Cobalt: Essential Core of Vitamin B12 — and Its Toxic Side
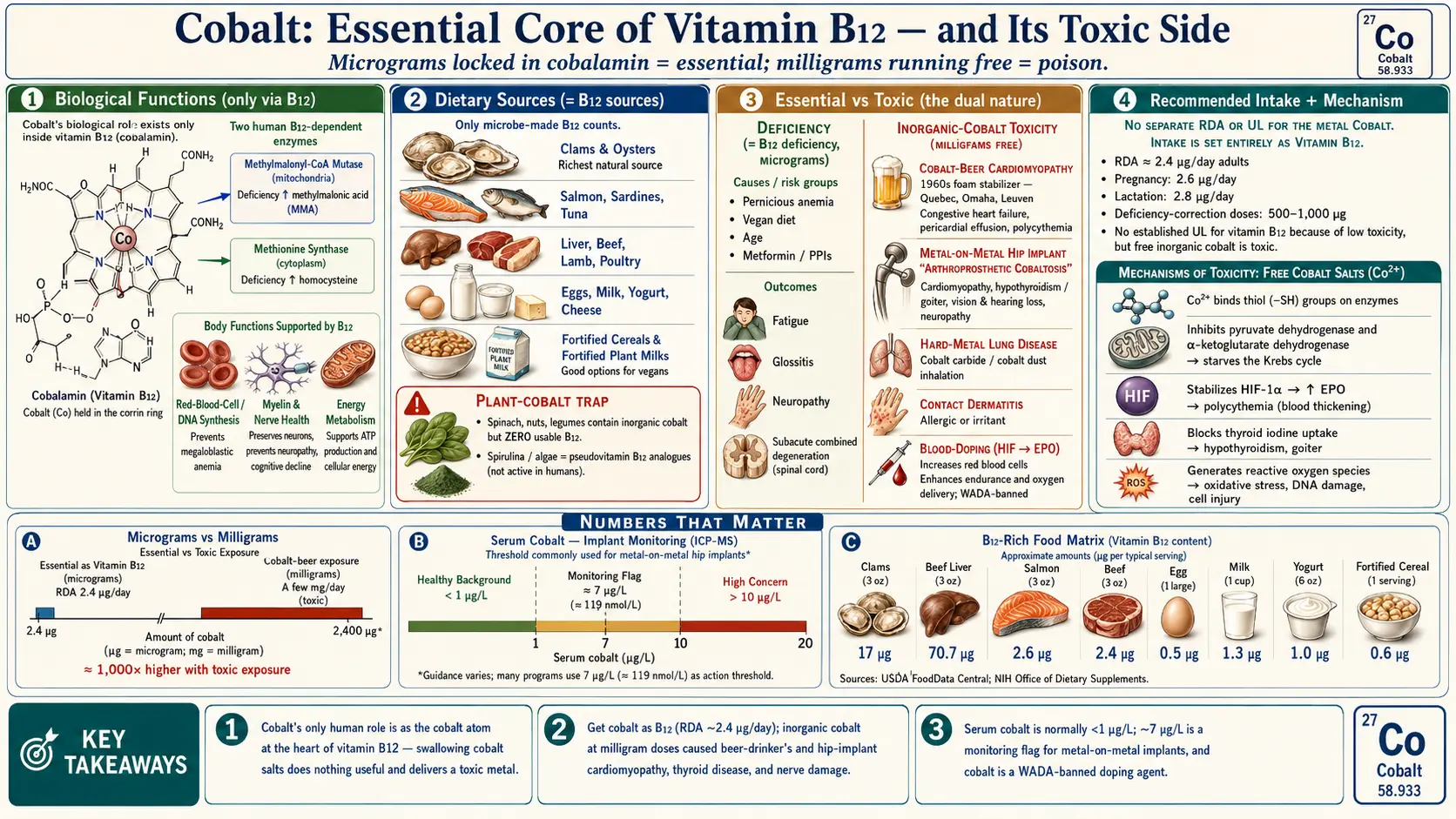
Table of Contents
- Overview
- Biological Functions
- Dietary Sources
- Deficiency
- Recommended Intake
- Supplementation & Forms
- Toxicity & Upper Limit
- Special Considerations
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Cobalt is a hard, silvery-grey metal — element number 27 on the periodic table, sitting right between iron and nickel. It has a curious double life in human health. On one hand, cobalt is genuinely essential: it forms the chemical heart of vitamin B12 (cobalamin), a vitamin without which we cannot make red blood cells or maintain a healthy nervous system. On the other hand, cobalt in its loose, inorganic form is a recognized toxin that has caused outbreaks of heart failure, thyroid disease, and nerve damage. Understanding cobalt means holding both of these truths at once.
