Cobalt Toxicity: Symptoms, Causes, and Risks
Cobalt toxicity means the body is carrying too much cobalt — almost always from an unusual source, not from a normal diet. Here is the key thing to understand: your body needs only a tiny trace of cobalt, and that trace arrives already built into vitamin B12, where a single cobalt atom sits at the center of the molecule. You do not need free cobalt at all, and there is no everyday food that delivers a harmful amount. When cobalt poisoning happens, it comes from somewhere out of the ordinary: a worn metal-on-metal hip implant slowly shedding cobalt into the bloodstream, years of inhaling cobalt dust in a "hard-metal" workshop, large doses of cobalt supplements, or — in a notorious 1960s episode — cobalt added to beer. Excess cobalt is dangerous mainly because of what it does to the heart, where it can poison the muscle and cause a form of heart failure called cardiomyopathy; it can also damage the thyroid, the nerves, hearing and vision, and (when inhaled) the lungs. And like many metal toxicities, it is often quiet at first — the cobalt level climbs while the person feels only vaguely unwell. This hub explains what cobalt toxicity is, why it harms the heart, why it can stay silent, what causes it, and how it is diagnosed and treated — with deep-dive pages on cobalt cardiomyopathy and on implant- and inhalation-related exposure. True cobalt toxicity is uncommon and is real medical territory; do not try to diagnose or treat it on your own.
Symptom Deep-Dive Pages
Heart (Cardiomyopathy)
The most dangerous consequence of cobalt overload — how excess cobalt poisons heart-muscle cells and causes a dilated cardiomyopathy, the lessons of the 1960s "beer-drinkers' cardiomyopathy" outbreaks, and why this can be partly reversible if the cobalt is removed in time.
Metal Implants & Inhalation
The two leading modern sources of cobalt exposure — a failing metal-on-metal hip implant that sheds cobalt ions into the blood (arthroprosthetic cobaltism), and the occupational dust that causes hard-metal lung disease — how each is recognized, monitored, and managed.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Cobalt Toxicity?
- Why Excess Cobalt Is Dangerous
- Why It Often Has Few Early Symptoms
- Common Causes of Cobalt Overload
- How Cobalt Toxicity Is Diagnosed
- How Cobalt Overload Is Treated
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
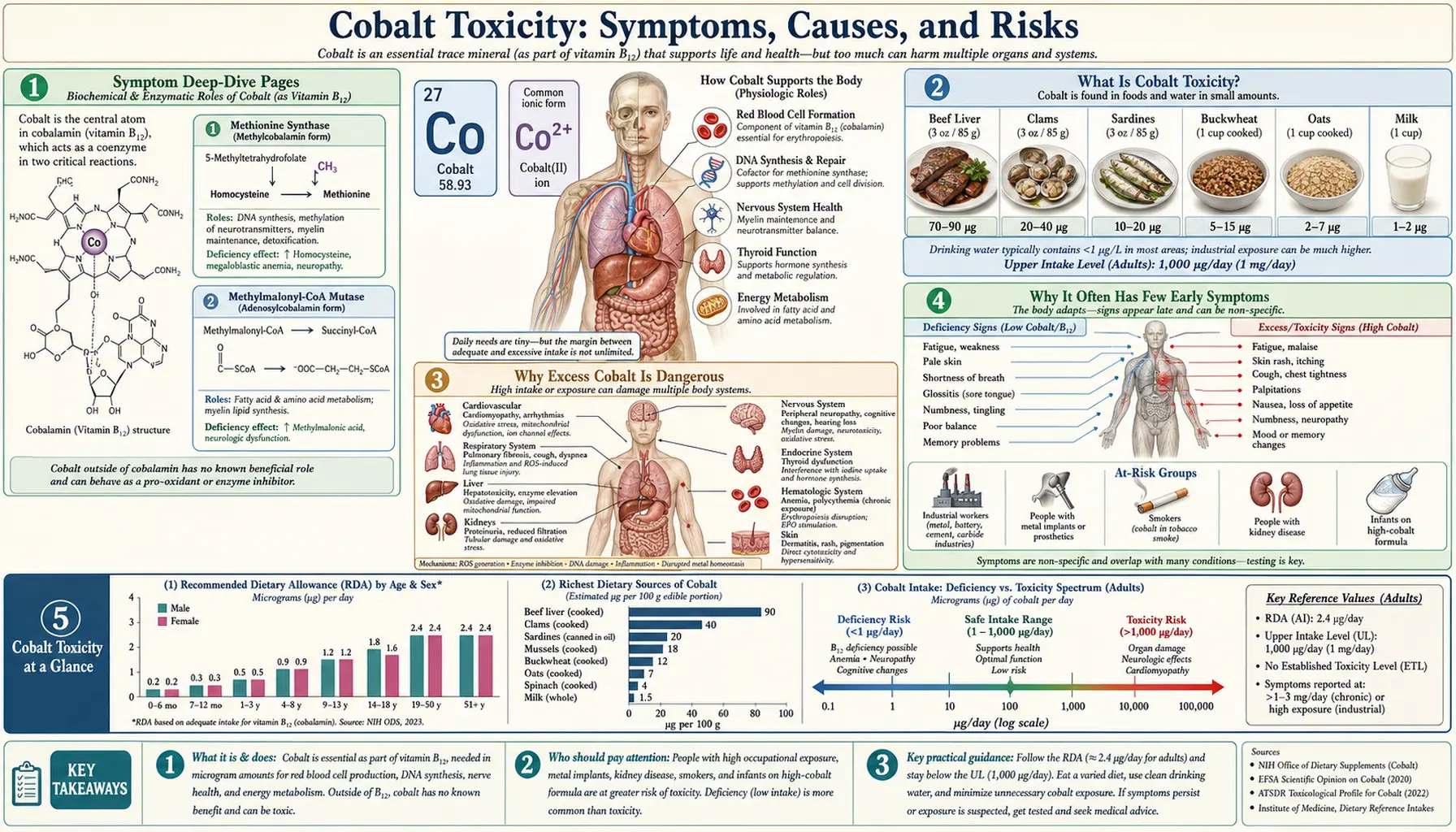
What Is Cobalt Toxicity?
