Magnesium Glycinate Bioavailability
Magnesium glycinate's clinical superiority comes from its chelate chemistry, not its elemental magnesium content. The molecule is a stable five-membered ring in which two glycine amino-acid carboxylates and amine nitrogens grip a single Mg2+ ion through coordinate covalent bonds — the same chelation pattern that the body itself uses to traffic divalent metals safely through serum. The chelate resists stomach-acid precipitation, escapes the phytate-and-oxalate chelation that bleeds plant-source magnesium into the toilet, bypasses the saturable paracellular-magnesium transport that limits oxide absorption, and is delivered into the enterocyte through dedicated amino-acid transporters. Fractional absorption is approximately 80%, versus 4% for oxide and 30% for citrate. The market consequence is that "magnesium glycinate" became the dominant premium-supplement category of 2024-2026 — and the consumer consequence is a flood of mislabeled product, in which cheap magnesium oxide is buffered with a sprinkle of glycine and sold as bisglycinate. This page walks through the chelate chemistry, the Albion patented process that defined the category, the fractional-absorption comparisons across forms, the saturation kinetics that govern dosing, the difference between true "fully reacted" chelate and oxide-buffered impostors, the third-party certifications (USP, NSF, ConsumerLab) that filter quality, the label red flags to spot inferior products, and how to read a Certificate of Analysis.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- Chelate Chemistry — What "Bisglycinate" Actually Means
- The Albion Patented Process and "Fully Reacted" Chelate
- Fractional Absorption Across Magnesium Forms
- Why Glycinate Absorbs Through Amino-Acid Transporters
- Saturation Kinetics and Why Smaller Divided Doses Work Better
- Oxide-Buffered Impostors and the "Magnesium Complex" Label Trick
- Third-Party Testing — USP, NSF, ConsumerLab
- Label Red Flags That Signal Inferior Product
- How to Read a Certificate of Analysis
- Cost vs Quality — What Premium Pricing Actually Buys
- Cautions and Market Caveats
- Key Research Papers
- Connections
- Featured Videos
Chelate Chemistry — What "Bisglycinate" Actually Means