The single most important fact about cobalt nutrition is this: the only established role for cobalt in the human body is as the central metal atom of vitamin B12. There is no recognized dietary requirement for free or inorganic cobalt. Crucially, humans cannot build a B12 molecule from raw cobalt — only certain bacteria and archaea (single-celled microorganisms) possess the enzymatic machinery to wrap cobalt inside the elaborate corrin ring that makes cobalamin. For us, "cobalt nutrition" is really just another way of saying vitamin B12 nutrition. Swallowing cobalt metal or a cobalt salt does nothing useful for B12 status; it simply delivers a potentially toxic metal.
This page therefore covers cobalt from both directions. The essential side is short and points you toward our detailed Vitamin B12 page, because that is where the real human requirement lives. The toxic side is longer and more cautionary, because cobalt's dark history — from cobalt-beer cardiomyopathy in the 1960s to systemic poisoning from worn metal-on-metal hip implants today — is exactly the kind of practical, real-world danger an ordinary reader benefits from knowing about. Cobalt is a textbook example of a metal that is indispensable in microgram amounts locked inside a vitamin, and harmful in milligram amounts running free.
Cobalt versus cobalamin: keeping the terms straight
It helps to separate three things. Elemental (inorganic) cobalt is the free metal and its simple salts — cobalt chloride, cobalt sulfate, cobalt gluconate. Cobalamin (vitamin B12) is the large organic molecule in which a single cobalt atom is held in place by a corrin ring and a series of attached groups. "Cobalt" in nutrition labels and soil-science reports usually means inorganic cobalt, which is not the same as usable B12. When a soil is called "cobalt-deficient," it matters to cattle and sheep — whose gut bacteria need that cobalt to make B12 for the animal — but it tells you nothing about whether a person eating those animals is getting enough B12.
2. Biological Functions
Every biological function of cobalt in humans runs through vitamin B12. There is no known cobalt-dependent enzyme or pathway in people that operates on free cobalt the way, say, iron operates in hemoglobin or zinc operates in hundreds of metalloenzymes. Inside the cobalamin molecule, the cobalt atom is the reactive center — it is where the chemistry actually happens, swinging between oxidation states and forming and breaking a carbon-cobalt bond that few other systems in biology can manage. Strip the cobalt out and the vitamin is inert.
The two human B12-dependent enzymes
Humans use vitamin B12 — and therefore cobalt — in exactly two enzymatic reactions, but both are vital:
- Methylmalonyl-CoA mutase uses adenosylcobalamin (a form of B12) inside mitochondria. It converts methylmalonyl-CoA into succinyl-CoA, a step that lets the body extract energy from certain fatty acids and amino acids by feeding them into the Krebs (citric-acid) cycle. When this enzyme stalls for lack of B12, methylmalonic acid backs up in the blood and urine — which is why doctors measure methylmalonic acid (MMA) as a sensitive marker of B12 deficiency.
- Methionine synthase uses methylcobalamin in the cytoplasm. It transfers a methyl (CH3) group from folate (as 5-methyltetrahydrofolate) onto homocysteine, regenerating the amino acid methionine and freeing up folate for DNA synthesis. This reaction sits at the crossroads of B12 and folate metabolism, which is why a B12 deficiency raises blood homocysteine and can mimic — and mask — a folate deficiency.
What those reactions accomplish for the body
Through these two enzymes, cobalt (as B12) supports three big, easily understood outcomes:
- DNA synthesis and red blood cell formation. By keeping folate cycling, methionine synthase allows rapidly dividing cells — especially the precursors of red blood cells in bone marrow — to copy their DNA properly. Without it, red cells are produced large, fragile, and immature, the hallmark of megaloblastic anemia.
- Nervous-system and myelin health. Adequate B12 is required to build and maintain myelin, the insulating sheath around nerves. Prolonged deficiency damages the spinal cord and peripheral nerves, producing numbness, tingling, unsteady walking, and in severe cases the classic syndrome called subacute combined degeneration.
- Energy metabolism. By feeding odd-chain fatty acids and branched-chain amino acids into the Krebs cycle, methylmalonyl-CoA mutase contributes to the body's energy supply.
