Cobalt Toxicity: Metal Implants and Inhalation
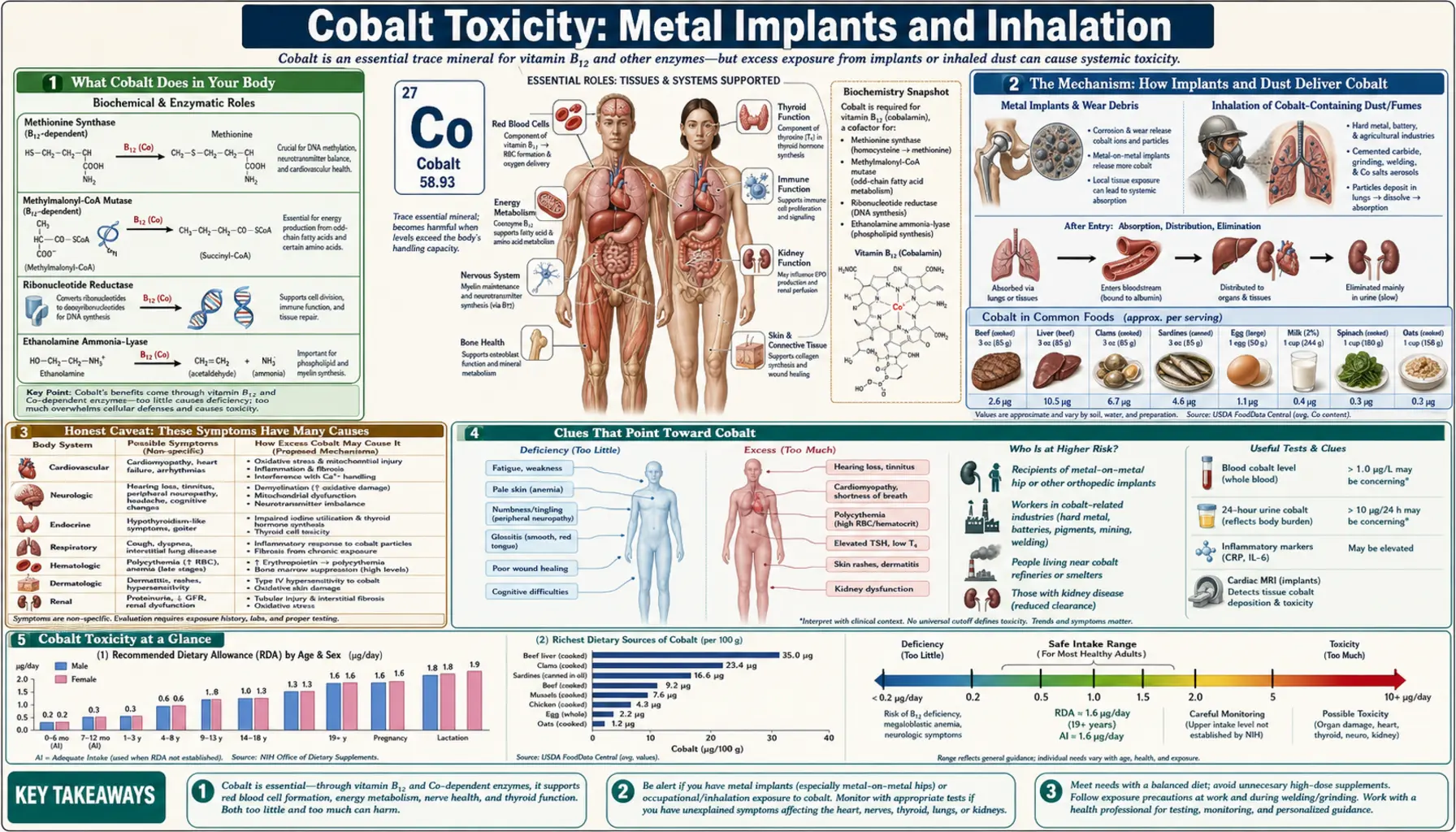
Cobalt is an essential trace mineral — the metal at the heart of vitamin B12 — and getting too much of it from food or ordinary supplements is essentially impossible. The handful of people who develop genuine cobalt toxicity get there by two very specific routes: a failing metal-on-metal hip implant that grinds cobalt particles into the bloodstream, or years of breathing cobalt-laden dust at work, especially in the “hard metal” (tungsten carbide) and diamond-polishing trades. This page is about those two exposures. It is honest about how rare and how non-specific the symptoms are — tiredness, breathlessness, and a failing heart have a hundred more common causes — while explaining the real mechanisms, the clues that should make a doctor think of cobalt, and exactly when to seek care.
