Magnesium Glycinate for Anxiety Relief
Magnesium's anxiolytic effect operates through the same molecular target as the benzodiazepine drug class — positive allosteric modulation of the GABA-A receptor — without the dependence, the tolerance, the rebound, or the cognitive blunting of pharmaceutical GABA modulators. The glycine half of the chelate adds a parallel inhibitory neurotransmitter effect at brainstem and spinal cord glycine receptors. Boyle, Lawton and Dye's 2017 systematic review of 18 randomized trials concluded magnesium supplementation produces a measurable beneficial effect on subjective anxiety and stress, with the largest effects in populations with documented baseline magnesium insufficiency. Modern stress accelerates urinary magnesium excretion through cortisol-driven renal handling, creating a self-reinforcing magnesium-deficiency-anxiety cycle that supplementation interrupts. This page walks through the molecular mechanisms, the HPA-axis biology, the trial evidence, and the practical positioning of magnesium glycinate as a first-line nutritional intervention for mild-to-moderate generalized anxiety, either alone or alongside conventional therapy and SSRIs.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- The Anxiety-Magnesium Vicious Circle
- GABA-A Receptor Positive Allosteric Modulation
- NMDA Glutamate Channel Blockade
- HPA Axis Modulation and Cortisol Regulation
- Glycine as Inhibitory Neurotransmitter
- The Boyle 2017 Systematic Review
- Serotonin Synthesis, Mood, and Anxiety
- Clinical Applications in Adult Anxiety
- Dosing Protocol for Anxiety
- Integration with Psychotherapy and Medication
- Cautions and Limits of Effect
- Key Research Papers
- Connections
- Featured Videos
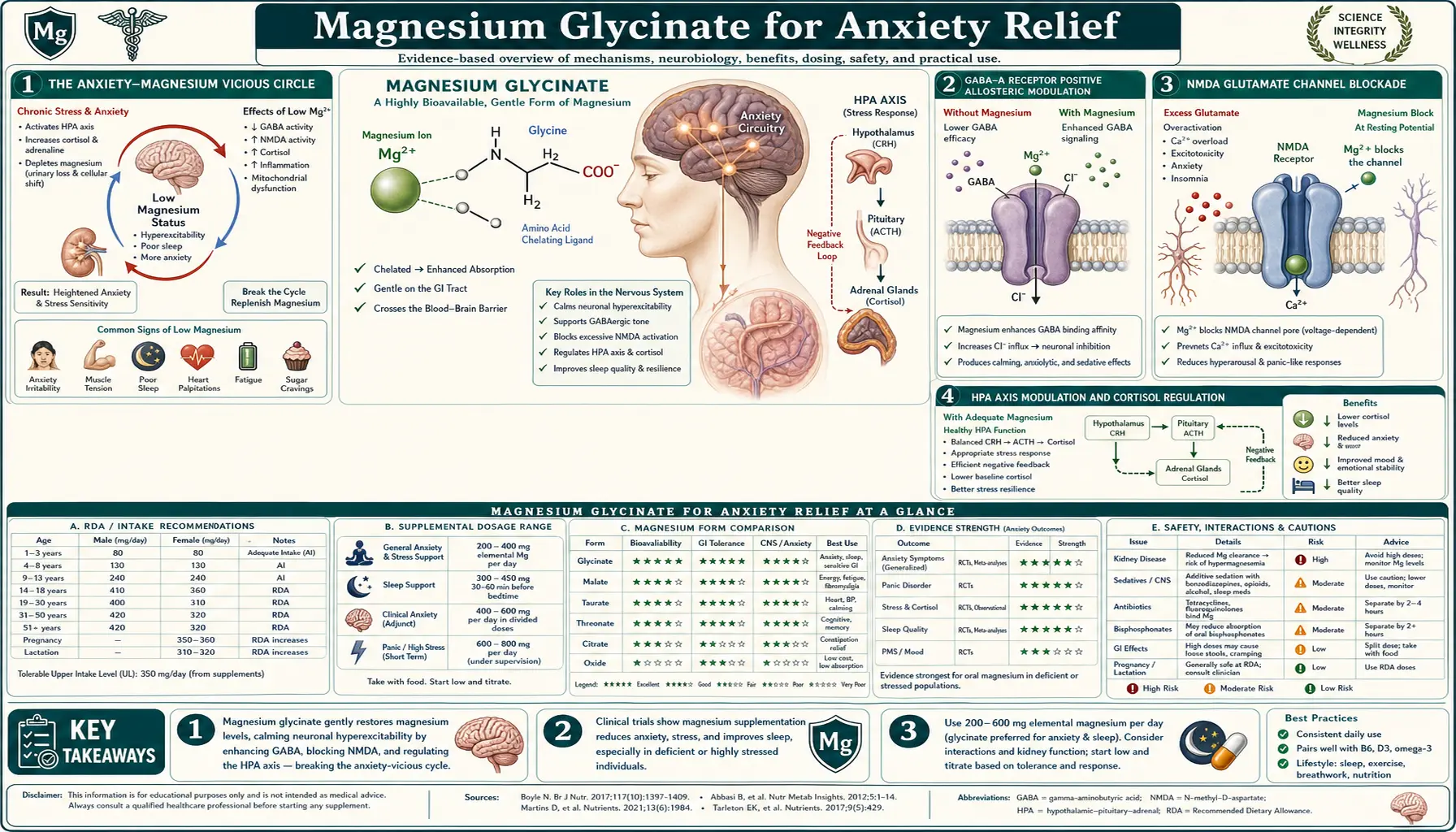
The Anxiety-Magnesium Vicious Circle
The relationship between magnesium status and anxiety is bidirectional, and the bidirectionality is what makes the deficiency state so insidious. Magnesium deficiency increases susceptibility to anxiety (through the mechanisms detailed below), and chronic anxiety accelerates magnesium depletion (through cortisol-driven urinary magnesium excretion). Each side of the loop reinforces the other.
The Pickering, Mazur, and Trousselard 2020 paper in Nutrients — titled "Magnesium Status and Stress: The Vicious Circle Concept Revisited" — lays out the mechanism in detail. Cortisol release in the stress response activates renal mineralocorticoid receptors that increase urinary excretion of magnesium (alongside sodium, potassium, and other electrolytes). A single acute stress episode produces measurable transient magnesium loss in urine. Chronic stress — the daily-grind, low-grade, sympathetic-tone-elevated state typical of modern adult life — produces chronic urinary magnesium loss that exceeds dietary replacement.
