Strontium for Bone Health: Evidence, Strontium Ranelate, and Safety
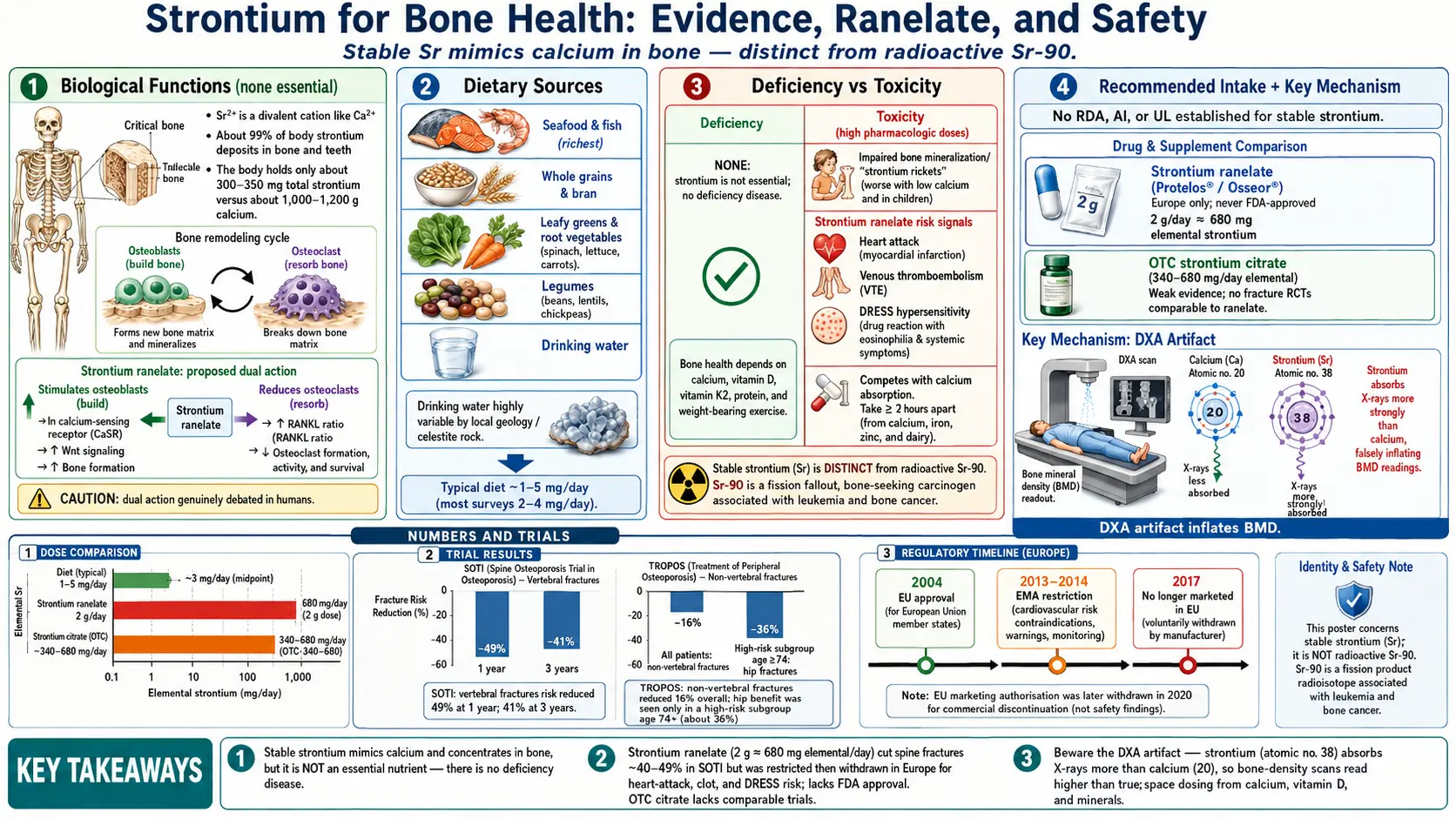
Table of Contents
- Overview
- Biological Functions
- Dietary Sources
- Deficiency
- Recommended Intake
- Supplementation & Forms
- Toxicity & Upper Limit
- Special Considerations
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Strontium (chemical symbol Sr, atomic number 38) is a soft, silvery metal that sits directly below calcium in the periodic table. Because it is a divalent cation with a similar size and charge to calcium (Ca2+), the human body cannot fully tell the two apart: it absorbs strontium through the same intestinal pathways, carries it in the blood, and deposits roughly 99% of body strontium in bone and teeth, exactly where it puts calcium. A healthy adult carries only about 300–350 mg of strontium in total — a tiny amount compared with the roughly 1,000–1,200 g of calcium in the skeleton.