Table of Contents
- What Cobalt Toxicity Feels Like
- The Mechanism: How Implants and Dust Deliver Cobalt
- Honest Caveat: These Symptoms Have Many Causes
- Clues That Point Toward Cobalt
- The Two Real Causes: Implants and Inhalation
- Getting Checked
- How Cobalt Excess Is Managed
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Cobalt Toxicity Feels Like
The first thing to understand about cobalt toxicity is that most people exposed to cobalt never get it, and when it does occur it builds up slowly and quietly. There is no sudden, dramatic “cobalt poisoning” in everyday life. Instead, over months to years, a small number of people with a high-wear metal hip or a dusty occupation accumulate enough cobalt to disturb several organs at once — and even then the early signs are vague enough to be blamed on aging, stress, or an unrelated illness.
When symptoms do appear, they tend to fall into a recognizable but scattered pattern, because cobalt does not target one organ. The two exposure routes also differ in which organ complains first.
From a failing hip implant (cobalt absorbed into the blood), the reported features — collectively nicknamed arthroprosthetic cobaltism — can include:
- The hip itself. New or worsening pain, swelling, clicking, or a sense of instability around a hip that was previously fine — often the earliest and most useful warning, because it points straight to the implant.
- Heart. Breathlessness on exertion, swelling of the ankles, and fatigue from a weakening heart muscle (cardiomyopathy) — covered in depth on the companion page, Cobalt Toxicity and the Heart.
- Nerves and senses. Ringing in the ears or hearing loss, changes in vision or color perception, numbness or tingling, tremor, and difficulty with balance or coordination.
- Thyroid. Sluggishness, weight gain, cold intolerance, or a swelling in the neck (goiter), because cobalt can interfere with the thyroid — see hypothyroidism.
- General. Fatigue, low mood or “brain fog,” and sometimes a skin rash.
From inhaled cobalt dust at work, the lungs and airways usually complain first:
- A dry, persistent cough and breathlessness that creep up over months and are often worse at work — the hallmark of hard metal lung disease.
- Wheeze, chest tightness, and work-related asthma that eases on weekends or holidays and flares again on returning to the job.
- Reduced exercise tolerance and, in advanced disease, scarring (fibrosis) of the lungs that does not fully reverse.
None of these symptoms, on their own, says “cobalt.” What makes a doctor suspect it is the combination plus the exposure — a recent metal hip, or years in a tungsten-carbide tool shop, diamond-polishing workshop, or cobalt refinery. That context is everything, and the clues section below explains exactly when the picture should raise a flag.
The Mechanism: How Implants and Dust Deliver Cobalt
To make sense of why cobalt harms so many organs, it helps to follow how it gets into the body in the first place — because the two routes are completely different, yet they converge on the same handful of biochemical mischief.
Route one: the grinding hip. Some hip replacements used a metal-on-metal bearing — a cobalt-chromium ball rotating inside a cobalt-chromium cup. Think of it like two hardened steel surfaces rubbing together millions of times. When the fit is good, wear is minimal; but when the components are positioned poorly, mismatched, or simply wear out, the surfaces shed a fine spray of metal debris — particles and dissolved cobalt and chromium ions — into the surrounding tissue. The body cannot wall all of it off. Some provokes a destructive local reaction (forming fluid collections and soft-tissue masses sometimes called pseudotumors), and some is absorbed into the bloodstream, where blood cobalt levels climb. The more the joint wears, the more cobalt enters circulation — which is why a loosening, painful, or malpositioned metal-on-metal hip is the classic setup for systemic cobaltism.
Route two: the dusty workshop. “Hard metal” is tungsten carbide cemented together with cobalt — the material in industrial drill bits, saw tips, and grinding wheels. Workers who machine, grind, or sharpen these tools, along with diamond-disc polishers and cobalt refinery staff, breathe in cobalt-containing dust and aerosol. Inhaled fine particles deposit deep in the lungs, where cobalt is slowly released. Here the lung tissue takes the brunt before much cobalt ever reaches the rest of the body, which is why inhalation tends to cause respiratory disease rather than the multi-organ picture seen with implants.