Cobalt is a trace element — the body needs only a vanishingly small amount of it, and it needs that amount in just one form: as the metal atom locked inside vitamin B12 (cobalamin). The word cobalamin literally tells you cobalt is part of the vitamin. In that role cobalt is essential, helping make red blood cells and keep nerves healthy. But free, "loose" cobalt — cobalt that is not packaged inside B12 — serves no known purpose in humans, and in large enough quantities it becomes a poison. Cobalt toxicity (sometimes called cobaltism) is what happens when the body accumulates too much of this free cobalt.
The most important fact to hold onto is that cobalt toxicity is uncommon, and ordinary food does not cause it. The cobalt in a normal diet is tiny, and most of it is the harmless B12 form. To become poisoned, a person almost always has to be exposed to an unusual source — a medical device, an occupational dust, a high-dose supplement, or a contaminated product. This makes cobalt very different from an electrolyte like potassium, where the danger comes from the body's own balance; with cobalt, the danger comes from the outside.
Doctors generally encounter cobalt overload in one of a few recognizable settings, and the amount that matters depends heavily on the route and the time-course:
- Slow build-up from a metal implant. A worn or failing metal-on-metal hip replacement can release cobalt ions into the bloodstream gradually over months or years. Blood cobalt levels that are normally well under 1 microgram per litre can climb into the tens or even hundreds in severe cases. This slow, internal source is the most common modern cause of systemic cobalt toxicity.
- Inhaled cobalt dust at work. Workers who grind, polish, or sharpen "hard metal" (tungsten carbide cemented with cobalt) — or who work in cobalt refining or diamond-polishing — can breathe in cobalt particles for years. Here the danger is concentrated in the lungs, though high exposure can affect the rest of the body too.
- Ingested cobalt — supplements and contaminated products. Cobalt salts taken in large oral doses can poison the body. Historically this happened with cobalt-containing tonics, with cobalt deliberately added to beer as a foam stabilizer (causing the 1960s cardiomyopathy outbreaks), and occasionally with high-dose supplements marketed for unproven purposes.
Because cobalt overload arises from such specific situations, the single most useful question in evaluating it is not "how do you feel?" but "where could the cobalt be coming from?" Identifying and stopping that source is the foundation of every treatment decision that follows.