This page is about stable (non-radioactive) strontium and its relationship to bone. That distinction matters enormously, because the word “strontium” is also attached to a notorious radioactive isotope, strontium-90 (Sr-90), a product of nuclear fission and atmospheric weapons-test fallout. Sr-90 is a bone-seeking carcinogen: it follows the same calcium-mimic route into the skeleton, where its radiation can damage bone marrow and raise the risk of leukemia and bone cancer. The natural, stable strontium found in food, water, and supplements is a completely different thing — it is not radioactive and does not emit ionizing radiation. The rest of this article concerns only stable strontium; Sr-90 is mentioned only to prevent confusion.
Interest in stable strontium for bone health comes from one main source: a prescription osteoporosis medicine called strontium ranelate (brands Protelos and Osseor), which was approved in Europe in 2004 and showed reduced fracture risk in postmenopausal women. That drug was never approved by the U.S. Food and Drug Administration (FDA), and it was later restricted and then discontinued because of safety concerns. Separately, over-the-counter (OTC) supplements containing strontium citrate are marketed for bones, but they are a different chemical salt with much weaker evidence. Understanding strontium honestly means keeping these three things — the element, the European drug, and the OTC supplement — clearly separate.
Why strontium is talked about at all
Strontium is not a vitamin or an essential mineral, and most clinicians never think about it. It enters health conversations almost entirely through osteoporosis: because it concentrates in bone and, at high doses, changes how bone is built and broken down, it can influence fracture risk and bone-density measurements. As the sections below explain, those effects are real but come with important caveats — including a measurement artifact that makes strontium look better on bone scans than it truly is.
2. Biological Functions
Strontium has no established essential biological function in humans. Unlike iron, zinc, iodine, or calcium, it is not a required cofactor for any enzyme, hormone, or structural protein, and no human metabolic pathway depends on it. The body tolerates and stores strontium simply because its chemistry is so close to calcium’s — not because it needs it. For that reason, the headings below describe what strontium does at the doses found in medicines and supplements, rather than a physiological “role” the body cannot do without.
Behaving like calcium in bone
Bone is constantly remodeled: cells called osteoclasts break down old bone (resorption), and cells called osteoblasts build new bone (formation). Strontium ions slot into the mineral lattice of bone in place of some calcium ions, and they accumulate especially in newly formed bone. At ordinary dietary levels this substitution is trivial. At the much higher doses used in strontium ranelate, laboratory and animal studies show that strontium can shift the balance of remodeling.
The proposed “dual action”
The most-discussed property of strontium ranelate is its claimed dual action on bone: stimulating osteoblasts to build more bone while reducing osteoclast activity so that less bone is broken down. In cell and animal models this dual effect is well documented and is thought to involve the calcium-sensing receptor and signaling pathways such as OPG/RANKL that govern osteoclast formation (Marie, 2006). If true in people, it would make strontium unusual, because most osteoporosis drugs either slow resorption (bisphosphonates, denosumab) or stimulate formation (teriparatide), but not both.
In humans, however, the “dual action” story is genuinely debated. Critics point out that markers of bone formation rise only modestly in patients, and that much of the apparent benefit on bone-density scans is a measurement artifact (see Section 7) rather than proof of vigorous new bone. So while strontium clearly influences bone biology at pharmacologic doses, the precise mechanism — and how much of the clinical benefit it explains — remains uncertain rather than settled.
3. Dietary Sources
Stable strontium is widespread in the environment and is present in the ordinary diet, though always in small amounts. Because plants take it up from soil and animals concentrate it in bone, strontium turns up across the food supply roughly in parallel with calcium. Typical total dietary intake is only a few milligrams per day — commonly estimated in the range of about 1–5 mg/day, with most surveys clustering near 2–4 mg/day, depending heavily on diet and local geology.