Why one metal damages so many organs. Once cobalt is loose in cells, it behaves like a chemical impostor and a saboteur. An analogy: imagine cobalt as a counterfeit key that fits several different locks just well enough to jam them.
- It imitates low oxygen. Cobalt stabilizes a cellular oxygen sensor (hypoxia-inducible factor), tricking cells into behaving as if they are starved of oxygen even when they are not — one reason cobalt was historically (and dangerously) misused to boost red-blood-cell production.
- It poisons energy production. Cobalt interferes with mitochondria — the cell's power plants — and generates damaging free radicals (oxidative stress). Heart muscle and nerve cells, which burn enormous amounts of energy, are especially vulnerable, which helps explain the cardiomyopathy and the nerve and hearing problems.
- It displaces other metals. Cobalt can elbow aside calcium and other essential metals at the proteins that depend on them, disturbing how cells signal and contract.
- It blocks the thyroid and provokes the immune system. Cobalt can impair iodine uptake by the thyroid, and inhaled cobalt acts as an allergen that drives occupational asthma and the inflammatory lung scarring of hard metal disease.
So the “counterfeit key” jams the oxygen sensor, the power plants, the metal-dependent machinery, the thyroid, and the immune system — and the organs that lean hardest on those systems (heart, nerves, ears, thyroid, lungs) are the ones that fail first. This is why cobalt toxicity looks like several unrelated illnesses at once rather than a single tidy syndrome.
Honest Caveat: These Symptoms Have Many Causes
This is the most important section to read before worrying that your symptoms mean cobalt toxicity. Cobalt toxicity is genuinely uncommon, and every one of its symptoms is far more often caused by something else. The honest framing matters because anxiety about implants is widespread, and the symptoms are exactly the everyday complaints that send people to the doctor for ordinary reasons.
- Fatigue and brain fog are among the most common symptoms in all of medicine — thyroid disease, anemia, sleep problems, depression, and dozens of other conditions cause them long before cobalt would.
- Breathlessness and ankle swelling usually stem from common heart and lung disease, weight, or deconditioning — not metal poisoning.
- A chronic cough in a worker is far more often from smoking, asthma, infection, or other dust exposures than from cobalt specifically.
- Hearing changes, tinnitus, numbness, and tremor have long lists of ordinary causes — age, noise, diabetes, medications, vitamin B12 issues, and more.
- Hypothyroid-type symptoms are usually ordinary autoimmune thyroid disease.
Two further honesty points. First, a high blood cobalt level by itself does not equal poisoning. Plenty of people with metal-on-metal hips have raised cobalt readings and feel completely well; the number must be interpreted alongside symptoms and the state of the joint. Second, having any metal implant is not the same as having a high-wear metal-on-metal bearing — ordinary hip and knee replacements, plates, and screws are not the concern here. The point of this page is not to make you fear a symptom or an implant, but to make sure cobalt is considered in the rare person who has both the right exposure and the right pattern. When that combination is absent, cobalt is almost never the answer.
Clues That Point Toward Cobalt
If the symptoms are so non-specific, what tips the balance toward investigating cobalt? It is almost always the exposure plus a suggestive pattern, not any single complaint. The features below, taken together, are what should prompt a doctor to check.
- A metal-on-metal hip — especially one that hurts. The single biggest clue is a cobalt-chromium hip resurfacing or large-head metal-on-metal replacement that has become painful, swollen, clicking, or unstable. New hip symptoms after such an implant warrant evaluation regardless of any other complaint.
- Multiple organs complaining at once. A combination that crosses unrelated systems — for instance heart failure plus new hearing loss plus thyroid problems plus a bad hip — is far more suggestive than any one symptom alone. It is the constellation, appearing over months in someone with the exposure, that raises the flag.
- A revision of a broken ceramic implant. A specific high-risk story is a prior ceramic hip that fractured and was replaced with a metal-on-metal or metal-on-polyethylene bearing: hard ceramic fragments left behind can grind the new metal head aggressively and release large amounts of cobalt.
- Respiratory symptoms tied to a dusty job. For inhalation, the clue is a cough or breathlessness that tracks the work week — better on holidays, worse back at the bench — in someone grinding tungsten-carbide tools, polishing diamond, or working in a cobalt plant.