Why Excess Cobalt Is Dangerous
If cobalt toxicity is so uncommon, why is it taken seriously when it does occur? The leading answer is the same organ that makes hyperkalemia dangerous: the heart. The most feared consequence of cobalt overload is a cardiomyopathy — a poisoning of the heart muscle that weakens it and can lead to heart failure. This, more than any other effect, is what gives cobalt toxicity its reputation, and it is covered in depth on the Heart (Cardiomyopathy) page.
Here is the mechanism in plain language. Heart-muscle cells are among the most energy-hungry cells in the body; they never rest, and they depend on tiny power plants inside each cell — the mitochondria — to burn fuel and keep beating. Free cobalt jams that machinery. It binds to and interferes with key enzymes the mitochondria use to extract energy from food, so the heart cell is, in effect, starved of power even while fuel is present. Think of it as a factory whose machines are fine but whose electricity keeps cutting out. Over time the weakened, energy-starved heart muscle stretches and dilates, pumps poorly, and the result is the picture of dilated cardiomyopathy and heart failure (see Cardiomyopathy and Heart Failure). Cobalt is also thought to disturb how the heart handles calcium and to add oxidative stress, both of which compound the damage.
The cardiac danger is the headline, but cobalt is a broad toxin and excess can harm several other systems — a pattern sometimes called cobaltism when it appears together:
- Thyroid. Cobalt can block the thyroid gland's ability to use iodine, reducing thyroid hormone production. In the era when cobalt was used to treat anemia, an enlarged thyroid (goiter) and an underactive thyroid were recognized side effects. See Hypothyroidism and Thyroid Disorders.
- Nerves, hearing, and vision. High systemic cobalt — classically from a failing hip implant — has caused peripheral nerve damage, hearing loss, ringing in the ears, and visual disturbances, a constellation reported under the name arthroprosthetic cobaltism. See Peripheral Neuropathy.
- Blood — too many red cells. Counter-intuitively, cobalt can raise red blood cell production. It mimics low oxygen at the cellular level, stabilizing a signal (hypoxia-inducible factor) that drives the kidney to make more erythropoietin, the hormone that tells the marrow to build red cells. This is why cobalt was once used to treat anemia — and why excess can cause an overly high red-cell count (a secondary polycythemia-like picture).
- Lungs (inhaled exposure). Breathing cobalt dust causes its own distinct diseases — occupational asthma and a scarring lung condition called hard-metal lung disease — covered on the Metal Implants & Inhalation page and below.
One honesty note worth keeping in view: not everyone with a raised cobalt level develops any of these problems, and the relationship between a given blood level and actual organ harm is not a simple, fixed line. Individual susceptibility, the form of cobalt, how fast it accumulated, and other exposures all matter. That uncertainty — how much cobalt is "too much" for a given person — is one of the genuinely unsettled questions in this field, which is exactly why monitoring and clinical judgment, not a single number, guide care.
Why It Often Has Few Early Symptoms
Cobalt toxicity, especially the slow kind that builds up from a metal implant, tends to be quiet at the start. The cobalt level can rise steadily for months while the person feels only a little off — more tired than usual, a bit short of breath on the stairs, perhaps some ringing in the ears or trouble with vision that is easy to attribute to age or stress. None of these early complaints points clearly at cobalt. By the time more obvious problems appear — a failing heart, marked hearing or vision loss, an obviously enlarged thyroid — the exposure may have been going on for a long time.
Why so quiet? Two reasons. First, the early symptoms are non-specific: fatigue, mild breathlessness, low mood, and subtle nerve or sensory changes have countless everyday explanations, so neither the patient nor the doctor naturally thinks of a rare metal poisoning. Second, the body has no built-in alarm for cobalt the way it does for, say, a broken bone; the harm accumulates silently inside cells and the heart muscle long before it announces itself. The danger, as with so many slow toxicities, is that the calm is mistaken for safety.
This is why knowing your exposure matters more than waiting for symptoms. The people who should think about cobalt — and, where appropriate, be monitored for it — are defined by their situation, not by how they feel:
- Anyone with a metal-on-metal hip implant, particular older or large-head designs, which orthopaedic and regulatory bodies now recommend following with periodic checks (often including blood cobalt and chromium levels and imaging) precisely because trouble can be silent.
- Workers with years of cobalt dust exposure — in hard-metal (tungsten carbide) tooling, cobalt refining, diamond polishing, or some battery and alloy manufacturing — who are candidates for occupational health surveillance.
