Magnesium Glycinate — Benefits Deep Dive
Magnesium glycinate is the most-bioavailable and gentlest-on-gut form of magnesium — a chelate in which the Mg2+ ion is held in a stable claw-like grip by two molecules of the inhibitory amino acid glycine. That dual identity makes it unique among magnesium supplements: the magnesium half is the cofactor for more than 600 enzymes (ATP production, DNA repair, the Na/K ATPase pump, NMDA channel gating), while the glycine half is itself a sleep-promoting and anxiety-reducing neurotransmitter that builds collagen and feeds glutathione synthesis. The four deep-dive pages below walk through the specific clinical applications where magnesium glycinate outperforms every other form: the sleep architecture changes documented in Inagawa's pre-bed glycine trial, the GABA-A potentiation and HPA-axis modulation behind its anxiolytic effect, the muscle-relaxation profile that makes it the preferred form for nocturnal cramps and restless legs, and the chelate chemistry that delivers 80%+ absorption versus the ~4% bioavailability of magnesium oxide.
Deep-Dive Articles
Sleep Quality
Why magnesium glycinate is the most-prescribed natural sleep aid in 2026. The dual mechanism — magnesium as cofactor for the pineal serotonin-to-melatonin conversion and as NMDA receptor blocker, plus glycine's own sleep effects via peripheral vasodilation and core temperature drop. The Inagawa pre-bed glycine + sleep architecture study, REM/NREM effects, and comparison to magnesium L-threonate (CNS targeting) and malate (energy/fibromyalgia).
Anxiety Relief
The neurochemistry of magnesium's anxiolytic effect: GABA-A receptor positive allosteric modulation (the same target as benzodiazepines, without the dependence), NMDA glutamate channel blockade, and HPA-axis dampening. Glycine's role as the dominant inhibitory neurotransmitter of the brainstem and spinal cord. The Boyle 2017 systematic review of 18 trials, the cortisol/magnesium vicious circle, and the place of glycinate in adult anxiety treatment alongside therapy and SSRIs.
Muscle Relaxation
Why glycinate is the preferred form for muscle cramps when oxide and citrate cause diarrhea. Magnesium as a physiological calcium antagonist at the sarcoplasmic reticulum, nocturnal leg cramp evidence, restless legs syndrome trials, fibromyalgia and chronic tension applications, training-induced muscle tension in athletes, and pregnancy-related leg cramps where glycinate's gentle profile matters most.
Bioavailability
The chelate chemistry that defines glycinate — the Albion patented process, the comparison of fractional absorption across forms (oxide ~4%, citrate ~30%, glycinate 80%+), saturation kinetics, the difference between "fully reacted" chelate and oxide-buffered-with-glycine impostors, third-party testing (USP, NSF, ConsumerLab), label red flags that signal inferior product, and how to read a Certificate of Analysis.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- Deep-Dive Articles
- Why Magnesium Glycinate Produces Effects Across Many Systems
- Research Papers: Sleep Quality
- Research Papers: Anxiety & Stress