- Symptoms that ease when exposure stops. Improvement after a hip is revised, or after time away from the dusty workplace, supports the link.
When these clues line up, a focused work-up (next sections) can confirm or exclude cobalt. The heart manifestation in particular has its own dedicated page; if breathlessness and a weakening heart are the dominant problem, see Cobalt Toxicity and the Heart (Cardiomyopathy) rather than duplicating it here.
The Two Real Causes: Implants and Inhalation
Because cobalt toxicity is essentially confined to these two routes, it is worth understanding each in a little more depth — including who is at risk and why the everyday worry (diet, supplements, ordinary implants) is not.
Metal-on-metal hip implants
Metal-on-metal hip resurfacings and large-diameter metal-on-metal total hips were used widely in the 2000s, on the theory that hard metal bearings would last longer and dislocate less. Large registry data later told a different story: stemmed metal-on-metal hips failed and needed revision more often than other bearing types, and the failures were frequently linked to wear, local soft-tissue reactions, and rising metal-ion levels. As a result, these bearings were largely abandoned, and health authorities introduced surveillance programs for people who already had one — periodic symptom checks, blood cobalt and chromium measurements, and imaging of the joint.
The key risk factors for systemic cobalt release are a poorly positioned or worn bearing, a large femoral head size, component loosening, and the special case of a revised fractured-ceramic implant noted above. Importantly, the great majority of people with these hips do not develop systemic cobaltism; the severe multi-organ cases described in the medical literature are rare and tend to involve very high wear. Still, because a worn metal-on-metal hip is the one setup that reliably drives blood cobalt up, anyone who has one should stay in their surveillance program and report new hip or whole-body symptoms promptly.
Occupational inhalation (“hard metal” and related dusts)
The other route is breathing cobalt dust over a working lifetime. The classic settings are the hard metal industry (manufacturing and sharpening tungsten-carbide cutting tools), diamond polishing (cobalt-containing grinding discs), and cobalt production and refining. Chronic inhalation causes two overlapping problems: an allergic, asthma-like airway disease (hard metal asthma) that flares with exposure, and a deeper inflammatory and scarring lung disease — hard metal lung disease, whose hallmark on biopsy is an unusual pattern called giant cell interstitial pneumonia. Epidemiological surveys of exposed workers have documented excess respiratory symptoms and reduced lung function compared with unexposed workers, and the risk rises with the intensity and duration of dust exposure.
Modern workplaces control this risk with dust extraction, enclosed processes, respiratory protection, and exposure monitoring — which is why severe cases are far less common than they once were. The people still at risk are those with poor controls or long histories in the trade.
What is not a cause
It is worth stating plainly: you cannot get cobalt toxicity from a normal diet (cobalt in food is bound up almost entirely as vitamin B12), from standard B12 supplements, or from ordinary orthopedic hardware such as a routine hip or knee replacement, a plate, or screws. The discredited historical episode of cobalt added to beer as a foam stabilizer, which caused an outbreak of heart failure in heavy drinkers in the 1960s, is a separate story of a deliberate additive in enormous combined doses — not something that happens today. (That episode is discussed on the cardiomyopathy page.)
Getting Checked
Diagnosing cobalt toxicity is really an exercise in connecting an exposure to a pattern, supported by a few specific tests. No single result proves it; the diagnosis is clinical, with the numbers as supporting evidence.
The history comes first. The most valuable step is simply establishing the exposure: do you have a metal-on-metal hip (and is it symptomatic), or a work history of cobalt dust? Everything else builds on that.
Blood cobalt (and chromium) levels. For people with metal-on-metal hips, measuring whole-blood cobalt and chromium is the central test. Rising or markedly elevated levels — tracked over time, not from a single snapshot — suggest a wearing bearing and prompt closer attention. But, as the honesty section stressed, a raised level alone is not a diagnosis of poisoning; many people with high readings feel well. The level is interpreted alongside symptoms and imaging.
Imaging the joint. Specialized imaging — metal-artifact-reduction MRI or ultrasound — looks for the soft-tissue reactions and fluid collections (pseudotumors) and for signs of a worn or loose implant. This tells the surgeon whether the bearing is the source.
