Molybdenum for Sulfite Metabolism
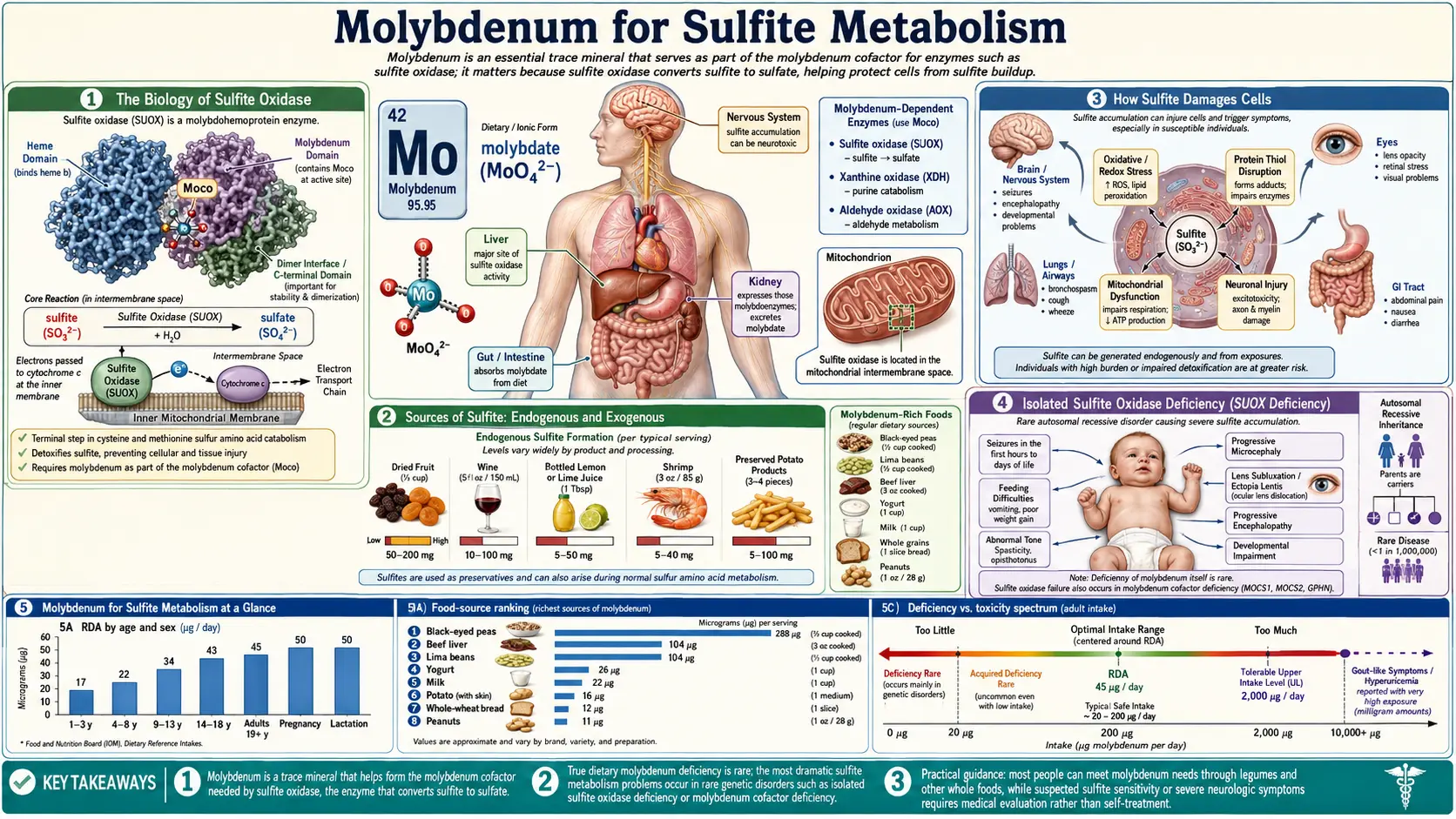
Sulfite oxidase — the molybdenum-dependent enzyme that converts toxic sulfite (SO32−) to inert sulfate (SO42−) — is the body's only enzymatic pathway for clearing sulfite. There is no backup. When sulfite oxidase fails (in molybdenum cofactor deficiency or isolated sulfite oxidase deficiency), sulfite accumulates within hours and destroys developing brain tissue. When it merely runs at low capacity (in some asthmatics, in some individuals with the SUOX low-activity polymorphism), the result is sulfite sensitivity — bronchospasm and anaphylactoid reactions to preserved wine, dried fruits, and processed foods. This page covers the molecular biology of sulfite oxidase, the catastrophic pediatric phenotypes, sulfite sensitivity in adults, the role of cruciferous vegetables and other high-sulfur foods, the interaction with glutathione and the methylation cycle, and practical dietary and supplementation strategies.
