Food Allergy
Interactive Visualization Histamine, Mast Cells & Allergy — trigger a mast cell yourself Arm a mast cell with IgE, let the allergen cross-link it, and watch histamine burst out to raise a wheal — then block the H1 receptor and see symptoms fall while histamine still pours out. Launch →
Table of Contents
- Overview
- Prevalence and the Top 9 Allergens
- IgE-Mediated Mechanism: Sensitization and Re-Exposure
- Symptoms: From Mild Reactions to Anaphylaxis
- Special Syndromes: OAS, Alpha-Gal, FPIES
- Non-IgE-Mediated Food Reactions: FPIES and Eosinophilic Disorders
- Diagnosis: Skin Testing, Specific IgE, and Oral Food Challenge
- Component-Resolved Diagnostics: Predicting Severity
- Management: Avoidance, Epinephrine, and Emergency Planning
- Immunotherapy: OIT, EPIT, and SLIT
- Research Papers
- Connections
- Featured Videos
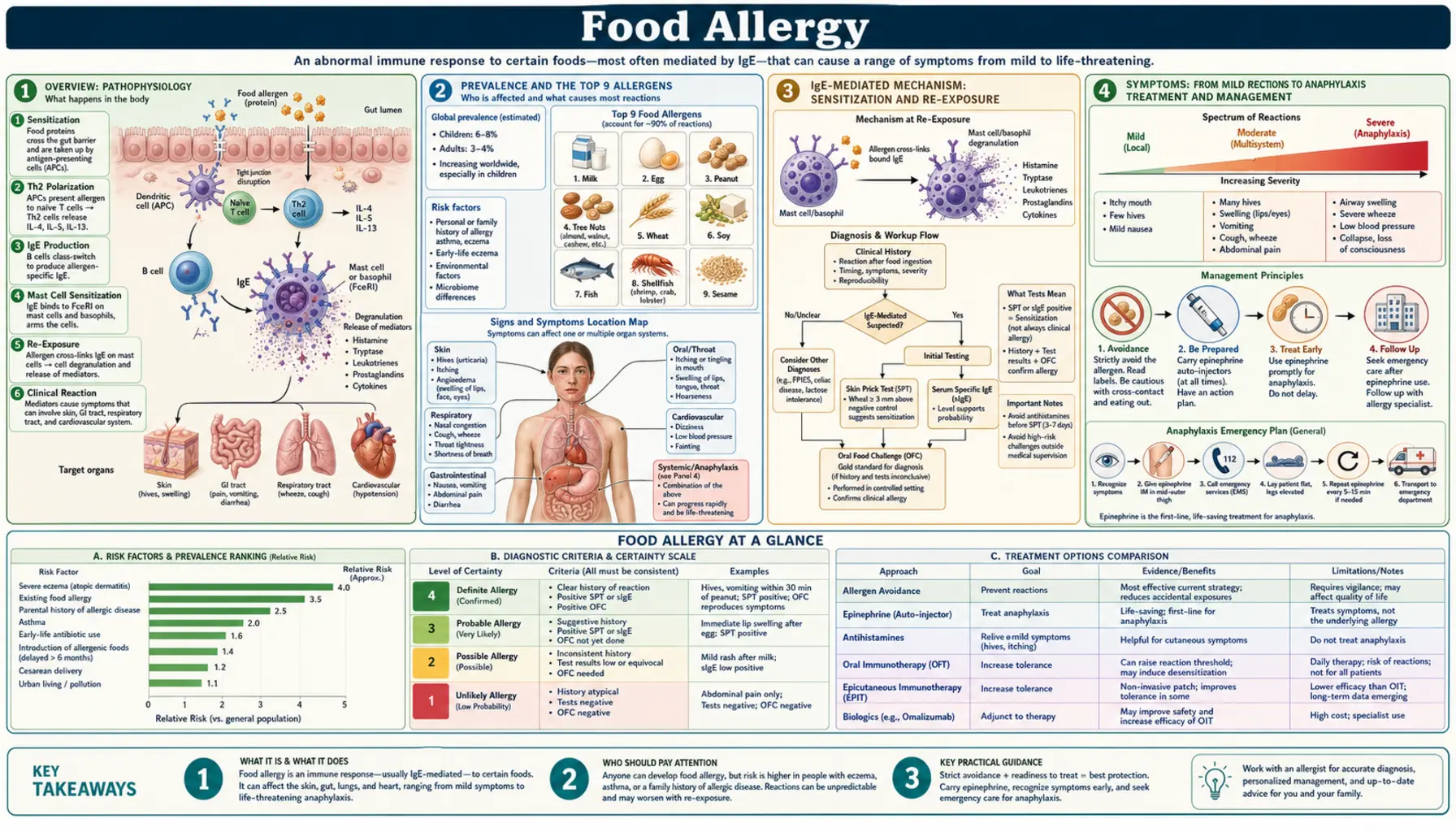
Overview
A food allergy is an immune-mediated adverse reaction to a food protein. This definition is clinically important because it distinguishes true food allergy from food intolerance, which is non-immune and metabolic in origin. Lactose intolerance, for example, results from a deficiency of the enzyme lactase and involves no IgE antibodies or immune activation whatsoever. Conflating the two leads to unnecessary dietary restriction and misallocation of specialist resources.
