Copper Toxicity (Wilson's Disease): Nausea and Stomach Upset
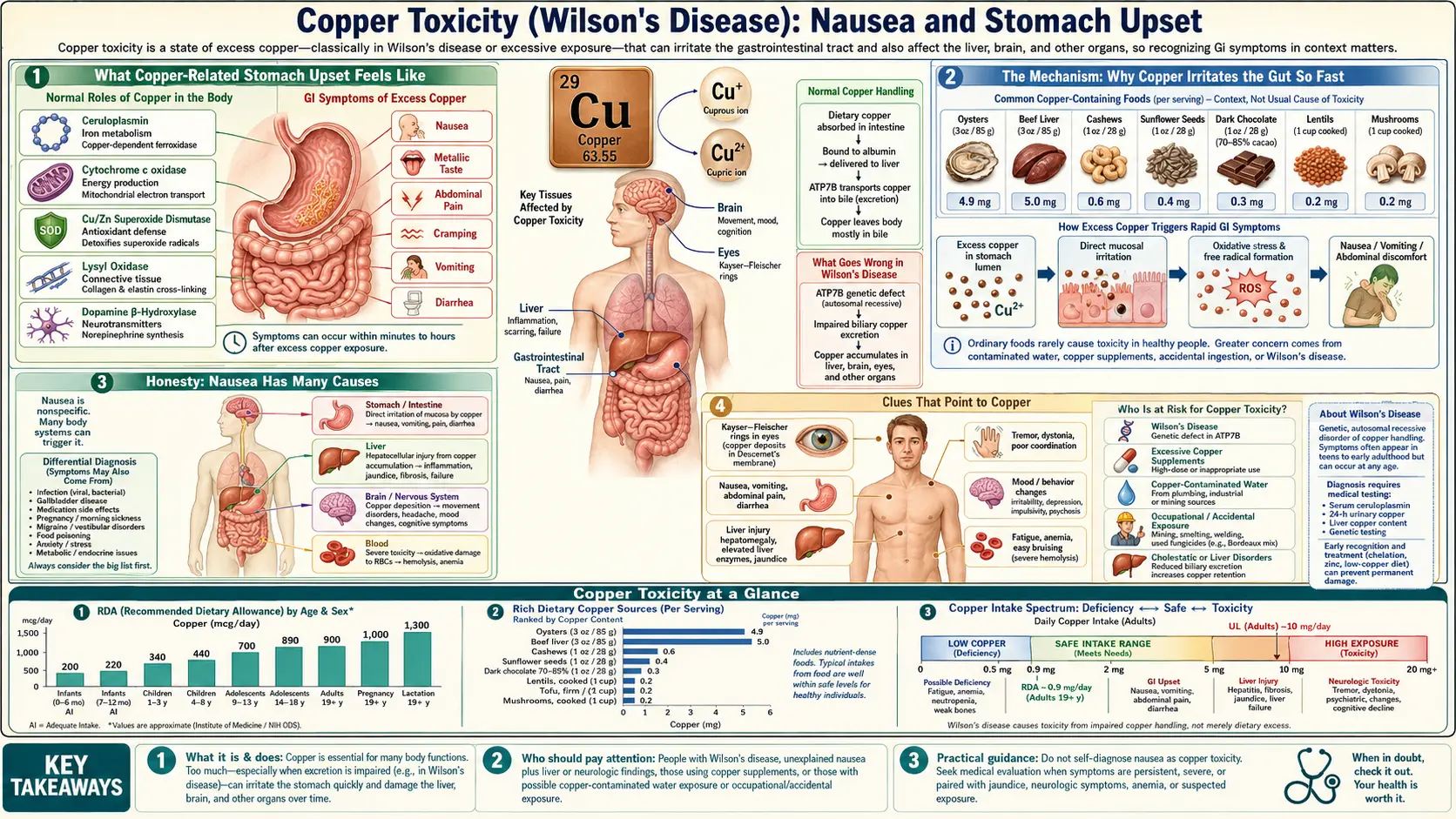
Of all the symptoms copper can cause, nausea and stomach upset are the fastest and the most reliable — but only when the dose is large and swallowed all at once. A single big gulp of copper — from contaminated water, a copper cooking pot, an acidic drink stored in copper, or a swallowed supplement — can set off cramping, queasiness, and vomiting within minutes to an hour, because copper irritates the lining of the stomach directly. That makes acute copper an honest exception to a hard truth about most copper toxicity: the slow, chronic kind — the kind seen in Wilson's disease, the inherited disorder in which the body cannot clear copper — usually does its damage silently, hitting the liver and brain long before the stomach ever complains. This page is about the acute stomach reaction: how it feels, why copper irritates the gut so quickly, why nausea is a notoriously non-specific symptom, and the clues that point to copper rather than an ordinary upset stomach.