Common food and water sources
- Seafood and fish — among the richer dietary contributors, reflecting the strontium content of seawater.
- Whole grains and bran — wheat, oats, and other cereals.
- Leafy green and root vegetables — spinach, lettuce, carrots, and similar produce.
- Legumes — beans, peas, and lentils.
- Drinking water — an important and highly variable source. Strontium content depends on local geology; water from areas with strontium-bearing rock (such as celestine, strontium sulfate) carries more.
Why geology matters
Because so much dietary strontium comes through soil and water, intake can vary several-fold between regions for reasons that have nothing to do with what someone chooses to eat. This natural variability is one reason strontium has never been given a recommended intake: there is no “deficiency” to correct, and ordinary diets already supply far more than any biological process requires (which, as Section 4 explains, is effectively zero). The milligram-per-day amounts from food are also orders of magnitude smaller than the hundreds of milligrams in strontium supplements or the ~680 mg of elemental strontium delivered by a daily 2-gram dose of strontium ranelate.
4. Deficiency
There is no recognized strontium deficiency in humans. Because strontium is not an essential nutrient, the body has no requirement for it, and no disease results from low intake — while at very high (pharmacologic) doses strontium can instead harm bone and raise cardiovascular and clotting risk. For full, patient-friendly guides to both ends of the spectrum — what the evidence actually shows about low intake and about excess — see Strontium Deficiency: What the Evidence Shows and Strontium Toxicity: What the Evidence Shows.
5. Recommended Intake
There is no Recommended Dietary Allowance (RDA), Adequate Intake (AI), or other official intake value for stable strontium, and there is no Tolerable Upper Intake Level (UL) set by nutrition authorities such as the U.S. National Academies. This follows directly from the fact that strontium is not essential: agencies set reference intakes only for nutrients the body actually requires. The few milligrams per day supplied by an ordinary diet are neither a target to hit nor a number anyone needs to track.
Drug and supplement doses are a separate matter
The doses that produce strontium’s bone effects are not “intakes” in the nutritional sense; they are pharmacologic doses, and they dwarf dietary amounts:
- Strontium ranelate (prescription, Europe): the studied dose was 2 grams of strontium ranelate once daily, taken as sachets dissolved in water at bedtime. That 2 g of the ranelate salt delivers roughly 680 mg of elemental strontium per day — on the order of 200 times a typical dietary intake.
- Strontium citrate (OTC supplement): products vary, but a common dose supplies a few hundred milligrams of elemental strontium per day (frequently labeled around 340–680 mg elemental). These are also far above dietary levels, though the salt and the supporting evidence differ from the prescription drug.
Why “more” is not automatically “better”
Because there is no established requirement and no defined safe upper limit for nutritional strontium, dosing supplements is essentially self-experimentation with a drug-like substance, without the safety monitoring that accompanies a prescription. Higher strontium does not straightforwardly mean stronger bone — very high strontium can actually impair bone mineralization (Section 7), and apparent gains on bone-density scans are inflated by a measurement artifact (also Section 7). For genuinely essential bone nutrients, by contrast, well-defined intake targets exist precisely because their safety and benefit have been characterized.
6. Supplementation & Forms
Strontium reaches people in two very different ways — as a prescription medicine that exists only outside the United States, and as an OTC dietary supplement. These are not interchangeable, and conflating them is the single most common source of confusion.
Strontium ranelate (prescription — Europe only)
Strontium ranelate (Protelos/Osseor) was approved in the European Union in 2004 for postmenopausal osteoporosis. Its evidence base is two large randomized controlled trials (RCTs):
- SOTI (Spinal Osteoporosis Therapeutic Intervention; Meunier and colleagues, 2004): in postmenopausal women with established osteoporosis, 2 g/day of strontium ranelate over 3 years reduced the risk of new vertebral (spine) fractures by roughly 40–49% compared with placebo.