Food allergy affects approximately 6–8% of children and 3–4% of adults in the United States. Those figures represent a genuine increase over the past three to four decades — not merely better detection. The biological drivers include the hygiene hypothesis (reduced microbial diversity in early life skewing immune development toward Th2 responses), decreased dietary diversity in infancy, increased cesarean delivery rates, and changes in skin barrier integrity linked to rising eczema prevalence.
The clinical stakes are high. Food allergy is the leading cause of anaphylaxis treated in US emergency departments, surpassing medications and insect stings in frequency. Fatal reactions, while rare in absolute terms, disproportionately involve peanuts and tree nuts and are more likely when epinephrine administration is delayed. The annual economic burden in the United States exceeds $25 billion when direct medical costs, lost productivity, and quality-of-life impacts are combined.
Management has historically been limited to strict avoidance and emergency preparedness, but the landscape is changing rapidly. The first FDA-approved oral immunotherapy product for peanut allergy reached the market in 2020, and epicutaneous approaches are advancing through regulatory review. Understanding the immunological basis, diagnostic framework, and emerging treatment options is now essential for patients, parents, and anyone who supports someone living with food allergy.
Prevalence and the Top 9 Allergens
Any food protein is theoretically capable of triggering an allergic response, but in practice a small number of foods account for the overwhelming majority of reactions. The US Congress recognized this in passing the Food Allergen Labeling and Consumer Protection Act (FALCPA) in 2004, which mandated clear disclosure of eight major allergens on packaged food labels. The FASTER Act of 2021 added a ninth: sesame. These nine foods are now required by federal law to be declared in plain language on all packaged food sold in the United States.
- Milk — the most common food allergy in infants and young children; affects approximately 2–3% of infants; most resolve by school age.
- Eggs — second most common in early childhood; roughly 50–70% of children outgrow egg allergy by age 5.
- Fish — includes bass, flounder, cod, salmon, and others; each species is considered a distinct allergen (allergy to one fish does not guarantee allergy to all).
- Shellfish (crustacean) — shrimp, lobster, crab; crustacean shellfish are distinct from mollusks (oysters, clams, scallops); crustacean allergy is more common and more likely to cause severe reactions; rarely outgrown.
- Tree nuts — walnut, cashew, pecan, almond, hazelnut, pistachio, and others; each nut is regulated as a separate allergen; rarely outgrown.
- Peanuts — technically a legume (in the same family as soybeans and lentils), but immunologically and clinically managed as a nut allergen; affects approximately 2% of US children; the most common cause of fatal and near-fatal anaphylactic reactions from food in the United States; only about 20% of affected children outgrow it, making it the most likely food allergy to persist into adulthood.
- Wheat — distinct from non-IgE-mediated gluten sensitivity and from celiac disease, which is an autoimmune condition; IgE-mediated wheat allergy in children is often outgrown by adolescence.
- Soybeans — affects 0.4% of children; most outgrow by age 10; cross-reactivity with other legumes is generally low.
- Sesame — added to FALCPA requirements by the FASTER Act, effective January 1, 2023; affects approximately 0.2% of the US population; prevalence appears to be rising; sesame allergy is often persistent.
Beyond the top 9, clinically significant allergens include mustard, celery, lupin, mollusks (oyster, squid, scallop), and various seeds. In Europe, mustard and celery are among the 14 allergens regulated under EU food labeling law, reflecting regional differences in diet and allergy prevalence.
Peanut allergy deserves special emphasis. It is responsible for more fatal and near-fatal anaphylactic reactions from food than any other single allergen in the United States, partly because of its widespread presence in processed foods and partly because of the potency of its storage proteins (particularly Ara h 2) at low doses. Cross-contamination during food manufacturing is a major practical concern. The "may contain" advisory labeling visible on many packages is voluntary in the US and has no standardized threshold, meaning its protective value varies widely.
IgE-Mediated Mechanism: Sensitization and Re-Exposure
The classical food allergy is an IgE-mediated (Type I hypersensitivity) reaction. Understanding the two-phase process — sensitization followed by re-exposure reaction — is essential for appreciating why someone can eat a food safely for years before suddenly reacting to it.
Phase 1: Sensitization (Silent Phase)
During sensitization, the allergen penetrates the mucosal barrier (or, importantly, the skin barrier) and is processed by antigen-presenting dendritic cells. These cells present allergen peptides to naive T helper cells and, under the influence of the cytokine environment, drive Th2 polarization. Th2 cells secrete IL-4 and IL-13, which signal B cells to undergo class-switch recombination from IgG/IgM production to IgE production. The resulting allergen-specific IgE antibodies bind with high affinity to FcεRI receptors on the surface of mast cells (resident in tissues) and basophils (circulating). At this stage, the individual has been sensitized but has had no allergic reaction. Sensitization is asymptomatic and can occur over weeks to months.
Phase 2: Re-Exposure and Degranulation
On subsequent ingestion of the food, the allergen again enters the body and encounters the IgE molecules already bound to mast cell surfaces. When two adjacent IgE molecules are bridged by the same allergen molecule — a process called IgE cross-linking — the FcεRI receptors aggregate, triggering intracellular signal transduction cascades. Within seconds to minutes, mast cells undergo degranulation: preformed mediators stored in cytoplasmic granules are released. These include:
- Histamine — binds H1 receptors on vascular endothelium and smooth muscle → vasodilation, increased vascular permeability, urticaria, bronchoconstriction, rhinorrhea
- Tryptase — a serine protease; elevated serum tryptase drawn 1–2 hours after a reaction is a useful biomarker confirming mast cell activation
- Prostaglandins and thromboxanes — amplify vascular effects, contribute to bronchoconstriction
- Leukotrienes (LTC4, LTD4, LTE4) — potent bronchoconstrictor and vascular permeability agents; the target of montelukast and other leukotriene receptor antagonists
The clinical manifestations of this immediate-phase reaction appear within 2 hours of ingestion (usually within 30 minutes). This timing is a key diagnostic criterion: symptoms that begin hours or days after eating are less consistent with classic IgE-mediated allergy.