The term "chelate" comes from the Greek chele, meaning "claw" — an apt metaphor for the geometry. In a metal-amino-acid chelate, the metal ion sits at the center while two or more amino-acid molecules grip it through multiple coordinate covalent bonds, holding the metal in a stable molecular cage. The cage protects the metal from interactions with the surrounding chemistry (acids, bases, competing ions) and keeps the metal soluble at physiological pH.
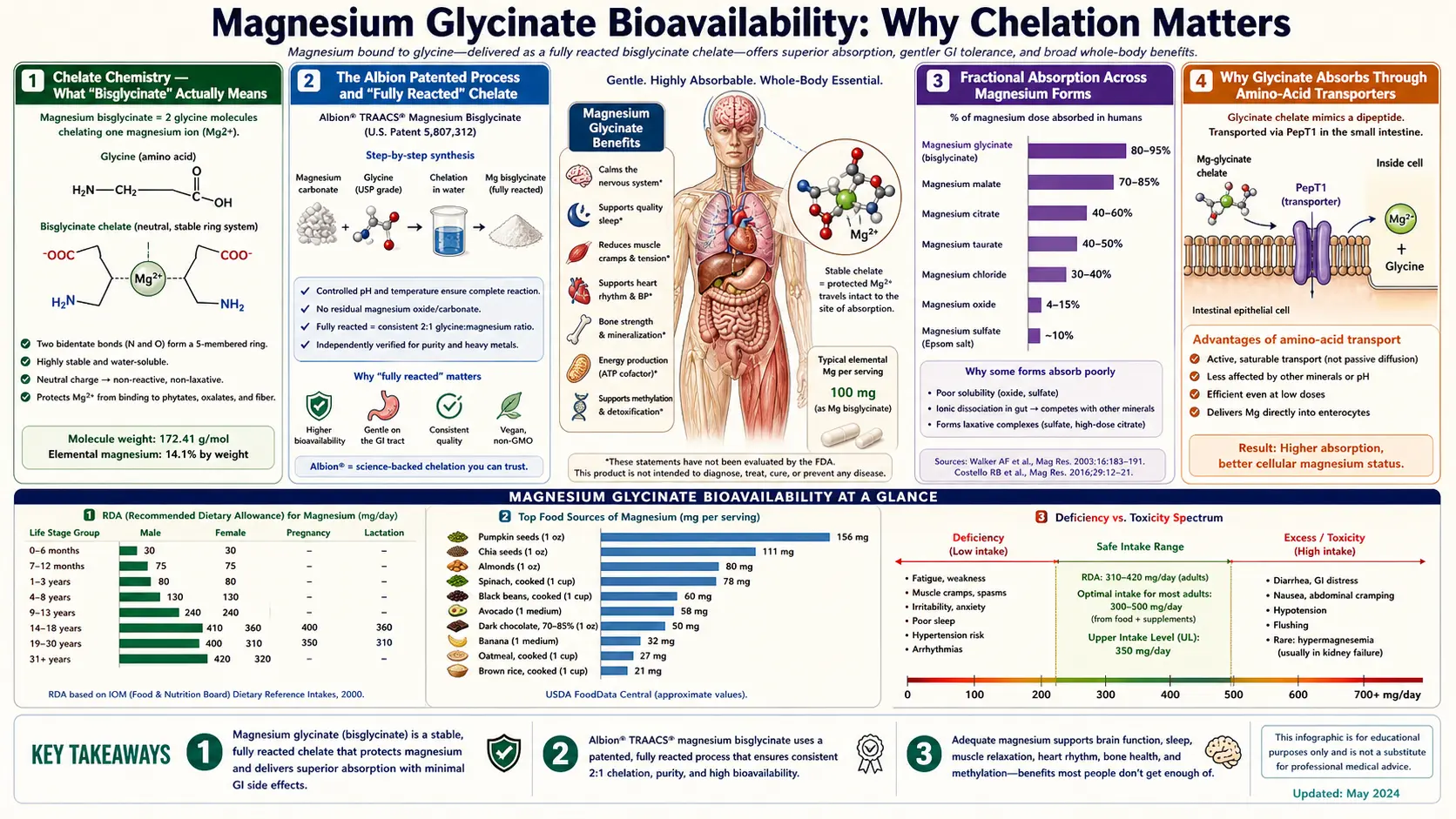
Magnesium bisglycinate (also written magnesium glycinate, magnesium diglycinate, or magnesium glycinate chelate) is a 1:2 metal-to-amino-acid chelate. One Mg2+ ion is held by two glycine molecules. Each glycine contributes two coordination points: the amine nitrogen at one end of the molecule and the carboxylate oxygen at the other end. The geometry produces two five-membered rings (the chelate rings), each containing one glycine's amino nitrogen, the Mg2+ ion, one carboxylate oxygen, and the two carbon atoms of the glycine backbone in between.
This particular ring geometry (five-membered chelate rings with N and O as donor atoms) is thermodynamically very stable — what coordination chemists call the "chelate effect." The chelate is more stable than either glycine alone with magnesium or magnesium with any single monodentate (one-bond) ligand. The stability constant Kf for the bisglycinate chelate is high enough that the chelate persists through stomach acid (where most loose Mg2+-anion ion pairs would dissociate) and through the small intestinal pH transition.
The elemental magnesium content of the chelate is approximately 14% by weight. A 1000 mg dose of magnesium bisglycinate compound therefore contains approximately 140 mg of elemental magnesium and approximately 860 mg of glycine (two glycine molecules per Mg, each 75 g/mol, times the per-molecule weight ratio). When label nutrition facts read "Magnesium (as Magnesium Bisglycinate) 140 mg," that 140 mg is the elemental content, not the compound weight — the actual chelate weight is the 1000 mg total.
The 14% elemental content is much lower than magnesium oxide (~60% elemental) but the absorption percentage is enormously higher, so the net delivered magnesium per gram of compound is comparable to or better than oxide despite the much lower headline elemental content. This is the source of substantial consumer confusion: oxide labels show large elemental numbers, glycinate labels show small elemental numbers, but the actually-absorbed magnesium tells the opposite story.