- Research Papers: Muscle Relaxation & Cramps
- Research Papers: Bioavailability & Chelate Chemistry
- Research Papers: Cross-Cutting (Magnesium Status, Glycine Biology)
- External Authoritative Resources
- Connections
- Featured Videos
Why Magnesium Glycinate Produces Effects Across Many Systems
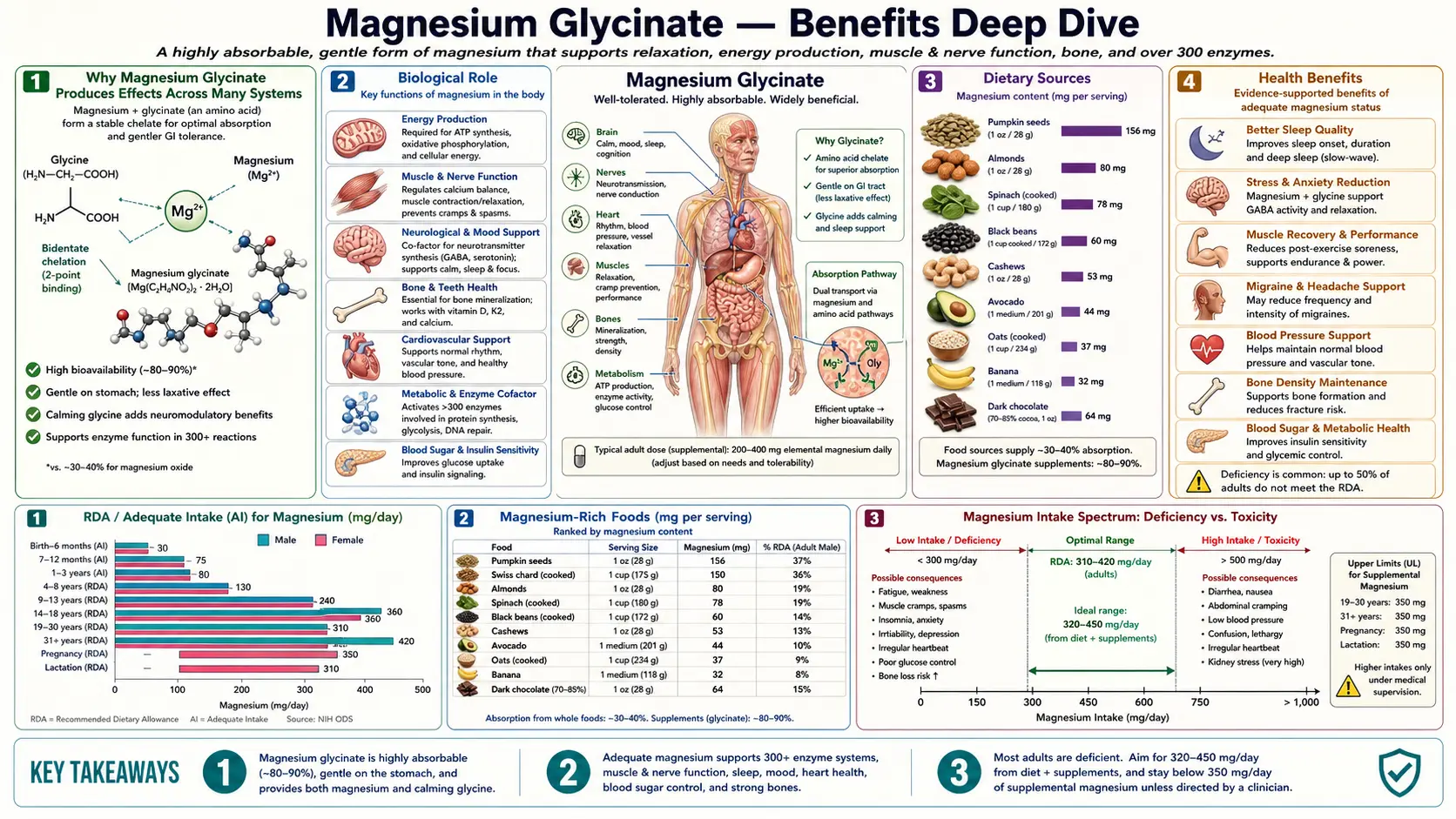
Most supplements act through one principal mechanism. Magnesium glycinate is unusual because it delivers two biologically active molecules that each operate through fundamentally different mechanisms, and the two effects converge on the same therapeutic territory — sleep, anxiety, muscle tension, and nervous-system tone. Each of the two ingredients maps to a distinct family of clinical effects, and the overlap is precisely what makes the chelate so versatile.
- Magnesium as a 600-enzyme cofactor — the Mg2+ ion is required by more than 600 mammalian enzymes, including every reaction that uses ATP (Mg2+ is the counter-ion that stabilizes the phosphate groups), the Na/K-ATPase pump that establishes the neuronal resting potential, glutamic acid decarboxylase that produces inhibitory GABA, and the methyltransferases that handle DNA repair and methionine cycling. Magnesium also sits as a voltage-dependent plug in the NMDA glutamate receptor ion channel, preventing calcium influx during normal neuronal activity. Loss of that NMDA block in magnesium deficiency is the proximate molecular cause of anxiety, hyperexcitability, and insomnia in deficient individuals — and the proximate target of magnesium's anxiolytic effect when status is restored.
- Glycine as an inhibitory neurotransmitter, collagen building block, and glutathione precursor — glycine is the smallest amino acid and one of the most metabolically versatile. It is the dominant inhibitory neurotransmitter of the brainstem and spinal cord (acting through strychnine-sensitive glycine receptors, separate from GABA), one of three amino-acid precursors to glutathione (the body's master antioxidant), and one in every three amino acids in collagen. Glycine also acts as a co-agonist at the NMDA receptor (the glycine binding site is required for the receptor to open even in the presence of glutamate), and it lowers core body temperature by dilating peripheral blood vessels — the physiological signal that initiates sleep onset.
- Chelate chemistry that protects both molecules through digestion — the magnesium-glycine bisglycinate chelate is a stable five-membered ring in which two glycine molecules grip the Mg2+ ion through nitrogen and oxygen coordination. The ring structure protects the magnesium from precipitation by stomach acid, from chelation by dietary phytates and oxalates, and from saturation of the passive paracellular magnesium absorption channels. The intact chelate is absorbed through amino-acid transport pathways in the small intestinal enterocyte, then split intracellularly into free Mg2+ and free glycine for their downstream effects. The fractional absorption advantage over magnesium oxide is roughly 20-fold — the engineering reason glycinate has displaced cheaper forms as the clinical standard.