Table of Contents
- The Biology of Sulfite Oxidase
- Sources of Sulfite: Endogenous and Exogenous
- How Sulfite Damages Cells
- Isolated Sulfite Oxidase Deficiency
- Sulfite Sensitivity in Adults
- Sulfites and Asthma (The Wine and Salad Bar Story)
- Cruciferous Vegetables and the Sulfur Load
- Interaction with Glutathione and Methylation
- Improving Tolerance for High-Sulfur Diets
- Dietary Strategies for Sulfite-Sensitive Patients
- Molybdenum Supplementation Considerations
- Key Research Papers
- Connections
- Featured Videos
The Biology of Sulfite Oxidase
Sulfite oxidase (SUOX) is a 110 kDa homodimeric enzyme located in the mitochondrial intermembrane space. Each monomer contains:
- A molybdopterin cofactor (Moco) at the active site, which holds the molybdenum atom in coordination geometry that allows two-electron oxygen transfer to sulfite
- A cytochrome b5-type heme domain that accepts electrons from the molybdenum center and shuttles them to the physiological electron acceptor
- A dimerization interface that allows the two monomers to share electron flow
The catalytic mechanism: sulfite binds at the molybdenum center, where an oxygen atom is transferred from a molybdenum-bound oxo group to the sulfur of sulfite, producing sulfate. The molybdenum cycles between Mo(VI) and Mo(IV) oxidation states during the reaction. The electrons released are passed first to the heme cytochrome b5 domain within the enzyme, then to cytochrome c in the mitochondrial respiratory chain, which feeds them into complex IV for ATP production. The overall reaction is therefore not just detoxification but also a modest energy capture — sulfite oxidation contributes electrons to the respiratory chain.
SUOX is expressed in essentially every cell type, with highest expression in liver, kidney, heart, and brain. Brain expression is particularly important because the blood-brain barrier limits sulfite efflux, and developing neurons appear to be the most vulnerable cell type to sulfite toxicity.
The gene encoding sulfite oxidase, SUOX, sits on chromosome 12q13.2. Over 30 disease-causing mutations have been characterized, distributed across the molybdenum-binding domain, the heme domain, and the dimerization interface. Compound heterozygotes for two severe loss-of-function alleles develop isolated sulfite oxidase deficiency in the neonatal period. Heterozygotes with one functional allele appear clinically normal, though they may have measurably reduced enzyme activity and possibly increased sulfite-sensitive symptoms under high sulfite challenge.
Sources of Sulfite: Endogenous and Exogenous
Sulfite (SO32−) reaches the body through two distinct routes that the same sulfite oxidase must handle:
Endogenous sulfite is the larger source by mass. The catabolism of the sulfur amino acids methionine and cysteine generates sulfite as a penultimate intermediate. The cysteine sulfinic acid pathway produces sulfite directly. The transsulfuration pathway feeds methionine through homocysteine and cystathionine to cysteine, which then enters the same sulfite-generating catabolic route. A typical adult consuming the RDA of protein produces approximately 25–30 millimoles of sulfite per day endogenously — far more than typical dietary sulfite intake.