- People taking high-dose cobalt supplements or unregulated products marketed (without good evidence) for stamina, anemia, or other claims.
- Anyone in these groups who develops new, unexplained heart, thyroid, hearing, vision, or nerve symptoms — the combination of a plausible source and otherwise unexplained multi-system symptoms is the pattern that should prompt testing.
The take-home is the mirror image of reassurance: feeling more or less fine does not prove your cobalt level is fine if you have a real source of exposure. In those situations, the level is something to measure, not to guess.
Common Causes of Cobalt Overload
Because food does not cause it, cobalt toxicity nearly always traces to one of a short list of out-of-the-ordinary sources. Knowing them is most of the diagnosis.
- Metal-on-metal hip implants — the leading modern cause. Some hip replacements used a cobalt-chromium alloy ball moving against a cobalt-chromium socket. As these surfaces wear — especially in certain large-diameter designs that were later recalled or restricted — they shed microscopic metal particles and release cobalt ions that enter the bloodstream. The result, arthroprosthetic cobaltism, can produce both local damage around the joint and the systemic effects on heart, nerves, hearing, vision, and thyroid described above. The risk is highest with a failing or malpositioned implant, and it is why these patients are now monitored. See the Metal Implants & Inhalation deep-dive.
- Inhaled cobalt dust at work. "Hard metal" is tungsten carbide cemented together with cobalt to make extremely tough cutting tools and drill bits. Workers who grind, sharpen, or polish these tools breathe in cobalt-containing dust; so do some cobalt refinery, diamond-polishing (using cobalt-bonded discs), and alloy or battery workers. Years of such exposure cause the lung diseases discussed below, and can contribute to body-wide cobalt as well.
- Cobalt added to beer — a cautionary tale from history. In the mid-1960s, several breweries in Canada, the United States, and Europe added small amounts of cobalt salt to beer to stabilize the foam. Heavy beer drinkers consuming large daily volumes developed a severe, often fatal heart failure that became known as "beer-drinkers' cardiomyopathy" — an episode that, more than anything else, taught medicine how toxic cobalt can be to the heart. The practice was banned once the link was recognized. (See the cardiomyopathy deep-dive.)
- High-dose oral cobalt — medicinal and supplemental. Decades ago, cobalt salts were prescribed to stimulate red-cell production in certain anemias, and this use revealed cobalt's thyroid and heart toxicity. Today, deliberate medical use is essentially abandoned, but cobalt occasionally appears in unregulated supplements or tonics; large or prolonged doses can cause poisoning. (Note: this is free cobalt salt, not the harmless trace of cobalt bound inside a normal B12 supplement — ordinary vitamin B12 does not cause cobalt toxicity.)
- Athletic misuse. Because cobalt boosts erythropoietin and red cells, cobalt salts have been misused as a cheap blood-doping agent to improve endurance. This is both prohibited in sport and dangerous, exposing the user to the same multi-system toxicity.
- Other and historical sources. Heavy environmental or industrial contamination, and certain past medical practices, round out the list. In every case the theme is the same: a concentrated, non-dietary source.
A practical point: these causes do not usually combine the way electrolyte disturbances do. With cobalt, there is typically one dominant source — an implant, a job, a product — and finding it is the key to both stopping the exposure and explaining the illness.
How Cobalt Toxicity Is Diagnosed
Diagnosing cobalt toxicity is really two tasks: recognizing that cobalt might be the culprit, and then measuring it. Because the early symptoms are so non-specific, the diagnosis often hinges on a doctor connecting an unexplained pattern of symptoms with a plausible source — a metal hip implant, a dusty occupation, a supplement. Once that suspicion exists, testing can confirm it.
- Blood (and sometimes urine) cobalt levels. The central test is measuring cobalt in the blood. Levels in unexposed people are very low (typically well under about 1 microgram per litre); in implant-related toxicity they may rise into the tens or hundreds. For people with metal-on-metal hips, blood cobalt — usually together with chromium, the other component of the alloy — is the standard way to gauge how much metal the implant is releasing, with rising or markedly elevated levels prompting further evaluation. Urine cobalt can reflect recent exposure, particularly in occupational settings.
- Routine bloodwork to assess the consequences. A comprehensive metabolic panel and a complete blood count help look for the downstream effects — for example an unexpectedly high red-cell count (cobalt-driven), or clues to other organ involvement. Thyroid function tests are checked when thyroid effects are suspected.