The Albion Patented Process and "Fully Reacted" Chelate
Albion Laboratories (now Balchem Albion Minerals, after the 2017 acquisition) is the company that developed the patented manufacturing process for fully-reacted amino-acid chelates that defined the category in the 1990s-2000s. The Albion process uses controlled-pH, controlled-temperature, controlled-ratio reaction of magnesium oxide with glycine in solution to drive the equilibrium toward the chelate product and away from the unreacted starting materials.
"Fully reacted" is the marketing term for a chelate in which the great majority of the magnesium present is bound in the bisglycinate ring structure, rather than existing as a physical mixture of magnesium oxide and free glycine. The verification methods include FTIR (Fourier-transform infrared spectroscopy) showing the characteristic chelate absorption peaks, NMR showing the expected coordination environment, and bench-stability tests showing the chelate survives expected gut conditions.
Albion holds (or held; some patents have expired) several patents covering specific reaction conditions, the resulting molecular structures, and the use of fully-reacted chelates in nutritional products. The "TRAACS" trademark (The Real Amino Acid Chelate System) and the Albion logo on a finished product label historically indicated genuine Albion-produced chelate. Many premium supplement brands source their bisglycinate from Albion specifically for this reason and feature the TRAACS / Albion logo prominently.
Since the foundational Albion patents began expiring, several competitor manufacturers have developed their own chelate processes (Jost Chemical, Gnosis by Lesaffre, and Aldrich/Sigma among them), and some Asian manufacturers produce lower-cost chelates of variable quality. The premium consumer market still treats Albion / TRAACS as the gold standard, but the practical question for any specific product is whether it is genuinely fully-reacted chelate, regardless of the original manufacturer.
Distinguishing fully-reacted chelate from oxide-buffered-with-glycine is the central quality question and is discussed in detail in the Oxide-Buffered Impostors section below.
Fractional Absorption Across Magnesium Forms
The published fractional absorption data across magnesium forms varies somewhat by study methodology (urinary recovery vs serum kinetics vs isotope tracer studies), but the rank-ordering is consistent:
- Magnesium oxide (MgO) — ~4% fractional absorption. The lowest of the commonly-sold forms. The Firoz and Graber 2001 trial measuring urinary magnesium recovery after oral magnesium found oxide produced significantly less urinary magnesium than citrate, chloride, or lactate, indicating less actually-absorbed magnesium. Oxide's high elemental percentage (~60% Mg by weight) creates the illusion of high magnesium delivery per dose, but the absorption percentage so low that net systemic delivery is poor.
- Magnesium sulfate (Epsom salt) — ~7% oral fractional absorption. Limited utility as an oral supplement; mostly used topically (bath soaks, where transdermal absorption is debated) or as an IV form for emergency hypomagnesemia.
- Magnesium hydroxide (milk of magnesia) — ~15-20% absorption. Better than oxide but still relatively poor. Primarily used as antacid and osmotic laxative rather than as a magnesium repletion supplement.
- Magnesium citrate — ~30% absorption. The Walker et al. 2003 randomized double-blind crossover trial in healthy volunteers found citrate produced significantly higher serum and urinary magnesium responses than oxide or aspartate at equivalent elemental doses. Reasonable absorption, but the citrate produces an osmotic laxative effect at sustained therapeutic doses that limits patient adherence.
- Magnesium lactate — ~40% absorption. Better tolerated than citrate, modestly higher absorption. Less commonly available as a standalone product.
- Magnesium chloride — ~50% absorption. Well-absorbed, but the very bitter taste makes it unpalatable as an oral supplement at therapeutic doses. More commonly used in transdermal preparations or in clinical IV forms.
- Magnesium glycinate (bisglycinate chelate) — ~80% absorption (some sources cite 70-90%). The Schuette 1994 trial in patients with ileal resection (a population with substantially impaired magnesium absorption) found diglycinate produced significantly higher absorption than oxide. Subsequent comparative trials in healthy volunteers have consistently shown glycinate at or near the top of the fractional-absorption rankings.