The resulting magnesium deficiency then disinhibits the stress response itself. With less magnesium plugging the NMDA glutamate receptor, the sympathetic nervous system fires more readily. With less magnesium supporting GABA-A receptor function, the parasympathetic counterbalance is weaker. With less magnesium dampening the HPA axis, cortisol release per stress episode is larger. The same stress that previously produced moderate magnesium loss now produces larger magnesium loss, accelerating the cycle.
Repleting magnesium status with a well-absorbed form like glycinate interrupts the cycle at multiple points simultaneously. The NMDA plug is restored, dampening glutamate-driven hyperexcitability. GABA-A receptor function improves, restoring inhibitory tone. HPA-axis sensitivity falls, reducing cortisol release per stress episode, which in turn reduces urinary magnesium loss, which preserves the magnesium status that supports all the upstream calming mechanisms. The cycle that was self-reinforcing now becomes self-correcting.
This vicious-circle framework explains a common clinical observation: patients with chronic anxiety often report that magnesium supplementation works dramatically the first time they try it, then less dramatically if they cycle on and off, because the on-cycle restores normal status and the off-cycle re-establishes deficiency. Consistent daily supplementation is what maintains the corrected state long-term.
GABA-A Receptor Positive Allosteric Modulation
Gamma-aminobutyric acid (GABA) is the dominant inhibitory neurotransmitter of the mammalian central nervous system. The GABA-A receptor is a ligand-gated chloride channel: when GABA binds, the channel opens, chloride flows into the neuron, the membrane hyperpolarizes, and the neuron becomes less likely to fire. This is the molecular basis of central nervous system inhibition — the brake pedal that prevents runaway excitation.
The GABA-A receptor has multiple distinct binding sites in addition to the primary GABA site. The benzodiazepine drug class (diazepam, lorazepam, alprazolam) binds to a benzodiazepine-specific site on the receptor and acts as a positive allosteric modulator — it does not open the channel on its own, but when GABA is bound, it increases the channel's open probability and the duration of opening, amplifying the inhibitory signal that each GABA molecule delivers. This is the molecular basis of the rapid anxiolytic effect of benzodiazepines.