In short, the entire human "need" for cobalt is the need to have a few micrograms of it pre-packaged inside cobalamin. For the full mechanistic and clinical picture, see our dedicated Vitamin B12 page.
3. Dietary Sources
Because usable cobalt reaches us only inside vitamin B12, the meaningful dietary sources of "cobalt" are simply the dietary sources of B12 — and B12 is made by microorganisms, not plants or animals. Animals accumulate B12 in their tissues because their gut bacteria (or the bacteria in the soil and feed they consume) synthesize it. That is why bioavailable cobalt-as-B12 comes overwhelmingly from animal-derived foods and from fortified foods, and essentially not at all from unfortified plants.
Foods that supply cobalt as usable vitamin B12
- Shellfish and fish: clams and oysters are among the richest natural sources of B12 on the planet; fish such as salmon, sardines, tuna, and trout are also strong sources.
- Organ and muscle meats: liver is extraordinarily B12-dense; beef, lamb, pork, and poultry all contribute.
- Eggs and dairy: milk, yogurt, cheese, and eggs provide moderate, reliable amounts.
- Fortified foods: many breakfast cereals, plant milks, and nutritional yeasts have synthetic B12 (usually cyanocobalamin) added. These are the main practical source for people who eat little or no animal food.
The plant-cobalt trap
Here is a point that trips up many people. Some leafy greens, nuts, and legumes do contain measurable inorganic cobalt, drawn up from the soil. But this cobalt is not convertible to vitamin B12 by the human body — we lack the bacterial enzymes to do it. So a spinach leaf or a handful of almonds may show "cobalt" on a mineral analysis while delivering zero usable B12. This is the single biggest reason that strict vegans and vegetarians who avoid fortified foods are at real risk of B12 deficiency despite eating plenty of cobalt-containing plants. The cobalt is there; the vitamin is not.
A related caution applies to certain fermented foods, mushrooms, algae, and spirulina that are sometimes marketed as plant B12 sources. Many contain B12 analogues (pseudovitamin B12) that look like B12 on some tests but do not work as the vitamin in humans and may even interfere with true B12. For dependable B12 without animal foods, fortified foods or a supplement are the safe route — see the Supplementation & Forms section below and our Vitamin B12 page.
4. Deficiency
There is no distinct human "cobalt deficiency" the way there is an iron or zinc deficiency: because cobalt's only role in people is to be the core of B12, a shortage of cobalt-as-B12 simply is vitamin B12 deficiency, producing megaloblastic anemia and nerve damage. (True cobalt deficiency is a veterinary problem in grazing livestock whose gut bacteria need soil cobalt to make their own B12 — not a human dietary need.) For a full, patient-friendly guide to the symptoms, causes, and treatment, see Cobalt Deficiency: What the Evidence Shows and our detailed Vitamin B12 page.
5. Recommended Intake
There is no Recommended Dietary Allowance (RDA) for elemental cobalt, and no official "adequate intake" figure for the inorganic metal. This is a direct consequence of everything above: since the human requirement is for cobalt locked inside vitamin B12, intake guidance is given entirely through the B12 recommendation. National nutrition bodies set a B12 target, not a cobalt target.
Intake expressed as vitamin B12
- The U.S. RDA for vitamin B12 is about 2.4 micrograms (µg) per day for most adults.
- It rises modestly in pregnancy (about 2.6 µg/day) and breastfeeding (about 2.8 µg/day).
- Because absorption efficiency falls as the dose rises (intrinsic-factor-mediated uptake saturates at roughly 1.5–2 µg per meal), people who get B12 from supplements often take far larger amounts so that a small fraction is absorbed by simple diffusion.
For context, the cobalt atom is a tiny fraction of the B12 molecule by weight, so 2.4 µg of B12 contains only a few tenths of a microgram of cobalt as the vitamin. This vanishingly small "cobalt requirement" underscores why no one sets an intake target for the metal itself.
How much inorganic cobalt do we actually eat?
Separately from B12, ordinary diets contain some inorganic cobalt — from plant foods, water, and trace contamination — typically on the order of a few micrograms up to a couple of milligrams per day, with most estimates landing somewhere between about 5 and 40 µg/day in Western diets. This inorganic cobalt is not nutritionally useful to humans (we cannot turn it into B12), and at these everyday levels it is not considered harmful. It only becomes a concern at the far higher exposures discussed in the next two sections — from cobalt supplements, industrial dust, contaminated drinks, or wearing metal implants. In short: aim for adequate B12; ignore "cobalt" as a separate intake goal.