Late-Phase Reaction
In some individuals, a second wave of symptoms occurs 4–12 hours after the immediate reaction. This late-phase response reflects eosinophil, neutrophil, and basophil recruitment to the site of mast cell activation, driven by mediators including IL-5 and eotaxin. Late-phase reactions can persist for 24–48 hours and contribute to chronic inflammation in conditions like eosinophilic esophagitis.
The Dual Allergen Exposure Hypothesis
A landmark insight into food allergy development came from the work of Gideon Lack and colleagues, formalized as the Dual Allergen Exposure Hypothesis. The key observation: infants who are exposed to peanut proteins through eczematous, barrier-disrupted skin (such as from peanut-containing creams or household dust) while avoiding oral ingestion become sensitized. By contrast, infants who regularly consume peanut orally during the period of immune development develop oral tolerance. Cutaneous exposure without oral consumption triggers Th2 skewing and IgE production; oral consumption during the critical window of immune maturation promotes Treg-mediated tolerance.
This hypothesis was directly tested in the LEAP (Learning Early About Peanut allergy) trial (Du Toit et al., NEJM 2015), which randomized high-risk infants (those with severe eczema and/or egg allergy) to consume or avoid peanut from 4–11 months until age 5. Early peanut consumption reduced the prevalence of peanut allergy by 81% compared to avoidance. This finding reversed decades of medical guidance that had recommended allergen avoidance in early life and now underpins current guidelines recommending early dietary introduction of allergenic foods in high-risk infants.
Symptoms: From Mild Reactions to Anaphylaxis
Food allergy reactions span a wide spectrum, from localized skin symptoms to life-threatening cardiovascular collapse. The same individual may react differently on different occasions depending on the dose of allergen, the physiological state at the time (illness, exercise, alcohol, NSAID use can all amplify reactions), and the route and rate of allergen absorption. Symptoms typically appear within minutes to 2 hours of ingesting the offending food.
Cutaneous (Most Common)
Skin and mucous membrane involvement occurs in approximately 90% of allergic reactions. Presentations include urticaria (hives — raised, pruritic wheals), angioedema (deeper swelling of the dermis and subcutaneous tissue, particularly around the lips, eyes, and tongue), generalized flushing and warmth, and diffuse pruritus (itching) without visible rash. The absence of skin symptoms does not rule out anaphylaxis — some severe reactions begin or proceed entirely without cutaneous involvement, a point that often delays recognition.
Gastrointestinal
GI symptoms are the second most common manifestation. They include nausea, projectile or repeated vomiting, diarrhea (sometimes bloody in young infants), abdominal cramping, and bloating. Vomiting that begins within 1–4 hours of ingestion, particularly in infants, may signal FPIES rather than IgE-mediated allergy (see the Non-IgE section below).
Respiratory
Upper airway symptoms include nasal congestion, sneezing, and profuse rhinorrhea. Lower airway involvement produces wheeze, cough, shortness of breath, and chest tightness. Most concerning is laryngeal edema with stridor (a high-pitched sound on inhalation) — edema of the glottis and subglottic structures can progress rapidly to complete airway obstruction and is a medical emergency requiring immediate epinephrine.
Cardiovascular
Cardiovascular manifestations reflect massive vasodilation and fluid extravasation from the vascular space. Hypotension (low blood pressure), compensatory tachycardia (rapid heart rate), pallor, syncope (fainting), and frank cardiovascular collapse (anaphylactic shock) represent the most severe end of the spectrum.
Anaphylaxis
Anaphylaxis is a severe, potentially life-threatening systemic allergic reaction requiring immediate treatment. The Sampson criteria, widely used in clinical practice, define anaphylaxis as highly likely when any one of three conditions is met:
- Acute onset of illness involving the skin or mucous membranes (urticaria, flushing, angioedema) AND at least one of: respiratory compromise (wheeze, stridor, hypoxemia) or reduced blood pressure with end-organ dysfunction (hypotension, collapse, incontinence)
- Two or more of the following occurring rapidly after exposure to a likely allergen: skin/mucosal involvement, respiratory compromise, hypotension, or persistent gastrointestinal symptoms
- Reduced blood pressure alone after exposure to a known allergen
Anaphylaxis can be triggered by trace amounts of allergen — a fact that profoundly affects daily life for affected individuals. There is no minimum safe dose that applies to all patients.
Biphasic anaphylaxis occurs in 10–20% of cases: after the initial reaction is treated and symptoms resolve, a second wave of anaphylaxis returns 1–72 hours later without re-exposure to the allergen. Critically, this delayed second phase can be more severe than the first. This is the clinical justification for the recommendation to observe patients for 4–6 hours after epinephrine administration following an anaphylactic reaction, even when symptoms have completely resolved.
Special Syndromes: OAS, Alpha-Gal, FPIES
Several food-related allergy syndromes do not fit the classic IgE-mediated mold and are frequently misdiagnosed or misunderstood.