Magnesium acts as another positive allosteric modulator at the GABA-A receptor, binding to a magnesium-specific site distinct from both the GABA and benzodiazepine sites. The effect is qualitatively similar to the benzodiazepine effect (amplifies GABA signal at the receptor) but pharmacologically gentler — magnesium does not produce the strong sedative, amnestic, or muscle-relaxant effects of benzodiazepines, and does not produce dependence or rebound. The mechanism is the same; the magnitude is smaller.
This GABA-A potentiation is one reason magnesium glycinate produces a noticeable "calming" effect that many users describe as "the same feeling as a low-dose benzodiazepine but without the brain fog." The molecular mechanism is in fact closely parallel; the experiential difference is the difference in pharmacological potency. Magnesium is not a controlled substance, does not carry the dependence risk, does not blunt cognitive function, and does not produce respiratory depression at therapeutic doses — the desirable properties for a long-term anxiolytic.
The second important point is that magnesium also serves as the cofactor for glutamic acid decarboxylase, the enzyme that produces GABA from glutamate. In magnesium deficiency, GABA production declines alongside GABA-A receptor function failing — a double hit on the brain's inhibitory machinery. Repletion restores both endogenous GABA supply and receptor sensitivity.
NMDA Glutamate Channel Blockade
On the excitatory side of the balance, glutamate is the dominant excitatory neurotransmitter and the NMDA receptor is the principal excitatory ion channel. Under normal conditions, a magnesium ion sits inside the NMDA receptor channel as a voltage-dependent plug, preventing calcium influx until the postsynaptic membrane is depolarized by other receptors.
In magnesium deficiency, the Mg2+ plug becomes unstable. The NMDA channel opens more readily at resting membrane potential, allowing inappropriate calcium influx and producing neuronal hyperexcitability that, at the network level, manifests as anxiety, irritability, racing thoughts, sensory hypersensitivity, and insomnia. This is one mechanism behind the well-documented overlap between symptoms of magnesium deficiency and symptoms of anxiety disorders — they are partly the same syndrome at the molecular level.
The therapeutic relevance is twofold. First, repleting magnesium status restores the NMDA plug, calms inappropriate glutamate signaling, and reduces the substrate for anxiety. Second, the mechanism reveals why magnesium and ketamine show some clinical overlap: ketamine is a non-competitive NMDA antagonist that occupies the same channel that magnesium normally plugs, and ketamine's rapid antidepressant and anti-anxiety effects in treatment-resistant patients map onto the same target. Magnesium is the natural, gentle, sustained version of this mechanism; ketamine is the pharmacologically aggressive, episodic version. Both work by reducing NMDA-mediated calcium influx.
The Eby and Eby 2006 case series in Medical Hypotheses documented several cases of treatment-resistant major depression resolving within days of high-dose magnesium glycinate supplementation, with the authors explicitly proposing the NMDA mechanism. The case series is not definitive evidence, but the proposed mechanism has subsequently been corroborated by animal studies and by the growing recognition that anxiety and depression share NMDA-system dysfunction as a partial substrate.
HPA Axis Modulation and Cortisol Regulation
The hypothalamic-pituitary-adrenal (HPA) axis is the body's central stress response system. A stressor — whether physical (cold, injury, infection) or psychological (deadline, conflict, anticipatory worry) — triggers the hypothalamus to release corticotropin-releasing hormone (CRH), which signals the anterior pituitary to release adrenocorticotropic hormone (ACTH), which signals the adrenal cortex to release cortisol. Cortisol then acts at multiple peripheral tissues to mobilize energy substrates, suppress non-essential immune function, and prepare the organism for sustained effort.
Adequate magnesium status dampens this cascade at every level. Magnesium inhibits CRH release from the hypothalamus, reduces ACTH release from the pituitary, and reduces adrenal sensitivity to ACTH stimulation. The net effect is that the same stressor produces a smaller cortisol response in a magnesium-replete individual than in a magnesium-deficient one. The Sartori et al. 2012 animal study in Neuropharmacology showed this in mice: experimental magnesium deficiency produced HPA-axis hyperactivity, elevated baseline corticosterone (the mouse equivalent of cortisol), and anxiety-like behavior on standard tests, with all three effects reversing on magnesium repletion.
