight-Bearing and Resistance Exercise
- Comprehensive Metabolic Panel
- Milk
- Yogurt