Oral Allergy Syndrome (OAS) / Pollen-Food Allergy Syndrome (PFAS)
OAS is caused by IgE cross-reactivity between pollen proteins and structurally homologous proteins in raw plant foods. The immune system, already sensitized to a pollen allergen (such as birch pollen's major allergen Bet v 1), recognizes a similar protein in a raw fruit, vegetable, or nut and mounts a localized IgE response. The cross-reactive proteins in plant foods are members of protein families including PR-10 proteins (Bet v 1 homologs in apples, pears, cherries, peaches, hazelnuts, soybeans — associated with birch pollen allergy), profilins (cross-reactive across many pollens and plant foods), and lipid transfer proteins (LTPs, which are thermostable and can cause more systemic reactions).
Classic OAS symptoms are confined to the oropharynx within seconds of contact with the food: immediate pruritus (itching), tingling, and mild swelling of the lips, tongue, palate, and throat. Symptoms typically resolve within minutes of swallowing or spitting out the food. Because the culprit proteins (particularly PR-10/Bet v 1 homologs) are heat-labile and digestion-labile, they are destroyed by cooking or stomach acid — which is why patients with birch-related OAS can usually eat cooked apple or applesauce without symptoms, but not a raw apple.
Common patterns by pollen sensitization:
- Birch pollen (Bet v 1): apple, pear, peach, cherry, plum, kiwi, hazelnut, almond, celery, carrot, parsley, soybeans (raw)
- Ragweed pollen: melon (cantaloupe, honeydew, watermelon), banana, zucchini, cucumber
- Grass pollen: tomato, peach, melon, orange
OAS rarely progresses to systemic anaphylaxis when the culprit is a PR-10 protein. However, LTP-related OAS (more common in Mediterranean countries) involves a thermostable protein that survives cooking and can cause more severe reactions including anaphylaxis. NSAIDs and vigorous exercise around the time of ingestion can amplify reactions in susceptible individuals.
Alpha-Gal Syndrome (Tick-Bite Sensitization to Red Meat)
Alpha-Gal Syndrome is one of the most unusual food allergy presentations in clinical medicine. Sensitization occurs through the bite of the lone star tick (Amblyomma americanum), which is endemic to the eastern and central United States. The tick injects galactose-α-1,3-galactose (alpha-gal), a carbohydrate moiety present on tick salivary proteins, into the skin. Unlike typical protein allergens, alpha-gal is a carbohydrate — one that is present on the cells of non-primate mammals (cattle, pigs, sheep, venison) but absent in humans and other higher primates. The immune response generates IgE antibodies specifically directed at alpha-gal.
The resulting reaction when the sensitized person consumes red meat (beef, pork, lamb, venison, rabbit) is dramatically delayed compared to classic food allergy: symptoms appear 3–6 hours after eating, often in the middle of the night (since red meat is frequently consumed at dinner). This delay occurs because alpha-gal is only released from meat proteins during digestion, and the resulting lipid-bound alpha-gal moieties are slowly absorbed in the gastrointestinal tract. Symptoms range from isolated urticaria and angioedema to full anaphylaxis.
Key diagnostic clue: serum anti-alpha-gal IgE (a specific ImmunoCAP component test) is the confirmatory biomarker. Management includes strict red meat avoidance and epinephrine prescription. Unlike most food allergies, Alpha-Gal Syndrome may wane over years if the person avoids further tick bites, as the sensitizing antigen is not continuously re-introduced through diet.
FPIES: An Overview
Food Protein-Induced Enterocolitis Syndrome (FPIES) is a non-IgE-mediated food allergy covered in detail in the section below. Unlike OAS and Alpha-Gal, FPIES does not involve IgE and standard allergy testing is typically negative, making it particularly difficult to diagnose without awareness of the syndrome.
Non-IgE-Mediated Food Reactions: FPIES and Eosinophilic Disorders
Not all immune-mediated food reactions are IgE-driven. A distinct group of disorders involves T cell-mediated or mixed mechanisms. These conditions present differently, are diagnosed differently, and are managed differently from classic IgE food allergy.
Food Protein-Induced Enterocolitis Syndrome (FPIES)
FPIES is a non-IgE-mediated gastrointestinal food allergy mediated primarily by T cell and innate immune mechanisms. It is most common in infants, with peak onset around age 6 months as solid foods are introduced. The cardinal symptom is profuse, repetitive projectile vomiting beginning 1–4 hours after ingestion of the trigger food. Vomiting is so severe that it can cause lethargy, pallor, dehydration, and in some cases metabolic acidosis — a presentation that can mimic sepsis. Diarrhea may follow 5–10 hours after exposure.
The most common trigger foods are cow’s milk and soy-based formula. As solid foods are introduced, additional triggers include rice, oat, sweet potato, squash, chicken, and various fruits. Unlike IgE-mediated allergy, standard diagnostic tests (skin prick test, serum IgE) are typically negative, and diagnosis is made on clinical grounds based on a compatible history. There is no reliable biomarker for FPIES, although atypical FPIES with some IgE elevation exists and may be at higher risk of evolution toward classic IgE-mediated allergy.
Treatment of acute FPIES: IV ondansetron (8mg in adults; weight-based in children) is effective in aborting the protracted vomiting. IV fluid replacement addresses dehydration. Epinephrine is generally not required (FPIES is not IgE-mediated) but may be given when the presentation is indistinguishable from anaphylaxis. Oral ondansetron may be used by families for mild FPIES episodes at home.