The clinical convergence is what makes the supplement therapeutically powerful. Magnesium and glycine each independently promote sleep (magnesium via melatonin synthesis and GABA-A potentiation, glycine via core temperature drop and NMDA modulation), each independently reduce anxiety (magnesium via GABA-A modulation and HPA-axis dampening, glycine via brainstem and spinal cord glycine receptors), and each independently support muscle relaxation (magnesium via calcium antagonism at the sarcoplasmic reticulum, glycine via spinal cord motor neuron inhibition through Renshaw cell circuits). The combined effect on these overlapping outcomes is greater than either ingredient alone — which is why muscle cramp prevention studies consistently rank glycinate above other magnesium forms despite the absence of any difference in elemental magnesium delivered per dose. The form genuinely matters, not just the dose.
Research Papers: Sleep Quality
- Magnesium bisglycinate supplementation in healthy adults reporting poor sleep (RCT) — PubMed: Bisglycinate sleep RCT
- Inagawa K et al. (2006). Subjective effects of glycine ingestion before bedtime on sleep quality — PubMed: Inagawa pre-bed glycine
- Bannai M, Kawai N (2012). New therapeutic strategy for amino acid medicine: glycine improves the quality of sleep — PubMed: Glycine sleep mechanism
- Yamadera W et al. Glycine ingestion improves subjective sleep quality and shortens latency to slow-wave sleep — PubMed: Glycine slow-wave sleep
- Abbasi B et al. (2012). The effect of magnesium supplementation on primary insomnia in elderly — PubMed: Abbasi magnesium insomnia
- Wienecke E, Nolden C. Long-term HRV analysis shows stress reduction by magnesium intake — PubMed: HRV and magnesium
- Held K et al. Oral magnesium supplementation improves slow wave sleep in elderly subjects — PubMed: Held slow-wave sleep
- Cao Y et al. (2018). Magnesium intake and sleep disorder symptoms in the Jiangsu Nutrition Study — PubMed: Magnesium and sleep disorders
- Wang J et al. (2024). The effect of magnesium-l-threonate on cognition and sleep — PubMed: L-threonate vs glycinate
- Slutsky I et al. (2010). Enhancement of learning and memory by elevating brain magnesium (L-threonate) — PubMed: Slutsky brain magnesium
Research Papers: Anxiety & Stress
- Boyle NB et al. (2017). The effects of magnesium supplementation on subjective anxiety and stress: a systematic review — PubMed: Boyle 2017 systematic review
- Sartori SB et al. (2012). Magnesium deficiency induces anxiety and HPA axis dysregulation — PubMed: Magnesium HPA axis
- Pickering G et al. (2020). Magnesium status and stress: the vicious circle concept revisited — PubMed: Magnesium-stress cycle
- Botturi A et al. (2020). The role and the effect of magnesium in mental disorders — PubMed: Magnesium and mental disorders
- de Baaij JH, Hoenderop JG, Bindels RJ. Magnesium in man: implications for health and disease — PubMed: Magnesium physiology review
- Eby GA, Eby KL. Rapid recovery from major depression using magnesium treatment — PubMed: Eby magnesium depression
- Tarleton EK et al. (2017). Role of magnesium supplementation in the treatment of depression — PubMed: Tarleton depression RCT
- Kalueff AV, Nutt DJ. Role of GABA in anxiety and depression — PubMed: GABA in anxiety
- Lopez-Corcuera B et al. Glycine neurotransmitter transporters: an update — PubMed: Glycine neurotransmitter
- File SE et al. Glycine as an inhibitory neurotransmitter at higher centres — PubMed: Glycine higher centres
Research Papers: Muscle Relaxation & Cramps
- Garrison SR et al. (2020). Magnesium for skeletal muscle cramps (Cochrane Review) — PubMed: Cochrane cramps review
- Roffe C et al. Randomised, cross-over, placebo controlled trial of magnesium citrate in chronic persistent leg cramps — PubMed: Roffe leg cramps trial
- Supakatisant C, Phupong V. Oral magnesium for relief in pregnancy-induced leg cramps — PubMed: Pregnancy leg cramps
- Hornyak M et al. Magnesium therapy for periodic leg movements-related insomnia and restless legs syndrome — PubMed: Hornyak RLS
- Kovacs L, Molnar BG, Huhn E, Bodis L. Magnesium substitution in pregnancy — randomized double-blind trial — PubMed: Kovacs pregnancy trial
- Bagis S et al. Is magnesium citrate treatment effective on pain, clinical parameters and functional status in patients with fibromyalgia? — PubMed: Magnesium fibromyalgia