Table of Contents
- What Copper-Related Stomach Upset Feels Like
- The Mechanism: Why Copper Irritates the Gut So Fast
- Honesty: Nausea Has Many Causes
- Clues That Point to Copper
- Common Sources of a Copper Overload
- Wilson's Disease: The Silent Kind
- Getting Checked
- How Copper Overload Is Treated
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Copper-Related Stomach Upset Feels Like
When stomach symptoms come from copper, they almost always follow a large dose taken at once — and they come on quickly. This is the defining feature: the timing is tight. Within minutes to about an hour of swallowing a copper-heavy drink or supplement, the gut reacts. The usual pattern is:
- A metallic taste. Many people notice an unpleasant, coppery or metallic taste in the mouth even before the stomach turns — an early hint that what was swallowed is the culprit.
- Queasiness and nausea. A rising sense of sickness in the stomach, often within the first half hour.
- Vomiting. Copper is a powerful emetic — it provokes vomiting readily, which is the body's attempt to expel the irritant. In heavier exposures the vomit may look blue-green from the copper itself.
- Cramping abdominal pain. A gripping, colicky ache across the upper abdomen, sometimes with a burning quality (see also abdominal pain).
- Diarrhea. Loose stools often follow, sometimes tinged blue-green, as the irritant moves through the gut.
For a mild exposure — say, water that sat overnight in new copper plumbing and picked up a modest amount — this may be the whole story: a brief bout of nausea, perhaps one episode of vomiting, then recovery within a few hours once the copper is gone. The gut, in effect, defends you by ejecting the irritant before much of it is absorbed, which is one reason mild acute exposures rarely cause lasting harm.
A large deliberate or accidental dose — swallowing copper sulfate, for example — is a very different and dangerous event. Severe, repeated vomiting (often blue-green), intense abdominal pain, and bleeding from the irritated stomach lining can follow, and the danger then extends well beyond the stomach to the blood, liver, and kidneys. That medical emergency is described under treatment and red flags below.
One contrast is worth fixing in mind from the start. This acute, dose-linked stomach upset is not how the most important form of copper toxicity usually announces itself. In Wilson's disease — where copper accumulates slowly over years — the early damage is to the liver and later the brain, and nausea, if it appears at all, is usually a downstream symptom of liver trouble rather than direct stomach irritation. The fast, gulp-it-and-feel-sick pattern on this page is the signature of acute copper.
The Mechanism: Why Copper Irritates the Gut So Fast
The speed of the reaction is the clue to the mechanism. Symptoms that arrive within minutes cannot be the result of copper being absorbed, distributed around the body, and slowly poisoning distant organs — there simply is not time. Instead, acute copper acts locally, right where it lands: on the lining of the mouth, stomach, and gut. Two things are happening at once.
Direct chemical irritation (a corrosive effect). Copper salts in solution — especially copper sulfate, but also the copper that dissolves off plumbing or cookware into acidic liquids — are caustic to the delicate mucous membrane that lines the stomach. At high concentration they injure the surface cells directly, much as a harsh chemical would, inflaming and in severe cases eroding the lining. That local injury is read by the gut as a strong “something is wrong here” signal.