- TROPOS (Treatment of Peripheral Osteoporosis; Reginster and colleagues, 2005): over 3 years, strontium ranelate reduced non-vertebral fractures, and in a high-risk subgroup (older women, age 74+, with very low hip bone density) it reduced hip fractures. The overall study did not show a hip-fracture benefit; the hip effect was confined to that pre-specified high-risk subgroup, which is an important nuance often dropped in summaries.
The drug was never FDA-approved in the United States, so it has never been legally available there as a medicine. As discussed in Section 8, European regulators later restricted its use and the manufacturer discontinued it.
Strontium citrate and other OTC salts
The strontium sold over the counter is usually strontium citrate, and sometimes strontium chloride, lactate, or gluconate. These are different chemical compounds from the ranelate salt studied in SOTI and TROPOS. A key honesty problem in this market is that supplement marketing frequently implies the ranelate trial results apply to citrate — but that has not been established. There are no large fracture-outcome RCTs for strontium citrate comparable to SOTI/TROPOS; the evidence for citrate is weak and largely indirect (chemical similarity, small studies, surrogate markers such as bone-density readings that are themselves distorted by the strontium artifact).
Practical points if strontium is being considered
- Take strontium and calcium at different times. Because they compete for the same absorption pathways, strontium can reduce calcium absorption (and vice versa). Supplement guidance typically advises separating strontium from calcium-containing meals or supplements by at least a couple of hours.
- Adequate calcium and vitamin D are still required. Strontium is not a substitute for them; the ranelate trials were conducted on a background of calcium and vitamin D supplementation.
- Expect bone-density numbers to be misleading. Any DXA “improvement” while taking strontium overstates true bone gain (Section 7), so scans cannot be taken at face value to judge whether it is working.
7. Toxicity & Upper Limit
Stable strontium is far from harmless at the doses used in medicines and supplements: very high intake can impair bone mineralization (“strontium rickets,” especially with low calcium or in children), inflate bone-density scans through a DXA measurement artifact, and — with strontium ranelate — raise the risk of heart attack, blood clots, and the rare DRESS skin reaction. There is no official nutritional Tolerable Upper Intake Level. For a full, patient-friendly guide to these harms, who should be cautious, and the broader picture of too little versus too much, see Strontium Toxicity: What the Evidence Shows and Strontium Deficiency: What the Evidence Shows.
8. Special Considerations
Strontium ranelate’s rise and fall in Europe
Strontium ranelate illustrates how a drug with proven fracture benefit can still be withdrawn once its harms become clear. After approval in 2004 on the strength of SOTI and TROPOS, post-marketing data and pooled analyses revealed an excess of cardiovascular events — particularly myocardial infarction — and venous blood clots, alongside cases of the serious skin reaction DRESS. In 2013–2014 the European Medicines Agency (EMA) sharply restricted the drug: it was limited to severe osteoporosis in patients who could not use other treatments, contraindicated in people with a history of heart disease, stroke, peripheral arterial disease, uncontrolled high blood pressure, or clotting disorders, and made subject to regular cardiovascular monitoring. Commercially, the medicine was effectively discontinued by its manufacturer around 2017. The practical bottom line for readers in the United States is simple: strontium ranelate is not approved or available there, and even in Europe it is no longer a routine option.
Don’t assume the supplement inherits the drug’s benefits — or escapes its risks
Two opposite errors are common. The first is assuming OTC strontium citrate works as well as ranelate — it has no comparable fracture-outcome trials, so that benefit is unproven. The second is assuming the supplement is automatically safe because it is sold without a prescription — but it still delivers hundreds of milligrams of the same element, and the toxicity concerns (mineralization defects at very high doses, calcium interference, and uncertainty about cardiovascular safety) have never been ruled out for citrate by the kind of large safety studies done for the drug. Honest framing means acknowledging both the weakness of the benefit evidence and the unresolved safety questions for the supplement.
Who should be especially cautious
- Cardiovascular disease or high cardiovascular risk — a history of heart attack, angina, stroke, peripheral arterial disease, or uncontrolled hypertension. The ranelate signal makes any high-dose strontium a poor choice here.
- Clotting risk / history of venous thromboembolism — including people who are immobilized, recovering from surgery, or have a personal or family history of deep-vein thrombosis or pulmonary embolism.