- Heart evaluation. Because the heart is the chief concern, suspected systemic cobalt toxicity usually prompts cardiac assessment — an echocardiogram to measure how well the heart is pumping, and tests for heart failure — especially if there is breathlessness, swelling, or fatigue. (See Cardiomyopathy.)
- Imaging of the implant. When a hip replacement is the suspected source, specialized imaging (such as MARS-MRI or ultrasound) looks for tissue reactions and fluid collections (pseudotumors) around the joint that signal the implant is failing and shedding metal.
- Targeted testing for other organs. Depending on symptoms, hearing tests, vision and nerve assessments, and thyroid imaging may be added to map out the extent of the toxicity.
One honest caveat carries through diagnosis just as it did through risk: there is no single cobalt number that cleanly separates "safe" from "toxic" for every person. A level that causes serious harm in one individual may cause little in another, and a high level does not always mean organ damage is present. So the level is interpreted alongside the symptoms, the heart and organ findings, and the exposure history — not on its own.
How Cobalt Overload Is Treated
The treatment of cobalt toxicity rests on one principle above all others: find the source and stop it. Unlike an electrolyte problem, cobalt poisoning will not improve while the cobalt keeps coming in, and it often improves substantially once the supply is cut off. This is specialist medical care — there is no safe do-it-yourself remedy for cobalt overload.
- Remove the source — the cornerstone. What this means depends on the cause:
- For a failing metal-on-metal hip implant, the definitive step is usually surgical revision — replacing the worn cobalt-chromium components with a different bearing (such as ceramic or polyethylene). After revision, blood cobalt levels typically fall over the following weeks to months, and many of the systemic symptoms can improve, sometimes dramatically — though damage that is already advanced (for example to nerves or hearing) may only partly recover.
- For occupational dust, it means removing the worker from further exposure and improving workplace controls (ventilation, respiratory protection).
- For ingested cobalt, it means stopping the supplement, tonic, or other source.
- Treat the organ damage. Whatever harm cobalt has done is managed on its own terms while the body clears the metal: heart failure from cobalt cardiomyopathy is treated with standard heart-failure care (see Heart Failure); an underactive thyroid may need temporary thyroid hormone; nerve, hearing, and vision problems are assessed and supported. Encouragingly, when caught before the damage is fixed, cobalt cardiomyopathy can be partly or substantially reversible once the cobalt is removed — a hopeful contrast to many causes of heart failure.
- Chelation — a limited and uncertain role. Chelating agents are medicines that bind a metal so the body can excrete it. For some heavy-metal poisonings they are central; for cobalt the evidence is much weaker and the role is uncertain and debated. Chelation is sometimes considered in severe poisoning, but it is not a routine or proven cure, and removing the source remains far more important. Any use is a specialist decision, weighing limited benefit against real risks.
- Monitoring and follow-up. After the source is addressed, cobalt levels and the affected organs are followed over time to confirm the level is falling and the body is recovering.
The reassuring theme is that cobalt toxicity, identified and its source removed, often improves — but the whole point of recognizing and monitoring it early is to act before the heart or nerves are permanently harmed.
When to Seek Care / Red Flags
Because cobalt toxicity can build quietly, the most important "red flag" is often a situation rather than a symptom: if you have a metal-on-metal hip implant or a job with cobalt dust exposure, keep your scheduled check-ups and monitoring even when you feel well, and raise any new unexplained symptoms with your doctor. That said, certain developments — especially in someone with a known cobalt source — deserve prompt medical attention rather than watchful waiting. See a doctor promptly, and seek urgent care for cardiac symptoms, if you have any of the following:
- New or worsening breathlessness, swelling of the legs, or fatigue — possible signs of cobalt's effect on the heart (heart failure). Severe or sudden breathlessness is an emergency.
- Palpitations or an irregular heartbeat — get urgent care, as with any new significant rhythm problem.
- New hearing loss, ringing in the ears, or visual disturbance — classic systemic features of cobalt overload from a failing implant.
- Numbness, tingling, weakness, or unsteadiness — suggesting nerve involvement.
- Symptoms of an underactive thyroid — unusual tiredness, cold intolerance, weight gain, or a swelling in the front of the neck (goiter).
- Worsening pain, swelling, or a lump around a metal hip implant — which can signal a local reaction to released metal and warrants evaluation.