Triggering the vomiting reflex. The irritated stomach lining is densely supplied with sensory nerves that report to the brainstem's vomiting center. Copper is one of the most reliable substances for setting off this reflex — historically, copper sulfate was even used (and later abandoned as unsafe) as an emetic to make people vomit. When the stomach lining is chemically assaulted, those nerves fire, nausea builds, and vomiting follows as a protective expulsion.
An analogy. Think of the stomach lining as the painted surface of a wall and copper as a splash of paint stripper. A faint mist that you wipe off quickly leaves the paint intact — mild, fleeting irritation. A bucketful thrown against the wall blisters and strips the paint — deep injury that won't simply wipe away. The dose, and the concentration, decide whether you get a passing wave of nausea or a corrosive emergency. This is also why diluting copper matters so much: the same total amount of copper spread through a large volume of water irritates far less than the same amount in a concentrated swallow.
Human studies make the dose-dependence concrete. In carefully controlled experiments, healthy volunteers given drinking water with rising copper concentrations reported nausea more and more often as the concentration climbed, with queasiness becoming common above roughly 4–6 milligrams of copper per liter — and the symptom appearing within an hour of drinking, then settling once the exposure stopped. That is the fingerprint of local irritation, not systemic poisoning: tied to concentration, fast in onset, and quick to fade when the source is removed.
Honesty: Nausea Has Many Causes
It would be misleading to suggest that an upset stomach points to copper. Nausea and vomiting are among the most non-specific symptoms in all of medicine — the body's all-purpose response to an enormous range of insults — and copper is a genuinely uncommon cause. The overwhelming majority of the time, queasiness has a far more ordinary explanation:
- Viral gastroenteritis (“stomach flu”) — by far the most common cause of sudden nausea, vomiting, and diarrhea, usually with others around you falling ill too.
- Food poisoning from contaminated food, which can mimic acute copper closely: rapid onset, vomiting, cramps. The shared meal, not a shared water source, is the usual link.
- Medications — many drugs irritate the stomach or trigger nausea, including antibiotics, NSAIDs, iron tablets, chemotherapy, and opioids.
- Pregnancy — an essential first thought for nausea in anyone who could be pregnant.
- Migraine, motion sickness, and inner-ear problems, which produce nausea through the brain and balance system rather than the gut.
- Other gut conditions — reflux, gastritis, ulcers, gallbladder disease, and many more.
So the honest framing is this: if your stomach is upset, copper is far down the list of likely explanations, and you should not assume it. Copper becomes a real possibility only when something in the story points to it — a copper source, a tight time-link to drinking or swallowing something, a metallic taste, a blue-green tinge. Those clues are the subject of the next section. Without them, an upset stomach is almost always something else, and chasing copper would be a distraction from the real cause.
Clues That Point to Copper
What separates copper from the far more common causes of nausea is the context. Any one of these on its own means little; several together should raise copper as a serious possibility worth mentioning to a clinician:
- A tight time-link to drinking or swallowing something. Symptoms that begin within minutes to an hour of a specific drink, a supplement, or a meal cooked or stored in copper — rather than building over a day — fit copper's fast, local mechanism.
- A plausible copper source. New or corroding copper plumbing (especially the first water drawn in the morning after it sat overnight), well water that is acidic or “aggressive,” unlined copper or brass cookware used for acidic foods, a copper water bottle or moonshine still, or a high-dose copper supplement.
- A metallic taste in the mouth around the same time — an unusual and suggestive accompaniment.
- A blue-green tinge to vomit, stool, or even the water itself, or blue-green staining on fixtures — a striking and fairly specific sign of copper.
- More than one person affected from a shared source. If others who drank the same water became queasy too, a contaminated supply is more likely than a coincidental virus — though a shared meal points instead to food poisoning, so the distinction matters.