- Magnesium L-threonate — ~75% oral absorption, plus the only form with measurable blood-brain barrier penetration. The CNS targeting is the niche; for systemic muscle / cardiovascular applications, glycinate matches the absorption at much lower cost.
- Magnesium taurate — ~60-70% absorption. Reasonable; the taurine component has independent cardiovascular and anxiolytic benefits.
- Magnesium malate — ~60-70% absorption. Comparable to taurate; malate component supports Krebs cycle energy production.
The Blancquaert, Vervaet, and Derave 2019 paper in Nutrients titled "Predicting and Testing the Bioavailability of Magnesium Supplements" is the most-cited modern synthesis of the bioavailability comparison work. They note that the absorption-percentage differences are real but the elemental-content differences also matter (oxide's 60% elemental Mg vs glycinate's 14% elemental Mg), and the net systemic delivery per gram of compound is the practically relevant metric. By that net metric, glycinate still wins comfortably over oxide and is approximately tied with citrate, with the major glycinate advantage being tolerability rather than absorption per se.
Why Glycinate Absorbs Through Amino-Acid Transporters
The mechanistic explanation for glycinate's superior absorption is that the chelate is taken up by enterocytes through different transport pathways than the loose Mg2+ ion. Free magnesium absorption in the small intestine uses two routes: the TRPM6 / TRPM7 channels (specific magnesium transporters in the apical membrane of enterocytes), which are easily saturated at modest luminal magnesium concentrations, and paracellular diffusion through the tight junctions between enterocytes, which depends on the magnesium concentration gradient and is also limited.
The intact bisglycinate chelate bypasses both of these saturable routes. Instead, it appears to be taken up through amino-acid transport systems — particularly the PEPT1 oligopeptide transporter and the various neutral amino-acid transporters that handle glycine and small peptides. These transporters have much higher capacity than the magnesium-specific routes and are not significantly saturated at typical supplemental magnesium doses.
Once inside the enterocyte, the chelate dissociates as intracellular pH conditions and the much lower chelate stability inside the cell (relative to the bulk intestinal lumen) favor dissociation into free Mg2+ and free glycine. The free Mg2+ then exits the basolateral side of the enterocyte through Mg2+-specific transporters into portal blood, while the free glycine joins the enterocyte's amino-acid pool and either is used locally or exits to portal blood for systemic delivery.
The practical implication is that glycinate avoids the competition with dietary phytates (in whole grains and legumes), oxalates (in spinach, beet greens, rhubarb), and tannins (in tea and coffee) that bleeds substantial magnesium from oxide and other free-Mg2+-forming supplements. Phytates and oxalates chelate Mg2+ in the gut lumen and prevent absorption. The bisglycinate chelate is already chelated, by glycine, with a higher stability constant than the phytate-Mg2+ complex, so the dietary chelators cannot displace the glycine.
This is also why glycinate can be taken with food or away from food with similar absorption, while oxide and citrate are more dose-dependent on what else is in the gut at the same time. The chelate is "armored" against the chemistry around it.
Saturation Kinetics and Why Smaller Divided Doses Work Better
Even with the favorable amino-acid-transporter absorption mechanism, magnesium absorption is not unlimited. As the luminal magnesium concentration rises, the fractional percentage absorbed falls — classic saturation kinetics. A single 800 mg dose of compound does not deliver twice as much absorbed magnesium as two 400 mg doses given several hours apart, because the transporters are more saturated by the single large bolus.
The practical consequence is that dividing the daily magnesium dose into two or three smaller doses typically delivers somewhat more total systemic magnesium than a single large daily dose of the same total compound weight. The Coudray et al. 2005 paper in Magnesium Research studied this with isotope-tracer methodology and showed that smaller, divided doses produced higher net retention over 24 hours than equivalent total amounts given as a single bolus.
For most adults, the practical sweet spot is two doses per day (morning and evening), each of 200-400 mg of compound. Three doses per day (with meals) marginally improves absorption further but adds compliance burden. Single daily dosing is acceptable when convenience is paramount, but should weight the compound at the higher end (400-600 mg of compound in one dose) to compensate for the saturation kinetics.