The natural history is favorable: most children with FPIES to solid foods outgrow it by age 3–5 years. Milk and soy FPIES tends to resolve earlier. Oral food challenges under physician supervision are used to confirm resolution and guide reintroduction.
Eosinophilic Gastrointestinal Disorders (EGIDs)
Eosinophilic Esophagitis (EoE) is the most prevalent EGID and has risen dramatically in incidence over the past 30 years. It is a chronic, immune/antigen-mediated disease characterized by esophageal dysfunction and eosinophilic inflammation on biopsy (≥15 eosinophils per high-power field). In children, it presents with vomiting, feeding difficulties, and failure to thrive. In adults and adolescents, the hallmark symptoms are dysphagia (difficulty swallowing solid foods) and food impaction (food becoming stuck in the esophagus, requiring urgent endoscopic removal). EoE is driven primarily by food antigens rather than aeroallergens, but is not IgE-mediated — serum IgE and skin prick testing have limited diagnostic utility for identifying trigger foods in EoE.
Two evidence-based treatments exist for EoE:
- Dietary elimination: the six-food elimination diet (removing milk, wheat, egg, soy, tree nuts/peanuts, and seafood) followed by systematic reintroduction with esophageal biopsy after each food group is the classic approach; empiric two-food or four-food protocols have shown comparable efficacy with less burden. Milk is the single most common EoE trigger.
- Swallowed topical corticosteroids: fluticasone propionate (swallowed from an MDI, not inhaled) or oral viscous budesonide suppress esophageal eosinophilia; require long-term use to maintain remission; FDA-approved budesonide oral suspension (Eohilia) became available in 2024.
Eosinophilic Gastritis (EoG) and Eosinophilic Gastroenteritis (EoGE) involve eosinophilic infiltration of the stomach and/or small intestine. Symptoms include epigastric pain, nausea, vomiting, and diarrhea. These conditions are rarer than EoE and less well-characterized; management parallels EoE with dietary and corticosteroid approaches.
Food-Protein-Induced Allergic Proctocolitis (FPIAP)
FPIAP affects primarily breast-fed infants in the first weeks to months of life. The sole symptom is blood-streaked, mucoid stool in an otherwise healthy, thriving infant. The reaction is triggered by cow's milk proteins (most commonly) or soy passing through the mother's breast milk. Management consists of eliminating the trigger food from the breastfeeding mother's diet; the condition resolves spontaneously by 12 months of age in most cases.
Celiac Disease: Not a Food Allergy
Celiac disease is frequently grouped with food allergies in public perception but is immunologically distinct. It is a T cell-mediated autoimmune condition triggered by gluten (a protein in wheat, barley, and rye) in genetically susceptible individuals (HLA-DQ2 or HLA-DQ8 haplotypes). The immune response generates anti-tissue transglutaminase IgA (anti-tTG) antibodies and causes intestinal villous atrophy leading to malabsorption. No IgE is involved. Celiac disease is diagnosed by serology (anti-tTG IgA, anti-endomysial antibody) confirmed by small bowel biopsy showing villous atrophy. Treatment is strict lifelong gluten avoidance. Celiac disease does not cause immediate hypersensitivity reactions or anaphylaxis.
Diagnosis: Skin Testing, Specific IgE, and Oral Food Challenge
Diagnosing food allergy accurately is critical: both over-diagnosis (leading to unnecessary dietary restriction, nutritional deficiency, and impaired quality of life) and under-diagnosis (leaving a patient unprotected from anaphylaxis) carry significant harms. The diagnostic approach integrates clinical history, testing, and in many cases a formal food challenge.
Clinical History
A detailed history remains the cornerstone of food allergy evaluation. Key elements to characterize include:
- Timing: onset within 2 hours of ingestion strongly suggests IgE-mediated allergy; delayed onset by hours favors non-IgE mechanisms (FPIES, alpha-gal) or intolerance
- Reproducibility: does the same food consistently cause the same symptoms? One-time unexplained reactions require cautious interpretation
- Dose: does a threshold exist, or do even trace exposures trigger reactions?
- Symptoms and severity: characterize each organ system involved
- Prior reactions and history of tolerance: was the food ever tolerated regularly? If so, sensitization occurred after a period of consumption, which changes the clinical picture
- Co-factors: exercise, alcohol, NSAIDs, illness, or stress can lower the reaction threshold and amplify severity
Skin Prick Test (SPT)
The SPT involves applying a drop of commercial allergen extract (or fresh food) to the forearm or back, then using a lancet to lightly prick the skin through the drop. A positive result is a wheal ≥3 mm larger than the negative control at 15–20 minutes. The SPT has an excellent negative predictive value (greater than 95% for most food allergens) — a negative SPT effectively rules out IgE-mediated allergy in most cases. However, its positive predictive value is only 50–60%, meaning that a positive test alone is insufficient to diagnose allergy in the absence of a compatible history, and it cannot predict reaction severity.
Important limitations: SPT cannot be performed in patients who have taken antihistamines within 3–7 days (depending on the agent); commercial extracts for fruits and vegetables are often less stable than the fresh food (fresh-food "prick-to-prick" testing may be more sensitive for OAS allergens); dermographism and severe eczema can produce false positives.