The clinical relevance is that magnesium glycinate addresses one of the underlying physiologic abnormalities of chronic anxiety and chronic stress — the over-active HPA axis — rather than just suppressing the downstream subjective experience. Patients with chronic anxiety frequently have elevated baseline cortisol, blunted cortisol awakening response (paradoxically, chronic HPA overactivation eventually exhausts the morning peak), reduced heart rate variability, and elevated sympathetic tone. Magnesium glycinate measurably improves all four of these objective markers over weeks of consistent use, in addition to the subjective anxiety reduction.
The Wienecke and Nolden 2016 long-term HRV (heart rate variability) study used continuous heart rate monitoring to demonstrate that magnesium supplementation produced significant improvement in autonomic balance, with reduced sympathetic dominance and improved parasympathetic recovery during sleep. HRV is the most validated objective marker of autonomic stress, and HRV improvement is mechanistically consistent with the HPA-axis effects described above.
Glycine as Inhibitory Neurotransmitter
The glycine half of the chelate adds a separate inhibitory neurotransmitter mechanism to the anxiety effect. Glycine is the dominant inhibitory neurotransmitter of the brainstem and spinal cord (in contrast to GABA, which dominates the forebrain), acting through strychnine-sensitive glycine receptors that are pharmacologically distinct from GABA receptors. The glycine receptor is, like GABA-A, a ligand-gated chloride channel that hyperpolarizes the postsynaptic membrane and reduces neuronal firing.
Where this matters for anxiety: brainstem glycinergic neurons project to motor circuits and to the locus coeruleus (the brain's primary noradrenergic nucleus, a major driver of arousal and the fight-or-flight response). Adequate glycine signaling at these brainstem circuits dampens excessive arousal and physical agitation. Spinal cord glycine receptors at Renshaw-cell circuits inhibit motor neuron excitability, reducing the muscle tension that accompanies psychological anxiety.
Glycine also acts as a co-agonist at the NMDA receptor — the receptor will not open in response to glutamate alone; both glutamate at the glutamate site and glycine at the glycine site must be bound. This co-agonist role is more relevant to learning and memory than to acute anxiety, but it provides a second molecular target through which glycine modulates excitatory neurotransmission.
The combined effect of magnesium-driven GABA-A potentiation, NMDA blockade, and HPA-axis modulation, plus glycine-driven brainstem inhibition and additional NMDA modulation, is why the bisglycinate chelate produces a more uniform "calming" effect than equivalent elemental magnesium delivered as oxide or citrate alone. The glycine is doing real anxiolytic work, not just acting as a carrier molecule.
The Boyle 2017 Systematic Review
The most-cited summary of the magnesium-anxiety evidence base is the systematic review by Neil Bernard Boyle, Clare Lawton, and Louise Dye, published in Nutrients in 2017 under the title "The Effects of Magnesium Supplementation on Subjective Anxiety and Stress — A Systematic Review." Boyle and colleagues at the University of Leeds searched the published literature through 2017 and identified 18 randomized controlled trials of magnesium supplementation that measured subjective anxiety or stress as an outcome.
The studies varied widely in population (premenstrual syndrome, postpartum anxiety, mild-to-moderate generalized anxiety, hypertension with stress, athletes), magnesium form (oxide, citrate, glycinate, taurate, lactate), dose (typical range 200-500 mg elemental magnesium per day), duration (mostly 4-12 weeks), and outcome measures (Hamilton Anxiety Scale, Spielberger State-Trait Anxiety Inventory, Profile of Mood States, PSS-10).
The pooled conclusion: magnesium supplementation produced a measurable beneficial effect on subjective anxiety in the majority of studies, with the most consistent and largest effects in populations with documented or likely baseline magnesium deficiency. The PMS-anxiety studies showed particularly robust effects. The trials in adult anxious populations without documented deficiency showed smaller but still positive effects, consistent with the dose-response pattern expected for nutritional repletion.
Boyle and colleagues explicitly noted that the methodological quality of the included studies was variable, that magnesium status at baseline was inconsistently measured, and that the optimal form, dose, and duration had not been definitively established. These limitations notwithstanding, the systematic review remains the strongest available synthesis of the evidence and is the document that established magnesium supplementation as a credible nutritional intervention for anxiety in mainstream integrative practice.