For applications targeting a specific time-of-day effect (sleep-onset, bedtime cramp prevention), a single evening dose at 300-400 mg of compound is the standard, and the absorption is adequate for the intended effect. The dosing-frequency optimization matters more for chronic repletion of severe deficiency, where maximum total systemic delivery is the goal.
Another saturation-related principle: the body's magnesium-handling kinetics include renal excretion of excess. The kidneys excrete approximately 90-95% of any acutely-administered oral magnesium load that exceeds the body's real-time tissue uptake capacity. This is what makes oral magnesium so safe in healthy kidneys — the excess just goes in the urine. It also means that "more is not better" beyond a certain dose threshold; the additional grams of compound mostly produce additional urinary magnesium without additional tissue benefit.
Oxide-Buffered Impostors and the "Magnesium Complex" Label Trick
The most common quality problem in the magnesium glycinate market is the practice of labeling a product as "magnesium glycinate" when the actual product is mostly magnesium oxide with a small amount of glycine added to it — sometimes called "buffered magnesium oxide" or "oxide-with-glycine." The product is much cheaper to manufacture than fully-reacted bisglycinate chelate, but it lacks the chelate's pharmacokinetic and tolerability advantages.
The label trick works because US dietary-supplement labeling rules do not currently require manufacturers to verify or disclose what percentage of the magnesium is actually in the chelate form versus what percentage is unreacted oxide. A product can legally call itself "magnesium glycinate" or "magnesium bisglycinate" as long as some of the magnesium is in chelate form. There is no minimum threshold; a product that is 95% oxide and 5% bisglycinate can carry the bisglycinate label.
Telltale signs of an oxide-buffered impostor:
- High elemental magnesium per capsule — if a single capsule is labeled "Magnesium 400 mg (as magnesium glycinate)," it almost certainly contains substantial oxide. True bisglycinate chelate is only 14% elemental magnesium, so a 400 mg elemental dose would require nearly 2.9 grams of pure chelate per capsule — impractical to encapsulate. Real bisglycinate products typically show "100-200 mg elemental Mg per capsule" at most, with patients taking 2-3 capsules per day for therapeutic dosing.
- The phrase "magnesium oxide" appearing anywhere on the ingredient list — some products honestly disclose the buffering by listing both compounds. If oxide is in the ingredients, the product is not pure bisglycinate.
- The phrase "magnesium complex" or "magnesium blend" on the front of the label — these vague terms often disguise an oxide-heavy mixture sold at glycinate prices.
- "Buffered magnesium glycinate" or "magnesium glycinate buffered with magnesium oxide" — the more honest disclosure label, but still indicates a substantial fraction is oxide.
- Loose-stool side effects at moderate doses — the most empirical test. Real fully-reacted bisglycinate rarely causes loose stools at 300-400 mg of compound. If a "glycinate" product reliably loosens stools at modest doses, the oxide content is likely high.
- Suspiciously low price — fully-reacted Albion-grade chelate costs the supplement manufacturer several-fold more than oxide. A 120-capsule bottle of legitimate Albion-sourced bisglycinate retails around $20-30. A "glycinate" bottle at $8-10 is likely an oxide blend.
The honest manufacturers disclose specifically: "Magnesium (as TRAACS® Magnesium Bisglycinate Chelate Buffered)" or "Magnesium (as Magnesium Bisglycinate Chelate, fully reacted)" or the unambiguous statement "100% magnesium bisglycinate chelate; no magnesium oxide." Products that disclose explicitly tend to deliver what they claim; products that use vague "magnesium glycinate" language without a fully-reacted or TRAACS qualifier are more likely to be oxide-heavy.