- Kidney disease — strontium is handled and excreted by the kidneys; impaired kidney function changes how it is cleared and concentrated.
- Children and adolescents — growing bone is most vulnerable to strontium-induced mineralization defects.
- Low calcium or vitamin D status — raises the risk of impaired mineralization and undermines any potential benefit.
What actually builds strong bones
Whatever one concludes about strontium, it is at best an adjunct, not a foundation. The well-established pillars of bone health are adequate calcium and vitamin D, vitamin K2 (which helps direct calcium into bone), sufficient dietary protein, and regular weight-bearing and resistance exercise, along with not smoking and limiting heavy alcohol use. For diagnosed osteoporosis, medicines with strong U.S. evidence and approval — bisphosphonates, denosumab, and bone-building agents — are the mainstays. Anyone weighing strontium for bone health should discuss it with a clinician who can weigh the cardiovascular and clotting risks against the modest and uncertain benefit, and who can interpret bone-density scans in light of the strontium artifact.
9. Key Research Papers
- Meunier PJ, Roux C, Seeman E, et al. The effects of strontium ranelate on the risk of vertebral fracture in women with postmenopausal osteoporosis (SOTI). New England Journal of Medicine. 2004;350(5):459–468. doi:10.1056/NEJMoa022436
- Reginster JY, Seeman E, De Vernejoul MC, et al. Strontium ranelate reduces the risk of nonvertebral fractures in postmenopausal women with osteoporosis: TROPOS study. The Journal of Clinical Endocrinology & Metabolism. 2005;90(5):2816–2822. doi:10.1210/jc.2004-1774
- Reginster JY, Bruyère O, Sawicki A, et al. Long-term treatment of postmenopausal osteoporosis with strontium ranelate: results at 8 years. Bone. 2009;45(6):1059–1064. doi:10.1016/j.bone.2009.08.004
- O’Donnell S, Cranney A, Wells GA, Adachi JD, Reginster JY. Strontium ranelate for preventing and treating postmenopausal osteoporosis. Cochrane Database of Systematic Reviews. 2006;(4):CD005326. doi:10.1002/14651858.CD005326.pub2
- Marie PJ. Strontium ranelate: a physiological approach for optimizing bone formation and resorption. Bone. 2006;38(2 Suppl 1):S10–S14. doi:10.1016/j.bone.2005.07.029
- Blake GM, Fogelman I. Long-term effect of strontium ranelate treatment on BMD. Journal of Bone and Mineral Research. 2005;20(11):1901–1904. doi:10.1359/jbmr.050810
- Abrahamsen B, Grove EL, Vestergaard P. Nationwide registry-based analysis of cardiovascular risk factors and adverse outcomes in patients treated with strontium ranelate. Osteoporosis International. 2014;25(2):757–762. doi:10.1007/s00198-013-2469-4
- Cacoub P, Descamps V, Meyer O, et al. Drug rash with eosinophilia and systemic symptoms (DRESS) in patients receiving strontium ranelate. Osteoporosis International. 2013;24(5):1751–1757. doi:10.1007/s00198-013-2265-1
- Storey E. Strontium “rickets”: bone, calcium and strontium changes. Australasian Annals of Medicine. 1961;10(3):213–222. doi:10.1111/imj.1961.10.3.213
- European Medicines Agency (EMA). Protelos/Osseor (strontium ranelate): recommendation to restrict use following review of cardiovascular safety (PRAC, 2013–2014). European Medicines Agency — Protelos/Osseor referral
- MedlinePlus (U.S. National Library of Medicine). Strontium — consumer drug and supplement information. medlineplus.gov — Strontium
- National Institute for Health and Care Excellence (NICE). Osteoporosis: assessing the risk of fragility fracture and management of osteoporotic fractures. nice.org.uk — Osteoporosis guidance
Connections
- Strontium Deficiency: What the Evidence Shows
- Strontium Toxicity: What the Evidence Shows
- All Minerals
- Calcium — the mineral strontium mimics
- Boron and bone health
- Magnesium
- Phosphorus and bone mineral
- Silicon and connective tissue
- Vitamin K2 — directing calcium into bone
- Osteoporosis
- Lab Tests