Even with these clues, acute copper from everyday household exposure is usually mild and self-limited. The point of recognizing the pattern is twofold: to remove the source (flush the pipes, replace the cookware, stop the supplement) so it does not happen again, and to know when a large exposure has crossed into the dangerous territory described under red flags. For the chronic, source-independent overload of Wilson's disease, the clues are entirely different — not stomach upset, but unexplained liver disease, tremor, or a change in behavior in a young person.
Common Sources of a Copper Overload
For acute stomach symptoms specifically, the copper almost always comes from outside the body in a single large dose — not from food, which delivers copper too gradually and in too small an amount to irritate the gut. The usual sources are:
- Contaminated drinking water. The most common everyday source. Copper plumbing — especially new pipes that have not yet built up a protective coating, or older pipes carrying acidic, low-mineral (“soft”) or stagnant water — can leach enough copper to upset the stomach. Water that has sat in the pipes overnight picks up the most; the simple fix of running the tap for a minute before drinking dramatically lowers the concentration.
- Acidic foods or drinks stored or cooked in copper or brass. Unlined copper pots, copper water bottles, brass vessels, and copper cocktail mugs can dissolve copper into acidic contents — citrus juice, vinegar, carbonated or fermented drinks, tomato sauce. This is why food-safety codes restrict bare copper surfaces from contact with acidic food.
- High-dose copper supplements. Swallowing far more copper than the body needs — through an over-strong supplement or a mistaken dose — can irritate the stomach. The adult tolerable upper intake level for copper from supplements and food is about 10 milligrams per day; everyday balanced diets sit well below it, but concentrated pills can exceed it.
- Copper sulfate and other copper salts. Used in some pesticides, algicides, and industrial products, copper sulfate is the classic cause of severe acute poisoning — usually from accidental or intentional ingestion of a concentrated solution, and a true medical emergency rather than a household upset.
Notice what is not on this list: ordinary food. Liver, shellfish, nuts, seeds, and dark chocolate are rich in copper, but the amounts and the slow pace of a meal do not irritate the stomach. A normal diet, even a copper-rich one, does not cause acute copper stomach upset — another reason an isolated bout of nausea is far more likely to be a virus or something you ate than the copper in your food.
Wilson's Disease: The Silent Kind
The page title pairs copper toxicity with Wilson's disease for an important reason — and to draw a sharp contrast with everything above. Wilson's disease is a rare inherited disorder (a fault in the ATP7B gene) in which the liver cannot package copper for disposal into bile. Copper that should leave the body instead builds up, year after year, first in the liver and later spilling over to the brain and other organs.
The crucial point is that this slow, internal overload is usually not felt as stomach upset. Unlike a corrosive gulp of copper sulfate, the copper in Wilson's disease never sits in concentrated form against the stomach lining — it accumulates quietly inside cells. For years there may be no symptoms at all. When symptoms finally appear, they are the symptoms of a damaged liver or brain: fatigue, jaundice, fluid buildup, and abnormal liver tests; or tremor, slurred speech, difficulty with fine movements, and changes in mood, personality, or school performance, typically emerging between the teens and the thirties. A telltale physical sign, the golden-brown Kayser–Fleischer ring at the edge of the cornea, reflects copper deposited in the eye.
Nausea can occur in Wilson's disease, but as a secondary consequence of liver dysfunction — the queasiness and poor appetite that accompany hepatitis or cirrhosis — not as the direct gastric irritation of acute copper. So the two halves of “copper toxicity” behave almost oppositely: the acute, external kind announces itself loudly and fast through the stomach and is usually mild; the chronic, internal kind of Wilson's disease is silent and slow yet far more serious. Recognizing that difference is the single most useful idea on this page. Wilson's disease is eminently treatable when caught, which is why unexplained liver disease or new neurological changes in a young person should prompt a doctor to test for it — covered in the sections that follow.
Getting Checked
How copper is investigated depends entirely on which problem is suspected, because acute and chronic copper are diagnosed very differently.