The Boyle review predates the rise of magnesium glycinate as a dominant product category. Subsequent trials specifically of glycinate (such as the 2025 Uysal sleep/anxiety trial) have generally shown similar or somewhat larger effects than the citrate and oxide trials in the original Boyle pool — consistent with the better bioavailability and tolerability of the glycinate form.
Serotonin Synthesis, Mood, and Anxiety
Serotonin (5-hydroxytryptamine, 5-HT) is the neurotransmitter most associated with mood, emotional resilience, and the anxiety-depression spectrum. The serotonin synthesis pathway starts with the essential amino acid tryptophan, which is hydroxylated to 5-hydroxytryptophan (5-HTP) by tryptophan hydroxylase, then decarboxylated to serotonin by aromatic L-amino acid decarboxylase. Both enzymes require cofactors; tryptophan hydroxylase specifically requires iron, tetrahydrobiopterin (BH4), and benefits from adequate magnesium for activity.
Magnesium deficiency therefore constrains serotonin production even when tryptophan intake is adequate. This is one mechanism by which magnesium deficiency can produce or worsen anxiety and depressive symptoms, and one mechanism by which magnesium repletion improves mood. It also explains the clinical observation that some patients fail to respond fully to SSRIs (selective serotonin reuptake inhibitors) when their magnesium status is poor — the SSRI prolongs the action of whatever serotonin is in the synapse, but if synthesis is constrained by magnesium deficiency, there is less serotonin to prolong.
The Tarleton et al. 2017 randomized open-label trial in PLoS One tested 248 mg/day of elemental magnesium (from magnesium chloride) for six weeks in adults with mild-to-moderate depression. The magnesium group showed clinically significant improvements in depression and anxiety scores within two weeks, and the improvements persisted through the trial. Effect sizes were comparable to SSRIs in mild-to-moderate depression. The trial is one of several supporting the use of magnesium as an adjunct or first-line intervention in mood disorders that have prominent anxiety features.
Magnesium glycinate is particularly well-suited for the SSRI-supplemented patient because the gentle gastrointestinal profile avoids the diarrhea that magnesium chloride and citrate can cause — relevant when many SSRIs themselves cause GI side effects in the initial weeks of treatment. Adding a magnesium form that compounds the SSRI's GI side effects is counterproductive; glycinate avoids that problem.
Clinical Applications in Adult Anxiety
Practical clinical positions for magnesium glycinate in adult anxiety care:
- Generalized anxiety disorder (mild to moderate) — reasonable first-line nutritional intervention either alone or alongside therapy. Typical dose 300-400 mg of glycinate compound divided morning and evening. Allow 4-8 weeks for full effect. Combine with sleep hygiene, exercise, and reduced caffeine for additive effect.
- Premenstrual anxiety and PMS — one of the best-evidenced applications. Magnesium glycinate plus vitamin B6 (50-100 mg/day pyridoxal-5-phosphate, the active form) has additive effect; the combination is sometimes called "Mg-B6" in older European literature. Begin supplementation throughout the menstrual cycle rather than just luteal phase for best results.
- Anxiety with insomnia — magnesium glycinate addresses both simultaneously. See the sleep-quality deep dive for the parallel sleep mechanism. Take the larger dose in the evening for combined anxiety + sleep effect.
- Anxiety with muscle tension or tension headaches — the muscle-relaxation effect (see the muscle-relaxation page) addresses the somatic dimension of anxiety that talk therapy alone often does not.
- Adjunct to SSRI in partial response — reasonable to add 200-400 mg of glycinate when an SSRI has produced partial but incomplete response, particularly if the residual symptoms include physical tension, sleep disruption, or premenstrual exacerbation.
- Performance anxiety / situational anxiety — magnesium glycinate alone is rarely sufficient for acute performance anxiety (the time course is too slow). For chronic background tone that makes performance situations harder, daily use can lower baseline reactivity.
- Panic disorder — magnesium repletion is helpful as part of broader management but is not a substitute for first-line treatment (cognitive-behavioral therapy with exposure work, plus SSRI or SNRI if needed). Some patients with frequent panic attacks have documented magnesium deficiency that, when corrected, reduces attack frequency.