Exogenous sulfite from sulfiting preservatives is the variable, more dramatic source. The major sulfiting agents in food and pharmaceuticals are:
- Sodium sulfite (Na2SO3)
- Sodium bisulfite (NaHSO3)
- Sodium metabisulfite (Na2S2O5)
- Potassium bisulfite (KHSO3)
- Potassium metabisulfite (K2S2O5)
- Sulfur dioxide gas (SO2)
High-sulfite foods and beverages:
- Wine — up to 350 ppm allowed in the US, typically 50–200 ppm; white wines generally higher than reds
- Beer — lower than wine but still measurable in most commercial beers
- Dried fruits — dried apricots, golden raisins, mango, papaya often contain 500–3,000 ppm; dark-colored sun-dried equivalents typically have much less
- Pickled vegetables and condiments — sauerkraut, pickles, horseradish, maraschino cherries
- Packaged shrimp and shellfish — sulfites prevent melanosis (black spotting); frozen and packaged shrimp can carry 100–200 ppm
- Processed meats and gelatin products
- Salad bar produce (historically) — sulfite sprays prevented browning of cut fruits and vegetables; this practice was banned in the US in 1986 after multiple deaths
- Some pharmaceuticals — sulfites are used as antioxidants in epinephrine injectables, some inhaled bronchodilators, and various IV medications
The 1986 FDA labeling rule requires sulfites at or above 10 ppm to be declared on the ingredient label. The pharmaceutical labeling rule from 1987 requires similar disclosure on drug packaging.
How Sulfite Damages Cells
Sulfite is a small, highly reactive nucleophile that damages cells through several distinct mechanisms:
- Disulfide bond disruption — sulfite reacts with the disulfide bonds (S−S) that hold protein tertiary structure together, cleaving them to S-sulfocysteine and free thiol. This destroys protein folding and inactivates enzymes, receptors, and structural proteins. The eye lens is particularly vulnerable because the lens proteins (crystallins) depend on intramolecular disulfides for transparency; this is why lens subluxation is a defining feature of severe sulfite oxidase deficiency.
- S-sulfocysteine formation — sulfite reacts with cysteine to form S-sulfocysteine, a structural analog of glutamate. S-sulfocysteine activates NMDA receptors and other glutamate receptors, producing excitotoxic neuronal injury. This is the molecular basis for the neonatal seizures of sulfite oxidase deficiency.
- Sulfite radical generation — under oxidative conditions, sulfite can undergo one-electron oxidation to sulfite radical anion (SO3−), which propagates lipid peroxidation chain reactions and damages membranes, DNA, and mitochondrial components.
- Glutathione depletion — sulfite reacts with glutathione (GSH) via the cysteinyl thiol, depleting the cell's most abundant antioxidant. Glutathione depletion sensitizes cells to all forms of oxidative injury.
- Mast cell degranulation — sulfite directly triggers mast cell degranulation independent of IgE, releasing histamine, leukotrienes, and prostaglandins. This is the proposed mechanism for the urticaria, angioedema, and anaphylactoid reactions seen in sulfite-sensitive patients.
- Parasympathetic airway reflex — inhaled sulfite (from gas evolving in the stomach after ingestion, or from inhaler preservatives) triggers parasympathetic bronchoconstriction via vagal afferent stimulation. This is a major mechanism in sulfite-induced asthma.
Isolated Sulfite Oxidase Deficiency
Isolated sulfite oxidase deficiency (ISOD) is a rare autosomal recessive disorder caused by biallelic loss-of-function mutations in the SUOX gene. Unlike molybdenum cofactor deficiency (MoCD), where all three molybdoenzymes fail, ISOD selectively eliminates sulfite oxidase — xanthine oxidase and aldehyde oxidase remain functional. Clinical presentation is therefore dominated by pure sulfite toxicity.