People at higher risk — those with a metal-on-metal hip, long-term cobalt dust exposure, or who have been taking cobalt-containing products — should have a low threshold for getting checked, because cobalt can accumulate without clear warning. If you are unsure whether a supplement or product contains cobalt, ask a pharmacist or doctor. For related conditions, see Cardiomyopathy, Heart Failure, and Hypothyroidism.
Key Research Papers
- Leyssens L, Vinck B, Van Der Straeten C, Wuyts F, Maes L (2017). Cobalt toxicity in humans — A review of the potential sources and systemic health effects. Toxicology;387:43-56. — DOI: 10.1016/j.tox.2017.05.015
- Morin Y, Daniel P (1967). Quebec Beer-Drinkers' Cardiomyopathy: Etiological Considerations. JAMA;202(13):1145-1148. — DOI: 10.1001/jama.1967.03130260067015
- Editorial (1968). Epidemic Cardiac Failure in Beer Drinkers. Nutrition Reviews;26(6):173-175. — DOI: 10.1111/j.1753-4887.1968.tb00905.x
- Bradberry SM, Wilkinson JM, Ferner RE (2014). Systemic toxicity related to metal hip prostheses. Clinical Toxicology;52(8):837-847. — DOI: 10.3109/15563650.2014.944977
- Brent J, Devlin JJ (2013). Dilemmas about the toxicological consequences of metal-on-metal hip prostheses — What we do and do not know, and what we should do. Clinical Toxicology;51(4):195-198. — DOI: 10.3109/15563650.2013.784326
- Ho VT, Caron G, Yamashita TE, et al. (2017). Metal-on-Metal Hip Joint Prostheses: a Retrospective Case Series Investigating the Association of Systemic Toxicity with Serum Cobalt and Chromium Concentrations. Journal of Medical Toxicology;13(4):321-328. — DOI: 10.1007/s13181-017-0629-1
- Tower SS (2012). Arthroprosthetic cobaltism associated with metal on metal hip implants. BMJ;344:e430. — DOI: 10.1136/bmj.e430
- Tower SS (2010). Arthroprosthetic Cobaltism: Neurological and Cardiac Manifestations in Two Patients with Metal-on-Metal Arthroplasty. Journal of Bone and Joint Surgery;92(17):2847-2851. — DOI: 10.2106/jbjs.j.00125
- Unice KM, Monnot AD, Gaffney SH, et al. (2014). Refined biokinetic model for humans exposed to cobalt dietary supplements and other sources of systemic cobalt exposure. Chemico-Biological Interactions;216:53-74. — DOI: 10.1016/j.cbi.2014.04.001
- Nemery B, Verbeken EK, Demedts M (2001). Giant Cell Interstitial Pneumonia (Hard Metal Lung Disease, Cobalt Lung). Seminars in Respiratory and Critical Care Medicine;22(4):435-448. — DOI: 10.1055/s-2001-17386
- Lison D, Lauwerys R (1996). Experimental research into the pathogenesis of cobalt/hard metal lung disease. European Respiratory Journal;9(5):1024-1028. — DOI: 10.1183/09031936.96.09051024
- Lison D, Buchet JP, Swennen B, Molders J, Lauwerys R (1994). Biological monitoring of workers exposed to cobalt metal, salt, oxides, and hard metal dust. Occupational and Environmental Medicine;51(7):447-450. — DOI: 10.1136/oem.51.7.447
PubMed Topic Searches
- PubMed — Cobalt toxicity in humans: systemic health effects
- PubMed — Cobalt cardiomyopathy and heart failure
- PubMed — Arthroprosthetic cobaltism and metal-on-metal hip implants
- PubMed — Hard metal lung disease and occupational cobalt exposure
- PubMed — Cobalt, thyroid function, goiter, and hypothyroidism
Connections
- Cobalt Toxicity: Heart (Cardiomyopathy)
- Cobalt Toxicity: Metal Implants & Inhalation
- Cobalt Overview
- Cobalt Deficiency Hub
- Vitamin B12 (Cobalamin)
- Cardiomyopathy
- Heart Failure
- Hypothyroidism
- Thyroid Disorders
- Polycythemia Vera
- Peripheral Neuropathy
- Interstitial Lung Disease
- Comprehensive Metabolic Panel
- Complete Blood Count
- Toxic Minerals
- Iron