Specific IgE (Serum ImmunoCAP)
Serum-specific IgE testing (commonly called RAST or ImmunoCAP) measures allergen-specific IgE antibodies in the blood. The result is reported in kUA/L with increasing levels broadly corresponding to increasing probability of clinical reactivity. Like SPT, the negative predictive value is high but the positive predictive value is moderate. Published decision points (e.g., peanut-specific IgE >14 kUA/L = >95% likelihood of reaction in young children) provide some guidance, but these thresholds are age- and population-specific and cannot substitute for clinical judgment.
Serum IgE testing is particularly useful when SPT is technically difficult (extensive eczema, dermographism) or when antihistamines cannot be withheld. An undetectable specific IgE does not rule out non-IgE-mediated food allergy (FPIES, EoE, FPIAP).
Oral Food Challenge (OFC): Gold Standard
The double-blind, placebo-controlled oral food challenge (DBPCFC) is the gold standard for definitively diagnosing or ruling out food allergy. It is also the definitive test for confirming that a child has outgrown a food allergy, enabling safe reintroduction. The challenge involves administering incremental, graded doses of the suspected allergen under direct physician supervision, with emergency medications and equipment immediately available. Doses are increased at timed intervals while the patient is observed for any objective signs of reaction.
OFCs are time- and resource-intensive, carry a risk of provoking a reaction, and must be performed in a clinical setting. They are indicated when:
- The diagnosis is uncertain based on history and testing alone
- Monitoring whether a previously confirmed allergy has resolved (particularly relevant for milk, egg, wheat, and soy in children)
- Assessing tolerance of baked or processed forms of an allergen (e.g., baked milk in a milk-allergic child)
- Guiding immunotherapy candidacy
Atopy Patch Test and Basophil Activation Test
The atopy patch test (APT) applies food allergens to intact skin under occlusive patches for 48–72 hours and reads delayed reactions. It has been investigated as an adjunct for identifying non-IgE triggers in EoE but has inconsistent results and is not considered standard of care for diagnosis.
The basophil activation test (BAT) measures IgE-triggered CD63 (or CD203c) upregulation on circulating basophils after allergen stimulation ex vivo. BAT has demonstrated specificity exceeding 90% for peanut allergy in research settings and may be helpful in distinguishing true peanut allergy from sensitization without clinical reactivity. It is not yet routinely available in clinical practice but is advancing toward clinical use.
Component-Resolved Diagnostics: Predicting Severity
Traditional specific IgE testing measures total IgE against a whole food extract. Component-resolved diagnostics (CRD) goes further: it measures IgE against individual molecular components (specific proteins) within a food, providing information about the nature of the sensitization and its likely clinical consequences. CRD is now clinically available for several major allergens and has transformed the ability to predict reaction severity and guide management decisions.
Peanut Components
- Ara h 1, Ara h 2, Ara h 3 — storage proteins (vicilin, 2S albumin, legumin respectively); heat-stable and resistant to digestion; sensitization to these components, especially Ara h 2, predicts a high risk of systemic reactions including anaphylaxis. Ara h 2 alone has the highest positive predictive value for clinically significant peanut allergy.
- Ara h 8 — a PR-10 protein (Bet v 1 homolog); sensitization reflects birch pollen cross-reactivity; typically causes mild OAS limited to the oropharynx; Ara h 8-only sensitization with negative Ara h 2 strongly predicts mild reactions.
- Ara h 9 — a lipid transfer protein (LTP); thermostable; more common in Mediterranean populations; associated with moderate-to-severe systemic reactions.
Milk Components
- nBos d 4 (α-lactalbumin) and nBos d 5 (β-lactoglobulin) — whey proteins; heat-labile; sensitization to these alone (with low or absent casein IgE) predicts likelihood of tolerating extensively heated (baked) milk products, which is clinically important as many milk-allergic children can safely eat baked goods containing milk.
- Bos d 8 (caseins) — thermostable; high casein-specific IgE predicts persistent milk allergy and inability to tolerate baked milk; an important marker for natural history prognosis.
Egg Components
- Gal d 1 (ovalbumin) — heat-labile; patients with IgE primarily to ovalbumin may tolerate baked egg (e.g., in a muffin) even if they react to raw or lightly cooked egg.
- Gal d 2 (ovomucoid) — thermostable; high ovomucoid-specific IgE predicts persistent egg allergy and inability to tolerate baked egg; an important natural history marker.
Hazelnut Components
- Cor a 1 — a PR-10 (Bet v 1 homolog); sensitization usually reflects birch cross-reactivity and predicts mild OAS only.
- Cor a 9 and Cor a 14 — storage proteins; IgE to these predicts a high risk of systemic anaphylaxis from hazelnut regardless of cooking.
Wheat and Exercise-Induced Anaphylaxis
- ω-5-gliadin (Tri a 19) — the specific component responsible for wheat-dependent, exercise-induced anaphylaxis (WDEIA), a syndrome in which neither wheat ingestion alone nor exercise alone triggers a reaction, but the combination does. Tri a 19-specific IgE is the diagnostic biomarker of choice for WDEIA.
CRD is increasingly available through reference laboratory platforms (e.g., Thermo Fisher ImmunoCAP ISAC multiplexed array or single-component tests) and is reshaping the pre-challenge risk stratification process in specialized allergy centers.
Management: Avoidance, Epinephrine, and Emergency Planning
The cornerstone of food allergy management remains strict avoidance of the culprit food. While this sounds straightforward, in practice it requires knowledge, vigilance, and planning across every food environment the patient encounters.