Classical (severe) ISOD presents in the first days of life with:
- Intractable myoclonic and generalized tonic-clonic seizures resistant to standard anticonvulsants
- Severe encephalopathy with progressive loss of brainstem reflexes
- Lens subluxation visible on slit-lamp examination — the lens dislocates because sulfite damages the zonular fibers (often the first physical sign noticed)
- Microcephaly developing over weeks to months
- Progressive cystic destruction of cerebral white matter on MRI within weeks
- Death typically by age 1–3 years if untreated
Biochemistry shows elevated urinary sulfite (detectable by Multistix or other reagent strips at the bedside), elevated S-sulfocysteine, elevated thiosulfate, decreased urinary sulfate, normal uric acid (distinguishing ISOD from MoCD where xanthine oxidase failure produces low uric acid), and normal urinary xanthine.
A milder late-onset / atypical ISOD phenotype has been described in older children and adults with residual sulfite oxidase activity, presenting with movement disorders, developmental delay, and intermittent neurological symptoms. These cases often go undiagnosed for years.
No specific replacement therapy exists for ISOD. Unlike MoCD type A, where exogenous cyclic pyranopterin monophosphate can rescue the cofactor biosynthesis defect, the SUOX protein itself is what's missing in ISOD — and protein replacement therapy for mitochondrial enzymes has not yet been developed. Management is supportive: aggressive dietary sulfur restriction (low methionine and cysteine), seizure control, and prevention of further sulfite exposure provide only partial benefit. Several research groups are pursuing gene therapy approaches.
Sulfite Sensitivity in Adults
Sulfite sensitivity affects an estimated 1% of the general population and 5–10% of individuals with asthma. Severity ranges from mild gastrointestinal symptoms after a glass of wine to fatal anaphylactoid reactions requiring emergency epinephrine.
Symptom categories:
- Respiratory — bronchospasm, wheezing, cough, chest tightness, rhinitis. Most common in asthmatic patients.
- Cutaneous — urticaria, angioedema, flushing, pruritus
- Gastrointestinal — cramping, nausea, vomiting, diarrhea
- Cardiovascular — hypotension, tachycardia, syncope
- Anaphylactoid — the full picture of an anaphylactic reaction without IgE involvement
The mechanism is not IgE-mediated true allergy. Most sulfite-sensitive patients have negative skin prick and serum-specific IgE tests for sulfite. The reaction appears to involve:
- Insufficient sulfite oxidase capacity relative to the rapid sulfite bolus, producing transient sulfite accumulation
- Direct mast cell degranulation by sulfite (non-IgE)
- Parasympathetic airway reflexes from inhaled sulfur dioxide gas (especially with wine)
- Possible reduced cysteine availability and glutathione depletion in some patients
Risk factors for sulfite sensitivity include preexisting asthma (especially steroid-dependent), atopic dermatitis, chronic rhinitis, possibly the SUOX low-activity polymorphisms, and underlying mast cell activation syndromes.
Diagnosis is typically clinical (correlation of symptoms with high-sulfite exposures) confirmed by oral sulfite challenge under medical supervision when uncertain. Skin prick testing is not useful because the reaction is not IgE-mediated.
Sulfites and Asthma (The Wine and Salad Bar Story)
The link between sulfites and severe asthma was established in dramatic fashion in the early 1980s when the FDA received reports of multiple deaths from asthma attacks triggered by sulfite-sprayed salad bar produce. Restaurants commonly sprayed cut fruits and vegetables with sulfite solutions to prevent browning; patrons would consume the produce and develop severe bronchospasm within minutes. Investigation linked the deaths to the sulfite spray practice; the FDA banned use of sulfites on fresh fruits and vegetables intended to be served raw in 1986.
The same year, the FDA mandated sulfite labeling on packaged foods at the 10 ppm threshold. Subsequent epidemiology refined the picture: roughly 5–10% of asthmatics are sulfite-sensitive, with the highest prevalence in steroid-dependent and severe asthma. The reaction is rapid (typically within 5–30 minutes of exposure), correlates with sulfite dose, and can be reproduced by oral sulfite challenge under controlled conditions.