6. Supplementation & Forms
The right way to "supplement cobalt" is to supplement vitamin B12 — never inorganic cobalt salts. Any cobalt your body can actually use must arrive already built into the cobalamin molecule. A B12 supplement delivers exactly that; a cobalt-salt supplement delivers a toxic metal with no nutritional benefit.
The useful forms — all are vitamin B12
- Cyanocobalamin: the most common, most stable, and cheapest form, used in most supplements and fortified foods. The body removes the cyanide group (a trivial amount, harmless at these doses) and converts it to the active forms.
- Methylcobalamin: a naturally occurring active form (the one used by methionine synthase), popular in supplements.
- Hydroxocobalamin: a form often given by injection, valued for its long retention in the body; it is also used (in much larger doses) as an antidote for cyanide poisoning.
- Adenosylcobalamin (dibencozide): the mitochondrial active form, sometimes sold in supplements.
All of these are appropriate ways to obtain cobalt-as-B12, whether by mouth (tablets, sublingual lozenges, fortified foods) or by injection when absorption is impaired. Doses for correcting deficiency are far larger than the 2.4 µg RDA — oral regimens of 500–1,000 µg/day and injection schedules are common — because B12 has an enormous safety margin and poor absorption at low doses.
Do not take inorganic cobalt supplements
Cobalt salts (cobalt chloride, cobalt sulfate, cobalt gluconate) have occasionally been sold or promoted to "boost energy," "build red blood cells," or enhance athletic performance. Avoid them. They cannot be converted into B12, they provide no genuine benefit, and — as the next section details — they are clearly toxic. The idea that cobalt salts raise red-cell counts is technically true (cobalt stimulates erythropoietin) but is exactly the mechanism behind their danger, and it is now classed as blood doping. Historically, cobalt chloride was even used as a medical treatment for stubborn anemias in the 1950s, until the cardiac and thyroid toxicity made the risk plainly unacceptable. There is no modern, legitimate role for swallowing cobalt as a nutrient. If you want the benefits of cobalt, eat B12-containing foods or take a B12 supplement.
7. Toxicity & Upper Limit
This is where cobalt's dual nature comes fully into view. There is no nutritional Tolerable Upper Intake Level (UL) for cobalt because there is no nutritional requirement to bound — but inorganic cobalt is unambiguously toxic in excess. The dose and route matter enormously: micrograms of cobalt sealed inside B12 are essential, while milligrams of free cobalt circulating in the blood are dangerous. Real-world poisoning has caused epidemics of heart failure (the 1960s cobalt-beer cardiomyopathy), systemic illness from worn metal-on-metal hip implants (arthroprosthetic cobaltism: cardiomyopathy, hypothyroidism, vision/hearing loss, neuropathy), occupational hard-metal lung disease, contact dermatitis, and blood doping via cobalt's stimulation of erythropoietin.
For a full, patient-friendly guide to the symptoms, causes, blood-cobalt thresholds, and treatment, see Cobalt Toxicity: Symptoms, Causes, and Risks.
8. Special Considerations
The honest, practical bottom line on cobalt is short and worth repeating: get your cobalt as vitamin B12, and never supplement the inorganic metal. Everything good cobalt does for you, it does from inside the cobalamin molecule; everything dangerous it does, it does when it runs free. Holding those two facts together is the whole story.
Who should pay extra attention
- Vegans, strict vegetarians, and people who avoid fortified foods. Their risk is B12 deficiency, not cobalt deficiency. The plant cobalt they eat cannot be converted to B12, so a reliable B12 source (fortified foods or a supplement) is important. See Vitamin B12.
- Older adults and people with absorption problems. Pernicious anemia, gastric or bowel surgery, and long-term use of metformin or acid-suppressing drugs all impair B12 absorption and may call for higher-dose oral B12 or injections.
- People with metal-on-metal hip implants. Anyone with such an implant who develops unexplained heart failure, an enlarging thyroid or new hypothyroidism, vision or hearing loss, or numbness, tremor, memory, or mood changes should ask a clinician to check blood cobalt and review the implant. Catching arthroprosthetic cobaltosis early — and revising the implant if needed — can halt or reverse the damage.