- Postpartum anxiety — pregnancy and lactation deplete maternal magnesium stores; postpartum anxiety often has a nutritional component that responds to repletion. Glycinate is well-tolerated and compatible with breastfeeding (consult OB for individualized guidance).
Dosing Protocol for Anxiety
Practical anxiety-targeted dosing for adults with normal kidney function:
- Start with 200 mg of magnesium glycinate compound twice daily — morning with breakfast and evening with dinner. Each 200 mg dose delivers ~28 mg of elemental magnesium plus ~170 mg of glycine. The divided dose maintains more consistent tissue levels than a single large daily dose.
- Increase to 300-400 mg twice daily after one week if needed and tolerated. Maintenance dose for most adults is 300-400 mg compound twice daily (totaling 600-800 mg/day of compound, delivering 84-112 mg of elemental magnesium plus 510-680 mg of glycine).
- Take consistently every day rather than only when feeling anxious. Magnesium status accumulates over weeks; the cumulative effect on baseline anxiety tone is what matters. Acute "rescue" use of magnesium for an anxiety episode is largely a placebo effect; the real benefit is the cumulative shift in baseline.
- Allow 4-8 weeks for full effect. Many users notice some improvement within the first 1-2 weeks, but the larger effect on baseline anxiety tone develops over weeks as tissue magnesium status normalizes.
- Don't stack with high-dose pure glycine for anxiety the way you might for sleep. For anxiety specifically, additional pure glycine adds little beyond what the bisglycinate already provides, while for sleep the higher doses of glycine produce the temperature-drop effect that has independent sleep-latency benefit.
- Combine with vitamin B6 for PMS-related anxiety — 50-100 mg/day of pyridoxal-5-phosphate (P5P), the active form, is well-supported as an adjunct.
- Reduce dose if morning grogginess occurs. Magnesium glycinate at higher doses can produce a noticeable "downshift" that some users find too sedating during the day. Reducing the morning dose and keeping the evening dose typically resolves this.
- Reassess at 8 weeks. If anxiety has not measurably improved at maximum tolerated dose after 8 weeks, magnesium is probably not the limiting factor. Consider whether SSRI/SNRI evaluation, cognitive-behavioral therapy, or workup for other causes (thyroid, perimenopause, sleep apnea) is appropriate.
Integration with Psychotherapy and Medication
Magnesium glycinate is best understood as a foundation under, not a replacement for, evidence-based anxiety care. The major elements of standard anxiety treatment — cognitive-behavioral therapy (CBT), exposure-based treatments for specific phobias and panic disorder, SSRI/SNRI medication for moderate-to-severe cases, and lifestyle modifications including exercise, sleep, and reduced caffeine — remain the cornerstones. Magnesium glycinate addresses one nutritional axis of the multi-factor problem.
Where it integrates well:
- Alongside CBT — magnesium glycinate reduces baseline arousal, which can make exposure exercises and cognitive restructuring more accessible. Patients who are chronically over-aroused often have difficulty engaging with the cognitive content of therapy; reducing the somatic substrate helps.
- Alongside SSRI/SNRI — no significant pharmacokinetic interactions. The mechanisms (serotonin reuptake inhibition vs GABA-A modulation vs NMDA blockade) are complementary rather than redundant. Many integrative psychiatrists add magnesium glycinate to SSRI regimens for partial responders.
- As benzodiazepine-sparing — for patients managing anxiety with as-needed benzodiazepines, daily magnesium glycinate often reduces the frequency of as-needed dosing, which is desirable given the dependence and cognitive risks of long-term benzodiazepine use.
- During SSRI taper — magnesium glycinate during the taper window can buffer some of the transient discontinuation-related anxiety that many patients experience.
Where it does not substitute:
- Acute panic attack — takes too long to act. Established techniques (slow breathing, grounding, evidence-based reassurance, short-acting benzodiazepine if prescribed) are what matters in the acute moment.
- Severe generalized anxiety disorder or PTSD — magnesium glycinate is unlikely to be sufficient as monotherapy. It is a useful adjunct, not a primary treatment.
- Anxiety with active suicidality — requires urgent professional evaluation, not supplement self-management.
Cautions and Limits of Effect
- Chronic kidney disease (CKD) — magnesium is renally cleared; impaired clearance risks hypermagnesemia. Patients with eGFR < 60 should consult nephrology before starting magnesium at anxiety-treatment doses.