- Andretic R et al. Calcium-magnesium balance and muscle excitability — PubMed: Ca/Mg muscle balance
- Zhang Y et al. (2024). Effects of magnesium supplementation on muscle soreness in different types of physical activity — PubMed: Zhang muscle soreness
- Setaro L et al. Magnesium status and the physical performance of volleyball players — PubMed: Magnesium volleyball
- Veronese N et al. Effect of oral magnesium supplementation on physical performance in healthy elderly — PubMed: Magnesium elderly performance
Research Papers: Bioavailability & Chelate Chemistry
- Blancquaert L, Vervaet C, Derave W. (2019). Predicting and testing bioavailability of magnesium supplements — PubMed: Bioavailability prediction
- Schuette SA et al. Bioavailability of magnesium diglycinate vs magnesium oxide in patients with ileal resection — PubMed: Diglycinate vs oxide
- Walker AF et al. Mg citrate found more bioavailable than other Mg preparations in a randomised double-blind study — PubMed: Walker bioavailability
- Lindberg JS et al. Magnesium bioavailability from magnesium citrate and magnesium oxide — PubMed: Lindberg citrate vs oxide
- Mhlmann S et al. Bioavailability of magnesium L-aspartate-hydrochloride versus magnesium oxide — PubMed: Aspartate vs oxide
- Ranade VV, Somberg JC. Bioavailability and pharmacokinetics of magnesium after administration of magnesium salts to humans — PubMed: Ranade pharmacokinetics
- Coudray C et al. Study of magnesium bioavailability from ten organic and inorganic salts (rats, isotope) — PubMed: Ten-salt comparison
- Ashmead HD. Conversations on chelation and mineral nutrition (Albion chelate mechanism) — PubMed: Ashmead chelation
- Firoz M, Graber M. Bioavailability of US commercial magnesium preparations — PubMed: Firoz commercial mag
- Schwalfenberg GK, Genuis SJ. The importance of magnesium in clinical healthcare — PubMed: Schwalfenberg review
Research Papers: Cross-Cutting (Magnesium Status, Glycine Biology)
- DiNicolantonio JJ, O'Keefe JH, Wilson W. Subclinical magnesium deficiency: a principal driver of cardiovascular disease — PubMed: DiNicolantonio Mg deficiency
- Rosanoff A, Weaver CM, Rude RK. Suboptimal magnesium status in the United States — PubMed: US magnesium status
- Costello RB, Elin RJ, Rosanoff A et al. Perspective: the case for an evidence-based reference interval for serum magnesium — PubMed: Mg reference interval
- Workinger JL, Doyle RP, Bortz J. Challenges in the diagnosis of magnesium status — PubMed: Mg status diagnosis
- Wang W, Wu Z, Dai Z et al. Glycine metabolism in animals and humans: implications for nutrition and health — PubMed: Glycine metabolism
- Razak MA et al. Multifarious beneficial effect of nonessential amino acid, glycine: a review — PubMed: Razak glycine review
- Meléndez-Hevia E et al. A weak link in metabolism: the metabolic capacity for glycine biosynthesis does not satisfy collagen demand — PubMed: Glycine biosynthesis gap
- Diaz-Flores M et al. Glycine and glutathione: rate-limiting precursor for redox homeostasis — PubMed: Glycine-glutathione
- Kirkland AE, Sarlo GL, Holton KF. The role of magnesium in neurological disorders — PubMed: Mg in neurology
- Gröber U, Schmidt J, Kisters K. Magnesium in prevention and therapy — PubMed: Gröber Mg review
External Authoritative Resources
- Linus Pauling Institute — Magnesium Micronutrient Information Center — the most authoritative scientific summary of magnesium biology, regularly updated by the Oregon State University micronutrient research group
- NIH Office of Dietary Supplements — Magnesium Fact Sheet (Health Professionals)
- MedlinePlus — Magnesium
- MedlinePlus — Glycine
- ConsumerLab — Magnesium Supplement Reviews (third-party tests of actual products, paywalled but authoritative)
- PubMed — Magnesium glycinate / bisglycinate research
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Magnesium Glycinate (Main Page)
- Magnesium Glycinate for Sleep Quality
- Magnesium Glycinate for Anxiety Relief
- Magnesium Glycinate for Muscle Relaxation
- Magnesium Glycinate Bioavailability
- Magnesium (Mineral Overview)
- Magnesium for Sleep
- Magnesium for Heart Health
- Glycine
- Calcium (Magnesium's Antagonist)
- Potassium
- Anxiety
- Insomnia
- Depression
- Migraine
- Cramp Prevention
- Sleep Hygiene
- Natural Anxiety Relief