The wine reaction is the most commonly recognized sulfite trigger today. Wines must contain sulfites to inhibit microbial spoilage and oxidation during fermentation and aging; legal limits in the US are 350 ppm, with most commercial wines in the 50–200 ppm range. Sulfite-sensitive asthmatics often report wheezing within 5–15 minutes of wine consumption. "No sulfite added" wines (containing only the small amount produced naturally by yeast fermentation, typically <10 ppm) are often better tolerated. Red wines generally contain less added sulfite than whites because the natural antioxidants in red wine (tannins, anthocyanins) provide partial preservative effect.
For patients with sulfite-sensitive asthma, the inhaled bronchodilator emergency may itself be problematic — some metered-dose inhaler preparations contain sulfites as preservative. Patients should review their inhaler ingredient lists with their pulmonologist; sulfite-free formulations are available for most major bronchodilators.
Cruciferous Vegetables and the Sulfur Load
Cruciferous vegetables (broccoli, cauliflower, Brussels sprouts, cabbage, kale, bok choy, arugula, mustard greens, radish, watercress, horseradish) are notable for their high content of glucosinolates — sulfur-containing secondary metabolites that yield isothiocyanates (sulforaphane, indole-3-carbinol, others) upon plant cell rupture. These compounds are widely celebrated for chemopreventive effects via Nrf2 activation and phase II enzyme induction.
However, cruciferous vegetables also contribute meaningful sulfur load to the body. The total sulfur content of a typical broccoli serving is approximately 100–200 mg, much of which enters the methionine-cysteine metabolic pool and eventually generates sulfite that must be cleared by sulfite oxidase. For individuals with limited sulfite oxidase capacity (genetic polymorphisms, suboptimal molybdenum status, or active inflammation), heavy cruciferous intake can produce symptoms of "sulfur intolerance" that overlap with sulfite sensitivity:
- Bloating and gas (some of this is the sulfate-reducing bacteria in the gut converting sulfur compounds to hydrogen sulfide)
- Headache
- Fatigue and brain fog
- Joint pain and inflammation
- Worsening asthma in susceptible individuals
The "sulfur intolerance" phenotype is being increasingly recognized in functional and integrative medicine circles, though it has not been formally codified in standard medical references. Practical evaluation involves a trial of low-sulfur diet (avoiding cruciferous vegetables, alliums, eggs, and animal protein for 2–4 weeks) with symptom tracking, followed by reintroduction. Patients who improve on low-sulfur diet may benefit from molybdenum supplementation (75–500 mcg/day) to support sulfite oxidase capacity before gradually reintroducing high-sulfur foods.
Interaction with Glutathione and Methylation
Sulfite metabolism is intertwined with two of the body's most important sulfur-dependent biochemical systems: glutathione synthesis and the methylation cycle.
Glutathione (GSH) is the tripeptide gamma-glutamyl-cysteinyl-glycine, the body's dominant intracellular antioxidant and the cofactor for phase II conjugation reactions. The rate-limiting amino acid for glutathione synthesis is cysteine, which is derived from the catabolism of methionine via the transsulfuration pathway. This same pathway produces sulfite as a downstream metabolite.
The interplay:
- When sulfite oxidase capacity is adequate, methionine catabolism flows efficiently: methionine → homocysteine → cysteine (some used for glutathione synthesis, some catabolized further) → sulfite → sulfate (excreted)
- When sulfite oxidase is limiting, sulfite accumulates and reacts with cysteine to form S-sulfocysteine, depleting the cysteine pool available for glutathione synthesis
- Sulfite directly reacts with glutathione via the cysteinyl thiol, depleting the GSH pool
- The combined effect is reduced glutathione status, increased oxidative stress, and impaired phase II detoxification — a syndrome that overlaps with what functional medicine practitioners call "stalled methylation"
The methylation cycle connects through homocysteine. Homocysteine sits at a branch point: it can be remethylated back to methionine (via folate/B12 or via betaine), or it can be committed to transsulfuration toward cysteine (via cystathionine beta-synthase, requiring vitamin B6). The choice depends on methionine availability and cellular demand for cysteine/glutathione. When the transsulfuration arm runs at high flux (high cysteine/glutathione demand), sulfite generation is also high, placing demand on sulfite oxidase.