Third-Party Testing — USP, NSF, ConsumerLab
The single best filter for identifying a high-quality magnesium glycinate product is third-party certification or testing by an independent organization that has no financial interest in selling the product. The major third-party programs in the US market:
- USP (United States Pharmacopeia) Verified Mark — the most rigorous and most expensive certification. USP verifies that the product contains the ingredients listed on the label in the amounts listed, that contaminants are below specified thresholds (lead, arsenic, cadmium, mercury, pesticides, microbiologicals), and that the product was manufactured under cGMP standards. The USP mark is reliable but uncommon on supplement labels because the cost of certification deters many manufacturers.
- NSF International Certified for Sport — rigorous certification originally developed for athletes to verify supplements are free of banned substances. The NSF Certified for Sport mark on a magnesium glycinate product is a strong quality signal. NSF's standard NSF/ANSI 173 also verifies supplement composition and contaminant limits for the general supplement market.
- ConsumerLab.com — an independent testing organization that purchases supplements anonymously off retail shelves and tests them for label accuracy, contaminants, and disintegration. ConsumerLab publishes test results for subscribers; the published reports are widely used in integrative medicine as a screening tool. ConsumerLab regularly tests magnesium supplements and identifies products that fail label-accuracy or contaminant tests.
- Informed Choice / Informed Sport — certifications focused on athletic supplements, verifying freedom from WADA-banned substances. Useful for athletes specifically.
- cGMP (Current Good Manufacturing Practice) — the basic regulatory requirement for supplement manufacturing in the US. All legal US supplement products must claim cGMP compliance, but the FDA does not pre-approve products or inspect every facility, so a cGMP claim alone is the floor of acceptability rather than an indicator of premium quality.
The practical recommendation: prefer products with USP Verified Mark, NSF certification, or ConsumerLab approval. Among premium brands without those certifications but with a strong reputation, look for the TRAACS / Albion logo or explicit "fully reacted" language plus published Certificate of Analysis on the manufacturer's website.
Label Red Flags That Signal Inferior Product
Concrete things to look for when evaluating a magnesium glycinate product:
- RED FLAG: "Magnesium 400 mg per capsule" — physically impossible from pure bisglycinate. Indicates oxide content.
- RED FLAG: Magnesium oxide listed anywhere in ingredients — not pure bisglycinate.
- RED FLAG: Vague labeling like "magnesium blend," "magnesium complex," "buffered magnesium" — obscures the actual form.
- RED FLAG: No specification of which chelate process or supplier was used — legitimate manufacturers proudly disclose TRAACS / Albion or equivalent. Generic "magnesium glycinate" with no chelate-source qualifier often means commodity-grade Asian chelate of variable quality.
- RED FLAG: Excessive fillers and excipients — titanium dioxide (a controversial colorant), excessive magnesium stearate (a flow agent), artificial colors, hydrogenated oils, large amounts of cellulose. Premium products use minimal excipients.
- RED FLAG: No Certificate of Analysis available — a manufacturer that won't share testing results for the specific lot you're buying is hiding something. Legitimate premium manufacturers post COAs by lot number on their websites.
- RED FLAG: Suspiciously low price — if a 120-capsule bottle of "magnesium glycinate" retails under $10, the math doesn't work for pure chelate. Probably oxide-buffered.
- GREEN FLAG: TRAACS® / Albion logo — indicates Albion-supplied chelate, the historical gold standard.
- GREEN FLAG: USP Verified, NSF Certified for Sport, or ConsumerLab approval — the strongest independent quality verification.
- GREEN FLAG: Explicit "fully reacted bisglycinate chelate" language — manufacturer is differentiating from oxide-buffered impostors.
- GREEN FLAG: 100-200 mg elemental Mg per capsule, with 2-3 capsules suggested for daily dose — consistent with pure chelate's 14% elemental content.
- GREEN FLAG: Short, transparent ingredient list — just bisglycinate plus capsule shell, ideally.
- GREEN FLAG: Published COA available by lot number — manufacturer transparent about testing.
How to Read a Certificate of Analysis
A Certificate of Analysis (COA) is a lab-test document showing what the manufacturer actually verified about a specific batch of product. Legitimate premium manufacturers make COAs available either on the product website (often searchable by lot number printed on the bottle) or by request. The key sections to check:
- Lot number — must match the lot number printed on the bottle you bought. A "generic" COA not tied to a specific lot is much weaker than a lot-specific COA.