Allergen Avoidance
FALCPA mandates that all nine major allergens be declared in plain English on packaged food labels sold in the United States, either in the ingredient list or in a separate "Contains" statement. However, several important gaps exist:
- "May contain" advisory labeling (e.g., "may contain traces of peanuts" or "processed in a facility that also handles tree nuts") is entirely voluntary in the US and has no standardized threshold. Studies show that a meaningful proportion of "may contain" labeled products do contain detectable allergen, but the levels vary widely. Patients must make individualized risk decisions about advisory labels in consultation with their allergist.
- Restaurant food is not covered by FALCPA. Cross-contamination at restaurants — from shared fryers, utensils, and preparation surfaces — is responsible for a significant proportion of accidental exposures. Communication with restaurant staff, menu review, and awareness of high-risk cuisines (peanut-heavy Asian cuisines, shellfish in seafood restaurants) are essential.
- Hidden sources: milk in "non-dairy" creamers, peanut in chili or satay sauces, egg in pasta and baked goods, fish sauce in Worcestershire sauce, and soy in many processed foods require label literacy.
Epinephrine Auto-Injectors
Epinephrine (adrenaline) is the only effective first-line treatment for anaphylaxis. Antihistamines and inhaled bronchodilators are adjunctive treatments only — they address individual symptoms (histamine-mediated urticaria, bronchospasm) but do not reverse the multisystem pathophysiology of anaphylaxis and must never be used as substitutes for epinephrine. Studies of fatal food anaphylaxis consistently find that epinephrine was not given, or was given too late.
Epinephrine auto-injectors (EpiPen, Auvi-Q, and generic equivalents) should be prescribed for every patient with IgE-mediated food allergy who is at risk of anaphylaxis. Standard prescribing:
- 0.3 mg for adults and children weighing more than 30 kg
- 0.15 mg for children weighing 15–30 kg
- Injected into the anterolateral thigh (outer thigh), through clothing if necessary; this route delivers peak epinephrine levels faster than the deltoid (arm) injection
- Two auto-injectors should always be prescribed and carried, as a second dose may be needed if the first is insufficient or if biphasic anaphylaxis occurs before emergency services arrive
- After administering epinephrine, call 911 (or local emergency services) immediately and proceed to an emergency department, even if symptoms resolve
Emergency Action Plan
All patients (and parents/guardians of affected children) should have a written, individualized Food Allergy Emergency Action Plan (FARE provides a widely used template). The plan should specify: the patient's confirmed allergens, a graded symptom chart, when to administer epinephrine, emergency contact information, and how to call for emergency help. For school-age children, this plan should be shared with all teachers, coaches, cafeteria staff, and the school nurse. Many US states have laws permitting schools to stock undesignated epinephrine for use in allergic emergencies when the student's own device is unavailable.
Medical Alert Identification
Medical alert bracelets, necklaces, or digital identification specifying the food allergen(s) and "carries epinephrine" can be life-saving in emergency situations where the patient cannot communicate.
Dietitian Referral
Patients eliminating multiple foods or entire food groups (particularly milk, egg, wheat, or fish) are at risk for nutritional deficiencies. Referral to a registered dietitian with food allergy experience is recommended to ensure adequate intake of calcium and vitamin D (milk-restricted), B vitamins and iron (wheat-restricted), omega-3 fatty acids (fish-restricted), and high-quality protein sources across the diet. Unnecessary food restriction in children can impair growth and development.
Immunotherapy: OIT, EPIT, and SLIT
For the first time in the history of food allergy treatment, active immunological interventions are available or in advanced development that can raise the threshold for allergic reaction, reducing risk from accidental exposures. None of these treatments are cures, and all require ongoing maintenance. They represent a significant but carefully bounded advance.
Peanut Oral Immunotherapy (OIT) — Palforzia
In January 2020, the FDA approved Palforzia (AR101, peanut allergen powder) for the mitigation of allergic reactions in individuals 4–17 years old with confirmed peanut allergy. Palforzia was the first food allergen immunotherapy product approved in the United States.
The treatment consists of three phases:
- Initial dose escalation: performed in a clinical setting; doses begin at 0.5 mg of peanut protein and are increased in a single day to the starting maintenance-escalation dose
- Up-dosing: patients increase their daily dose every two weeks over approximately 6 months, from 0.5 mg up to 300 mg (the maintenance dose), with each dose increase supervised in clinic
- Maintenance: 300 mg of peanut protein daily indefinitely
In the pivotal PALISADE trial (Vickery et al., NEJM 2018), approximately 67% of treated patients (ages 4–17) tolerated 600 mg of peanut protein (the equivalent of approximately 2 peanuts) at exit food challenge, compared to 4% of placebo recipients. This represents desensitization — an elevation of the reaction threshold — not a cure. Patients must continue daily maintenance dosing to preserve desensitization; stopping treatment typically results in loss of tolerance within weeks to months.
Critical limitation: Palforzia does not enable intentional peanut consumption. Its goal is protection from accidental low-dose exposures (e.g., cross-contamination), not the ability to eat peanuts freely. Patients must continue carrying epinephrine throughout treatment and after. The risk of anaphylaxis during OIT escalation is real — estimated at 2–5% of patients requiring epinephrine during the up-dosing phase — and OIT must only be administered under allergist supervision with emergency equipment available.