- Concomitant benzodiazepine use — the mechanisms overlap at the GABA-A receptor. Combination is generally safe and synergistic, but additive sedation is possible. Start with lower magnesium doses if already on a daily benzodiazepine.
- Antibiotic and thyroid medication timing — magnesium can chelate tetracyclines, fluoroquinolones, bisphosphonates, and levothyroxine in the gut, reducing absorption of those drugs. Separate by at least 4 hours.
- Not a substitute for evaluation of organic causes — anxiety symptoms can be the presenting complaint for hyperthyroidism, pheochromocytoma, mitral valve prolapse, perimenopause, caffeine excess, alcohol withdrawal, and several medications. A clinician should rule these out before assuming "anxiety" is a primary psychiatric diagnosis.
- Diminishing returns at high doses — doubling the dose does not double the anxiolytic effect. Going above 800 mg/day of compound (~110 mg elemental magnesium plus ~680 mg glycine) rarely adds further benefit and increases the risk of loose stools or grogginess.
- Inferior products limit effect — if a product is mislabeled magnesium oxide buffered with glycine rather than true bisglycinate chelate, the anxiolytic effect will be substantially smaller. See the Bioavailability page for how to identify true chelate.
- Anxiety with documented hyperthyroidism — treat the thyroid first; magnesium will not resolve anxiety driven by elevated T3/T4.
Key Research Papers
- Boyle NB, Lawton C, Dye L (2017). The effects of magnesium supplementation on subjective anxiety and stress — a systematic review. Nutrients. — PubMed
- Pickering G, Mazur A, Trousselard M et al. (2020). Magnesium status and stress: the vicious circle concept revisited. Nutrients. — PubMed
- Sartori SB, Whittle N, Hetzenauer A, Singewald N (2012). Magnesium deficiency induces anxiety and HPA axis dysregulation: modulation by therapeutic drug treatment. Neuropharmacology. — PubMed
- Tarleton EK et al. (2017). Role of magnesium supplementation in the treatment of depression: a randomized clinical trial. PLoS One. — PubMed
- Eby GA, Eby KL (2006). Rapid recovery from major depression using magnesium treatment. Medical Hypotheses. — PubMed
- Wienecke E, Nolden C (2016). Long-term HRV analysis shows stress reduction by magnesium intake. MMW Fortschritte der Medizin. — PubMed
- Kirov GK, Birch NJ, Steadman P, Ramsey RG (1994). Plasma magnesium levels in a population of psychiatric patients: correlations with symptoms. Neuropsychobiology. — PubMed
- Botturi A, Ciappolino V, Delvecchio G et al. (2020). The role and the effect of magnesium in mental disorders: a systematic review. Nutrients. — PubMed
- De Souza MC, Walker AF, Robinson PA, Bolland K (2000). A synergistic effect of a daily supplement for one month of 200 mg magnesium plus 50 mg vitamin B6 for the relief of anxiety-related premenstrual symptoms. Journal of Women's Health. — PubMed
- Mocking RJ, Harmsen I, Assies J et al. Vagal tone and HPA axis function in major depression. — PubMed
- Schutten JC et al. (2025). The role of magnesium in depression, migraine, Alzheimer's disease, and cognitive health: a comprehensive review. Nutrients. — PubMed
- Slutsky I et al. (2010). Enhancement of learning and memory by elevating brain magnesium. Neuron. (NMDA mechanism) — PubMed
PubMed Topic Searches
- PubMed: Magnesium anxiety supplementation RCT
- PubMed: Magnesium GABA-A allosteric modulation
- PubMed: Glycine inhibitory NT brainstem/spinal
- PubMed: Magnesium HPA axis cortisol
- PubMed: Magnesium B6 PMS anxiety
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Magnesium Glycinate Overview
- Magnesium Glycinate Benefits Hub
- Magnesium Glycinate for Sleep
- Magnesium Glycinate for Muscle Relaxation
- Magnesium Glycinate Bioavailability
- Magnesium (Overview)
- Glycine
- Tryptophan (Serotonin Precursor)
- Vitamin B6 (P5P Cofactor)
- Anxiety
- Depression
- Insomnia
- Natural Anxiety Relief
- Stress Management
- Sleep Hygiene