For an acute exposure with stomach upset, the diagnosis is mostly about the story and the source. A clinician will ask what was swallowed, how much, how fast the symptoms came on, and whether there was a metallic taste or blue-green coloring. For mild household exposures, that history plus removing the source is often all that is needed. The water itself can be tested for copper (public guidance flags drinking water above about 1.3 milligrams per liter). After a large ingestion, the picture is urgent and hospital-based: blood tests look for the dangerous downstream effects — a complete blood count and blood film for the breakdown of red blood cells (hemolytic anemia), liver function tests for liver injury, and a comprehensive metabolic panel with kidney function — sometimes alongside a blood copper level to gauge the magnitude.
For suspected Wilson's disease, a single blood copper level is not the answer — it can be misleading because most blood copper is bound up in the protein ceruloplasmin. The standard work-up instead combines a low serum ceruloplasmin, a high 24-hour urinary copper excretion, an eye examination for Kayser–Fleischer rings, and, when needed, a liver biopsy measuring the copper content of liver tissue or genetic testing of the ATP7B gene. This is specialist territory, usually coordinated by a liver specialist (hepatologist). The takeaway for a patient: if you have unexplained liver disease or new neurological symptoms and are young, ask whether Wilson's disease has been ruled out — it is treatable, and it is missed when no one thinks to test for it.
How Copper Overload Is Treated
Treatment, too, splits along the same acute-versus-chronic line.
- Mild acute exposure. Usually nothing more than removing the source and supportive care is required. Stop drinking the suspect water (and flush the pipes), retire the copper cookware or bottle, or discontinue the supplement. Sip clear fluids to stay hydrated while the nausea settles — which it typically does within hours, because the gut has already done much of the work by expelling the irritant.
- Severe acute poisoning. A large ingestion of copper sulfate or a similar salt is a medical emergency managed in hospital. Care centers on aggressive supportive treatment — intravenous fluids, control of vomiting, and protection of the kidneys — and on watching for and treating the dangerous complications: hemolysis (destruction of red blood cells), acute liver injury, and acute kidney injury. In serious cases, chelation drugs that bind copper so it can be excreted are used, and the most severe cases may need treatments to remove copper or its breakdown products from the blood. This is decided by clinicians, ideally with input from a poison-control center; it is not something to manage at home.
- Wilson's disease. Treatment is lifelong and aims to pull excess copper out of the body and then keep it from re-accumulating. Chelating agents (such as penicillamine or trientine) bind copper for removal in the urine; zinc works differently, blocking copper absorption from the gut by inducing a protein in the intestinal lining that traps it. Patients also limit very copper-rich foods (liver, shellfish, nuts, chocolate). Started early and taken consistently, this treatment can halt and even reverse much of the damage — which is exactly why diagnosing it matters so much.
The interaction with zinc is a useful thread connecting the two: zinc and copper compete for absorption in the gut, which is why high-dose zinc both treats Wilson's disease and, taken to excess on its own, can cause a copper deficiency. It is a reminder that these trace metals are balanced against one another, and that more of one is not always better.
When to Seek Care / Red Flags
Most brief stomach upset — copper-related or not — settles on its own. But certain features mean seek care now, and a known or suspected large copper ingestion should be treated as an emergency and discussed immediately with a poison-control center or emergency services:
- A known or suspected large copper ingestion — for example, swallowing copper sulfate or another copper compound, whether accidental or intentional. Do not wait for symptoms to worsen; contact poison control or emergency services at once.
- Severe or persistent vomiting, especially if it is blue-green or contains blood, or vomiting that prevents keeping any fluids down.
- Severe abdominal pain or signs of bleeding from the gut — black, tarry stools, or blood in the stool.
- Signs of red-blood-cell breakdown or organ injury — yellowing of the skin or eyes (jaundice), dark or reddish-brown urine, passing little or no urine, breathlessness, or marked weakness.
- Dehydration from ongoing vomiting or diarrhea — dizziness on standing, a dry mouth, little urine, or confusion.
- Mental status changes — confusion, extreme drowsiness, or collapse.