- Active ingredient assay — the actual measured elemental magnesium content per serving, compared to the label claim. Should be within 5-10% of label claim. Substantial under-delivery (40% of claim) is a serious quality problem; over-delivery within reasonable bounds is acceptable.
- Heavy metal testing — lead, arsenic, cadmium, mercury. Limits vary by jurisdiction; the California Proposition 65 limits are stricter than federal standards. Look for "below detection limit" or quantitative results well below the regulatory threshold for each metal. Heavy metal contamination in mineral supplements is the single most consequential quality issue.
- Microbial testing — total aerobic plate count, yeast, mold, E. coli, Salmonella. Should be below specified thresholds.
- Identity testing — FTIR or NMR confirmation that the product is genuinely the bisglycinate chelate, not oxide masquerading. This is the section that distinguishes "real" from "buffered impostor."
- Disintegration / dissolution test — the capsule must actually break down and release the contents in simulated gastric and intestinal conditions within a specified time. Poorly-manufactured products can pass through the GI tract intact, delivering essentially nothing.
- Date of testing — should be recent, ideally within a year of the manufacturing date. Very old COAs (5+ years) being recycled for new product lots is a warning sign.
- Testing laboratory — should be an independent lab, not the manufacturer's in-house lab. Look for ISO 17025 accreditation.
Most consumers will not need to read a COA for every supplement purchase, but for high-quality magnesium glycinate at therapeutic doses taken for years, spending 10 minutes verifying the COA for a specific brand is reasonable due diligence. The manufacturers who make COAs easy to find are generally the ones who have nothing to hide.
Cost vs Quality — What Premium Pricing Actually Buys
The retail cost spread between bargain-bin and premium magnesium glycinate is large — sometimes 5-10x. The premium price tag buys real things:
- Genuinely fully-reacted bisglycinate chelate rather than oxide-buffered impostors. The single most consequential quality difference.
- Albion / TRAACS sourcing with the patent-process quality control behind it.
- Independent third-party testing (USP, NSF, ConsumerLab) verifying label accuracy and contaminant freedom.
- Lower heavy-metal contamination — mineral supplements vary substantially in heavy-metal load depending on the magnesium source rock and the refining process. Premium products tend to use cleaner source materials.
- Better disintegration — capsules that actually break down and deliver contents reliably.
- Minimal fillers and excipients — cleaner ingredient lists with fewer additives.
- Transparent COA disclosure — the manufacturer's willingness to be scrutinized.
That said, "premium" is not synonymous with "best." Some mid-tier products from honest mid-tier manufacturers deliver excellent fully-reacted chelate at moderate prices. Pure Encapsulations, Thorne, Designs for Health, NOW Foods' verified bisglycinate line, Klaire Labs, Metagenics, Doctor's Best, and Jarrow Formulas (with the TRAACS-disclosed magnesium glycinate specifically) are examples of brands with consistently good track records at various price points. Brand-name recognition without quality verification is not the same as actual quality — some heavily-marketed brands skimp on chelate purity to fund marketing.
The most cost-effective strategy is usually: pick a mid-tier brand with explicit "fully reacted bisglycinate" labeling, TRAACS or USP/NSF/ConsumerLab verification, and reasonable price-per-dose math (around $0.20-0.40 per 100 mg elemental magnesium delivered), and stay with that brand long-term unless quality concerns arise.
Cautions and Market Caveats
- Regulatory landscape — the FDA regulates dietary supplements under DSHEA (1994), which is much less strict than prescription drug regulation. The FDA does not pre-approve supplements, does not verify label accuracy before market entry, and only intervenes when adverse events or specific complaints accumulate. This regulatory gap is what makes third-party certification valuable.
- "Structure / function" claims — supplement labels can legally claim a product "supports relaxation," "supports sleep," "supports muscle function." They cannot legally claim it "treats anxiety" or "cures insomnia" without FDA drug approval. The asymmetry leaves consumers to translate vague structure / function claims into clinical applications, which is part of why this site exists.