For patients with methylation cycle dysfunction (elevated homocysteine, MTHFR polymorphisms, CBS upregulation polymorphisms), attention to molybdenum status to support sulfite oxidase capacity is sensible. Some functional medicine protocols specifically include molybdenum (typically 75–500 mcg/day) when managing patients with elevated transsulfuration flux.
The interaction with N-acetylcysteine (NAC) is worth noting: NAC provides direct cysteine for glutathione synthesis, but in patients with severely limited sulfite oxidase capacity, large NAC doses can paradoxically worsen sulfur-intolerance symptoms because the cysteine load eventually generates sulfite. Starting NAC at low doses (300–600 mg/day) with concurrent molybdenum supplementation is a reasonable approach for sulfite-sensitive patients who need glutathione support.
Improving Tolerance for High-Sulfur Diets
Many of the foods most prized by health-conscious eaters — cruciferous vegetables, alliums (garlic, onion, leek), pasture-raised eggs, grass-fed beef, organ meats, salmon, sardines, and bone broth — are high in sulfur amino acids. Patients who develop intolerance to these foods often face a difficult choice between symptom management and the nutritional benefits of a sulfur-rich diet.
Strategies to improve tolerance for high-sulfur foods:
- Optimize molybdenum intake — 75–500 mcg/day supports sulfite oxidase capacity. Higher doses (up to the 2,000 mcg/day UL) may be appropriate under clinical supervision.
- Adequate B vitamin status — B6 (pyridoxal-5-phosphate) is required for cystathionine beta-synthase, the enzyme that commits homocysteine to transsulfuration. B12 and folate support remethylation back to methionine, reducing transsulfuration pressure when cysteine/glutathione demand is met.
- Support glutathione synthesis directly — low-dose NAC (300–600 mg/day), liposomal glutathione, or whey protein concentrate (rich in cysteine and glutamylcysteine)
- Address gut sulfate-reducing bacteria — some patients with sulfur intolerance have overgrowth of hydrogen sulfide-producing bacteria (often co-occurring with SIBO). Treatment of the gut overgrowth often improves sulfur tolerance.
- Gradual reintroduction — after a period of low-sulfur diet with molybdenum and B vitamin support, sulfur-rich foods can often be reintroduced gradually, starting with small servings of moderate-sulfur foods (cooked broccoli) before progressing to higher-sulfur items (raw garlic, organ meats).
- Cooking methods matter — thoroughly cooked cruciferous vegetables generally produce less symptoms than raw, possibly because cooking reduces glucosinolate-derived volatile sulfur compounds.
Dietary Strategies for Sulfite-Sensitive Patients
For patients with confirmed or suspected sulfite sensitivity, dietary management focuses on minimizing exogenous sulfite exposure while addressing the underlying capacity limitation:
- Read all labels — "sulfite-free" or "no sulfites added" indicates <10 ppm sulfite
- Avoid the highest-sulfite categories — preserved wine, dried fruits (especially light-colored: golden raisins, dried apricots), packaged shrimp, sauerkraut, pickled vegetables, processed meats
- Choose alternatives — sun-dried (no-sulfite) dried fruit, fresh or frozen shrimp (not packaged with sulfite preservative), "natural" or "biodynamic" wines made with minimal or no added sulfite
- Review medications — some inhaled bronchodilators, IV medications, and even injectable epinephrine pens contain sulfite as antioxidant; ask the pharmacist for sulfite-free alternatives where possible
- Carry an epinephrine auto-injector if previous reactions have been severe; check that the device itself is sulfite-free
- Restaurant strategies — avoid salad bars in older establishments (post-1986 rules should preclude sulfite spraying, but compliance varies); ask about preservatives in shrimp, dried fruit garnishes, and condiments; choose tap water over packaged beverages with unclear preservative content
Molybdenum Supplementation Considerations
For adults with sulfite sensitivity, sulfur intolerance, or chronic exposure to dietary or environmental sulfites, molybdenum supplementation is a low-cost, low-risk intervention that may improve sulfite oxidase capacity. Practical guidance:
- Typical dose — 75–500 mcg/day as sodium molybdate, ammonium molybdate, or molybdenum glycinate chelate. Start at the lower end and titrate based on symptom response over 4–8 weeks.