Separately, and without any stomach upset at all, see a doctor about possible chronic copper trouble if a young person develops unexplained liver disease, persistent fatigue with abnormal liver tests, or new neurological or psychiatric symptoms such as tremor, slurred speech, clumsiness, or a change in personality — these are the warning signs of Wilson's disease, not of an irritated stomach, and they warrant testing rather than reassurance. When a large copper exposure is even possible, it is always safer to call for advice than to wait and see.
Key Research Papers
- Pizarro F, Olivares M, Gidi V, Araya M (1999). The Gastrointestinal Tract and Acute Effects of Copper in Drinking Water and Beverages. Reviews on Environmental Health;14(4):231-238. — DOI: 10.1515/reveh.1999.14.4.231
- Pizarro F, Olivares M, Araya M, Gidi V, Uauy R (2001). Gastrointestinal effects associated with soluble and insoluble copper in drinking water. Environmental Health Perspectives;109(9):949-952. — DOI: 10.1289/ehp.01109949
- Araya M, Olivares M, Pizarro F, Llanos A, Figueroa G, Uauy R (2004). Community-Based Randomized Double-Blind Study of Gastrointestinal Effects and Copper Exposure in Drinking Water. Environmental Health Perspectives;112(10):1068-1073. — DOI: 10.1289/ehp.6913
- Gaetke LM, Chow CK (2003). Copper toxicity, oxidative stress, and antioxidant nutrients. Toxicology;189(1-2):147-163. — DOI: 10.1016/s0300-483x(03)00159-8
- Sinkovič A, Strdin A, Svenšek F (2008). Severe Acute Copper Sulphate Poisoning: A Case Report. Archives of Industrial Hygiene and Toxicology;59(1):31-35. — DOI: 10.2478/10004-1254-59-2008-1847
- Oldenquist G, Salem M (1999). Parenteral copper sulfate poisoning causing acute renal failure. Nephrology Dialysis Transplantation;14(2):441-443. — DOI: 10.1093/ndt/14.2.441
- Milne DB (1998). Copper intake and assessment of copper status. The American Journal of Clinical Nutrition;67(5):1041S-1045S. — DOI: 10.1093/ajcn/67.5.1041S
- La Fontaine S, Mercer JFB (2007). Trafficking of the copper-ATPases, ATP7A and ATP7B: Role in copper homeostasis. Archives of Biochemistry and Biophysics;463(2):149-167. — DOI: 10.1016/j.abb.2007.04.021
- Ala A, Walker AP, Ashkan K, Dooley JS, Schilsky ML (2007). Wilson's disease. The Lancet;369(9559):397-408. — DOI: 10.1016/S0140-6736(07)60196-2
- European Association for the Study of the Liver (2012). EASL Clinical Practice Guidelines: Wilson's disease. Journal of Hepatology;56(3):671-685. — DOI: 10.1016/j.jhep.2011.11.007
- Alkhouri N, Gonzalez-Peralta RP, Medici V (2023). Wilson disease: a summary of the updated AASLD Practice Guidance. Hepatology Communications;7(6):e0150. — DOI: 10.1097/hc9.0000000000000150
PubMed Topic Searches
- PubMed — Copper in drinking water and gastrointestinal symptoms
- PubMed — Acute copper sulphate poisoning
- PubMed — Copper toxicity, emesis, and gastric irritation
- PubMed — Wilson's disease: diagnosis and treatment
- PubMed — Copper tolerable upper intake and toxicity
Connections
- Copper Toxicity Symptom Hub
- Copper Toxicity and Liver Damage
- Copper Toxicity: Neurological & Psychiatric
- Copper Deficiency Symptom Hub
- Copper Overview
- Copper Benefits
- Food Sources of Copper
- Zinc
- Iron
- Liver Disease
- Cirrhosis
- Acute Kidney Injury
- Anemia
- Nausea and Vomiting
- Abdominal Pain
- Comprehensive Metabolic Panel
- Liver Function Tests
- Complete Blood Count
- Wilson's Disease — the inherited copper-overload disorder whose damage is silent rather than gastric.