- International products — supplements imported from outside the US may not meet US labeling standards. European and Australian regulatory frameworks differ from the US; Asian-manufactured supplements (especially those bought through Amazon resellers from unidentified manufacturers) have variable quality and may contain undisclosed contaminants.
- Amazon marketplace caveat — counterfeit and adulterated supplements appear regularly in the Amazon ecosystem. Buying through Amazon "ships and sold by Amazon" or directly from the brand's manufacturer-verified storefront reduces (but doesn't eliminate) this risk. Third-party Amazon sellers are higher risk.
- "Magnesium spray" and topical products — transdermal magnesium absorption is debated. Some patients find topical magnesium oil useful adjunctively, but for systemic repletion oral bisglycinate is much more reliable.
- Liquid and powder magnesium glycinate — flavored powders and liquid forms exist. Quality varies; the key verification questions are the same as for capsule products (fully reacted, third-party tested, transparent COA).
- Storage conditions — bisglycinate is stable at room temperature in dry conditions but should be protected from heat, moisture, and direct light. Don't store in a hot car or humid bathroom long-term.
- Expiration dates — legitimate products list a "best by" date. The bisglycinate molecule is stable for years if properly stored; the date is typically conservative.
Key Research Papers
- Blancquaert L, Vervaet C, Derave W (2019). Predicting and testing bioavailability of magnesium supplements. Nutrients. — PubMed
- Schuette SA, Lashner BA, Janghorbani M (1994). Bioavailability of magnesium diglycinate vs magnesium oxide in patients with ileal resection. JPEN Journal of Parenteral and Enteral Nutrition. — PubMed
- Walker AF, Marakis G, Christie S, Byng M (2003). Mg citrate found more bioavailable than other Mg preparations in a randomised, double-blind study. Magnesium Research. — PubMed
- Lindberg JS, Zobitz MM, Poindexter JR, Pak CY (1990). Magnesium bioavailability from magnesium citrate and magnesium oxide. Journal of the American College of Nutrition. — PubMed
- Firoz M, Graber M (2001). Bioavailability of US commercial magnesium preparations. Magnesium Research. — PubMed
- Coudray C, Rambeau M, Feillet-Coudray C et al. (2005). Study of magnesium bioavailability from ten organic and inorganic Mg salts in Mg-depleted rats using a stable isotope approach. Magnesium Research. — PubMed
- Ashmead HD. Conversations on chelation and mineral nutrition. (Albion chelate mechanism reference text) — PubMed
- Ranade VV, Somberg JC (2001). Bioavailability and pharmacokinetics of magnesium after administration of magnesium salts to humans. American Journal of Therapeutics. — PubMed
- Workinger JL, Doyle RP, Bortz J (2018). Challenges in the diagnosis of magnesium status. Nutrients. — PubMed
- Costello RB, Elin RJ, Rosanoff A et al. (2016). Perspective: the case for an evidence-based reference interval for serum magnesium. Advances in Nutrition. — PubMed
- Rosanoff A, Weaver CM, Rude RK (2012). Suboptimal magnesium status in the United States: are the health consequences underestimated? Nutrition Reviews. — PubMed
- Schwalfenberg GK, Genuis SJ (2017). The importance of magnesium in clinical healthcare. Scientifica. — PubMed
PubMed Topic Searches
- PubMed: Magnesium bisglycinate chelate bioavailability
- PubMed: Magnesium fractional absorption
- PubMed: Amino acid chelate mineral absorption
- PubMed: TRPM6/TRPM7 intestinal Mg transport
- PubMed: Mg supplement contamination
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Magnesium Glycinate Overview
- Magnesium Glycinate Benefits Hub
- Magnesium Glycinate for Sleep
- Magnesium Glycinate for Anxiety
- Magnesium Glycinate for Muscle Relaxation
- Magnesium (Overview)
- Magnesium for Sleep
- Magnesium for Heart Health
- Glycine
- Calcium
- Zinc (Chelate Comparison)
- Iron (Chelate Comparison)
- Lab Tests
- Heavy Metals
- Cramp Prevention