- Tolerable upper intake limit — 2,000 mcg/day for adults (FNB/IOM). Doses above this carry meaningful risk of copper antagonism and other adverse effects.
- Copper balance — high-dose molybdenum (especially >500 mcg/day for extended periods) can induce functional copper deficiency through thiomolybdate complex formation. Maintain adequate copper intake (1–2 mg/day from food and/or supplement) when using extended high-dose molybdenum.
- Timing — molybdenum has no specific timing requirement; take with or without food
- Form preference — sodium molybdate is the cheapest and most studied form; chelated forms (glycinate) have slightly higher bioavailability but cost more
- Combine with B vitamin support — particularly B6, B12, and folate to support the upstream methylation and transsulfuration cycle
- Monitor for response — reduced sulfite reactions, improved tolerance for previously problematic foods, improved energy. Lack of response after 8 weeks suggests the underlying issue is not molybdenum-limited.
- Caution in established gout — high-dose molybdenum may marginally increase uric acid production via xanthine oxidase support
Key Research Papers
- Schwarz G, Belaidi AA (2013). Molybdenum in human health and disease. Metal Ions in Life Sciences. — PubMed
- Bender D, Tobias Kabil O et al. (2019). Impaired mitochondrial maturation of sulfite oxidase in a patient with severe SUOX deficiency. Human Molecular Genetics. — PubMed
- Tan WH et al. (2005). Isolated sulfite oxidase deficiency: a case report with a novel mutation and review. Pediatrics. — PubMed
- Vincent SH et al. (1991). Sulfite-induced asthma. Annals of Allergy. — PubMed
- Vally H, Misso NL (2012). Adverse reactions to the sulphite additives. Gastroenterology and Hepatology from Bed to Bench. — PubMed
- Simon RA (1998). Update on sulfite sensitivity. Allergy. — PubMed
- Mendel RR, Bittner F (2006). Cell biology of molybdenum. Biochimica et Biophysica Acta. — PubMed
- Belaidi AA, Schwarz G (2013). Metal insertion into the molybdenum cofactor. Biochemical Journal. — PubMed
- Rajagopalan KV, Johnson JL (1992). The pterin molybdenum cofactors. Journal of Biological Chemistry. — PubMed
- Touati G et al. (2000). Molybdenum cofactor deficiency: from genotype to phenotype. Journal of Inherited Metabolic Disease. — PubMed
- Veldman A et al. (2010). Successful treatment of molybdenum cofactor deficiency type A with cPMP. Pediatrics. — PubMed
- Garcia-Castello FJ et al. (2007). Cysteine sulfinic acid decarboxylase, hypotaurine, and taurine. Amino Acids. — PubMed
PubMed Topic Searches
- PubMed: Sulfite oxidase / SUOX
- PubMed: Sulfite sensitivity asthma
- PubMed: Isolated sulfite oxidase deficiency
- PubMed: Transsulfuration cysteine glutathione
- PubMed: Sulfite/sulfate metabolism humans
Connections
- Molybdenum Benefits Hub
- Molybdenum Overview
- Molybdenum for Detoxification
- Molybdenum for Uric Acid
- Molybdenum for Iron Utilization
- Sulfites
- Asthma
- Sulfur
- Cysteine
- Methionine
- N-Acetylcysteine (NAC)
- Glutathione
- Copper
- Vitamin B6
- Vitamin B12
- Oxidative Stress
- Liver Cleansing
- Food Allergies
- All Minerals