Epicutaneous Immunotherapy (EPIT) — Viaskin Peanut
Viaskin Peanut (DBV Technologies) delivers peanut antigen via a patch applied daily to intact, unbroken skin. The Viaskin patch creates a moisture-occlusive chamber that enhances local antigen uptake via epidermal Langerhans cells, which are tolerogenic by nature. Because the antigen is taken up by the skin rather than the gut mucosa, systemic absorption is minimal, resulting in a substantially lower rate of systemic reactions compared to OIT — an important safety advantage.
The FDA's Allergenic Products Advisory Committee voted in favor of Viaskin Peanut for children ages 4–7 in 2024, though regulatory approval timing remained under negotiation. Efficacy in the PEPITES trial (Fleischer et al., JAMA 2019) was lower than Palforzia OIT (approximately 35% response rate by strict criteria), but the favorable safety profile makes EPIT particularly attractive for young children and those unable to tolerate the systemic reactions associated with oral dosing. EPIT research is also active for milk allergy.
Sublingual Immunotherapy (SLIT)
SLIT involves placing small amounts of allergen extract under the tongue and holding it for 2 minutes before swallowing. The sublingual mucosa is rich in tolerogenic dendritic cells and regulatory T cells. SLIT has been studied for peanut, hazelnut, and peach allergy. Its efficacy is lower than OIT but its safety profile is better, with predominantly local (oromucosal) side effects rather than systemic reactions. No SLIT product for food allergy has received FDA approval as of 2024, but research programs continue.
Natural Resolution and Outgrowth
Many childhood food allergies resolve spontaneously, making annual re-evaluation with SPT, specific IgE, and supervised oral food challenge an important part of management:
- Milk: 50–80% resolved by age 3–5
- Egg: 50–70% resolved by age 5
- Wheat: approximately 65% resolved by age 12
- Soy: approximately 50% resolved by age 7
- Peanut: only approximately 20% outgrow; annual re-evaluation recommended in children to identify those who may be candidates for supervised challenge or immunotherapy
- Tree nuts and shellfish: rarely outgrown; typically require lifelong management
The concept of the baked milk/egg ladder has emerged from natural history research: many children allergic to raw milk or egg can tolerate extensively heated (baked) forms of these allergens. Regular consumption of baked forms may accelerate the development of tolerance to raw forms, and structured introduction of baked forms followed by progressively less-heated forms is now incorporated into management guidelines for selected patients.
Research Papers
- Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy (LEAP trial). N Engl J Med. 2015;372(9):803–813. PMID: 25705822
- Sampson HA, Aceves S, Bock SA, et al. Food allergy: a practice parameter update—2014. J Allergy Clin Immunol. 2014;134(5):1016–1025.e43. PMID: 25174862
- Gupta RS, Springston EE, Warrier MR, et al. The prevalence, severity, and distribution of childhood food allergy in the United States. Pediatrics. 2011;128(1):e9–17. PMID: 21690110
- Sicherer SH, Sampson HA. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol. 2018;141(1):41–58 — Search PubMed
- Commins SP, Satinover SM, Hosen J, et al. Delayed anaphylaxis, angioedema, or urticaria after consumption of red meat in patients with IgE antibodies specific for galactose-alpha-1,3-galactose. J Allergy Clin Immunol. 2009;123(2):426–433. PMID: 19070355
- Benhamou AH, Schäppi Tempia MG, Belli DC, Eigenmann PA. An ICON summary of diagnosis, management and prevention of allergic reactions to cow’s milk protein. World Allergy Organ J. 2017;10(1):27 — Search PubMed
- Vickery BP, Vereda A, Casale TB, et al. AR101 Oral Immunotherapy for Peanut Allergy. N Engl J Med. 2018;379(21):1991–2001. PMID: 30449234
- Wang J, Sampson HA. Food allergy. J Clin Invest. 2011;121(3):827–835 — Search PubMed
- Fleischer DM, Greenhawt M, Sussman G, et al. Effect of epicutaneous immunotherapy vs placebo on reaction to peanut protein ingestion among children with peanut allergy: The PEPITES randomized clinical trial. JAMA. 2019;321(10):946–955 — Search PubMed
- Nowak-Wegrzyn A, Sampson HA, Wood RA, Sicherer SH. Food protein-induced enterocolitis syndrome caused by solid food proteins. Pediatrics. 2003;111(4 Pt 1):829–835 — Search PubMed
- Keet CA, Matsui EC, Dhillon G, Lenehan P, Paterakis M, Wood RA. The natural history of wheat allergy. Ann Allergy Asthma Immunol. 2009;102(5):410–415 — Search PubMed
- Eigenmann PA, Caubet JC, Zamora SA. Are avoidance diets still warranted in children with atopic dermatitis? Pediatr Allergy Immunol. 2020;31(1):19–26 — Search PubMed
PubMed Topic Searches:
- Food allergy IgE anaphylaxis
- Peanut allergy oral immunotherapy
- FPIES food protein-induced enterocolitis syndrome
- Eosinophilic esophagitis food elimination diet
- Alpha-gal syndrome tick bite red meat
- Component-resolved diagnostics food allergy
Connections
- Pain & Allergy
- Histamine, Mast Cells & Allergy — interactive animation
- Allergies
- Anaphylaxis
- Chronic Urticaria
- Eosinophilic Esophagitis
- Alpha-Gal Syndrome
- Drug Allergy
- Mast Cell Activation Syndrome
- Food Intolerance
- All Conditions