- Workers in hard-metal, grinding, pigment, and battery industries. Inhaled cobalt dust and skin contact are the main hazards; dust controls, ventilation, and avoiding skin exposure matter, and a cobalt-allergic rash should prompt evaluation.
- Athletes. Cobalt is a banned doping agent and a genuine poison at performance-"enhancing" doses — there is no safe way to use it for an edge.
Putting the dual nature in perspective
Cobalt is one of the clearest examples in all of nutrition of a substance whose value depends entirely on its chemical packaging and dose. Sealed inside vitamin B12 at the level of a few micrograms, it is irreplaceable — the literal core of the molecule that keeps our blood and nerves healthy. Set loose as a salt or worn off a metal implant at the level of milligrams in the bloodstream, it can damage the heart, thyroid, nerves, eyes, ears, and lungs. The site's broader pages on minerals and toxic minerals place cobalt alongside other elements that share this Jekyll-and-Hyde quality, and the lab tests section covers the blood and urine measurements used to tell the difference between safe and harmful exposure. When in doubt, the rule is simple: cobalt belongs in your B12, not in a supplement bottle.
9. Key Research Papers
- Green R, Allen LH, Bjørke-Monsen AL, et al. Vitamin B12 deficiency. Nature Reviews Disease Primers. 2017;3:17040. doi:10.1038/nrdp.2017.40
- Stabler SP. Vitamin B12 Deficiency. New England Journal of Medicine. 2013;368(2):149–160. doi:10.1056/NEJMcp1113996
- Froese DS, Banerjee R. Human B12-dependent enzymes: Methionine synthase and Methylmalonyl-CoA mutase. Methods in Enzymology. 2022;668:309–326. doi:10.1016/bs.mie.2021.12.012
- Yamada K. Cobalt: Its Role in Health and Disease. In: Metal Ions in Life Sciences, vol. 13. 2013:295–320. doi:10.1007/978-94-007-7500-8_9
- Leyssens L, Vinck B, Van Der Straeten C, Wuyts F, Maes L. Cobalt toxicity in humans — A review of the potential sources and systemic health effects. Toxicology. 2017;387:43–56. doi:10.1016/j.tox.2017.05.015
- Morin Y, Daniel P. Quebec Beer-Drinkers' Cardiomyopathy: Etiological Considerations. JAMA. 1967;202(13):1145–1146. doi:10.1001/jama.1967.03130260067015
- Alexander CS. Cobalt-beer cardiomyopathy: A clinical and pathologic study of twenty-eight cases. The American Journal of Medicine. 1972;53(4):395–417. doi:10.1016/0002-9343(72)90136-2
- Packer M. Cobalt Cardiomyopathy: A Critical Reappraisal in Light of a Recent Resurgence. Circulation: Heart Failure. 2016;9(12):e003604. doi:10.1161/CIRCHEARTFAILURE.116.003604
- Tower SS. Arthroprosthetic cobaltism: neurological and cardiac manifestations in two patients with metal-on-metal arthroplasty. Journal of Bone and Joint Surgery. 2010;92(17):2847–2851. doi:10.2106/JBJS.J.00125
- Nemery B, Verbeken EK, Demedts M. Giant cell interstitial pneumonia (hard metal lung disease, cobalt lung). Seminars in Respiratory and Critical Care Medicine. 2001;22(4):435–448. doi:10.1055/s-2001-17386
- Hindsén M. Allergic contact dermatitis from cobalt in jewellery. Contact Dermatitis. 2005;53(6):350. doi:10.1111/j.0105-1873.2005.0592a.x
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Cobalt. U.S. Department of Health and Human Services, Public Health Service. atsdr.cdc.gov/toxprofiles/tp33.pdf
- National Institutes of Health, Office of Dietary Supplements. Vitamin B12 — Health Professional Fact Sheet. ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional
- Medicines and Healthcare products Regulatory Agency (MHRA). Medical Device Alert: All metal-on-metal (MoM) hip replacements — updated advice for follow-up of patients. gov.uk — MoM hip replacement guidance
Connections
- Cobalt Deficiency: What the Evidence Shows
- Cobalt Toxicity: Symptoms, Causes, and Risks
- Vitamin B12 (Cobalamin)
- All Minerals
- Toxic Minerals
- Iron
- Copper
- Manganese
- Zinc
- Nickel
- Heavy Metals
- Cardiomyopathy
- Hypothyroidism
- Anemia
- Lab Tests