Targeted organ tests. Depending on symptoms, a clinician may add an Comprehensive Metabolic Panel and other bloods, an echocardiogram to assess the heart muscle if cardiomyopathy is suspected, thyroid function tests, and hearing and vision testing if those senses are affected.
For inhalation disease, the work-up is led by a respiratory specialist and looks different: lung-function tests, a CT scan of the chest, and sometimes a lung biopsy — the finding of giant cell interstitial pneumonia is strongly tied to cobalt and hard metal exposure. A careful occupational history, again, is what frames the whole investigation.
How Cobalt Excess Is Managed
The single most important principle of treatment is the same one that defines the disease: remove the source of cobalt. Because the toxicity comes from an ongoing exposure rather than a one-time dose, stopping the source is both the treatment and, often, the cure. As cobalt input falls, blood levels decline and many of the reversible problems improve.
- Revising the implant. For a high-wear metal-on-metal hip causing rising cobalt and symptoms, the definitive step is revision surgery — replacing the metal-on-metal bearing with a different combination of materials and clearing out the reactive tissue. This is the orthopedic decision that actually stops the cobalt at its origin. In published cases, blood cobalt falls after revision and several symptoms (including heart and nerve features) can partially or substantially recover, though some damage — particularly advanced cardiomyopathy or established hearing loss — may be permanent.
- Leaving the dusty environment. For inhalation disease, removal from cobalt exposure is the cornerstone — reassignment away from the dust, far better workplace controls, and respiratory protection. Early hard metal lung disease can improve once exposure stops; established fibrosis may not fully reverse, but halting exposure prevents further progression. Asthma-type disease is managed with standard inhaler therapy plus avoidance.
- Supporting the affected organs. Treatment otherwise targets the organ that is failing: standard heart-failure therapy for cardiomyopathy, thyroid hormone replacement for an underactive thyroid, and respiratory care for the lungs. These manage the consequences while source-removal addresses the cause.
- A note on chelation. Drugs that bind metals (chelation) are sometimes considered in severe poisoning, but their role in cobalt toxicity is uncertain and not routine; the literature does not establish a clear benefit, and removing the source remains the priority. Chelation is a specialist decision in selected severe cases, not a standard or self-directed treatment.
The encouraging message is that, caught before organ damage becomes fixed, cobalt toxicity is one of the more reversible metal exposures — precisely because the fix is to stop the source rather than to undo a permanent injury.
When to Seek Care / Red Flags
Cobalt toxicity is rare and usually develops slowly, so most of the time the right move is a planned visit rather than an emergency. But some features should prompt urgent attention, and the exposure history determines how seriously a symptom should be taken.
- Get emergency care for severe breathlessness, breathlessness at rest or when lying flat, chest pain, fainting, or a racing or pounding heartbeat — these can signal heart failure or a dangerous rhythm, whatever the cause, and need assessment now (see also arrhythmia and cardiomyopathy).
- See your surgeon or doctor promptly if you have a metal-on-metal hip and develop new hip pain, swelling, clicking, or instability, or new whole-body symptoms such as unexplained breathlessness, hearing or vision changes, numbness, or marked fatigue. Do not wait for a routine review — report it.
- Stay in your surveillance program. If you have a metal-on-metal implant, keep the recommended follow-up appointments and blood-metal checks even when you feel well; the point is to catch a rising trend before it causes harm.
- Raise it with an occupational-health or respiratory clinician if you work with cobalt or hard metal dust and have a persistent cough, wheeze, or breathlessness — particularly if it improves away from work. Early recognition can prevent irreversible lung scarring.
- Do not start chelation or “detox” products on your own. Cobalt toxicity is managed by removing the source under specialist care, not by over-the-counter remedies.
The unifying rule: it is the exposure plus a new or worsening symptom that should trigger care. A symptom on its own, with no metal-on-metal implant and no cobalt-dust job, almost never points to cobalt — but with that exposure present, it deserves a prompt, specific look.
Key Research Papers
- Leyssens L, Vinck B, Van Der Straeten C, et al. (2017). Cobalt toxicity in humans — A review of the potential sources and systemic health effects. Toxicology;387:43-56. — DOI: 10.1016/j.tox.2017.05.015
- Zywiel MG, Cherian JJ, Banerjee S, et al. (2016). Systemic cobalt toxicity from total hip arthroplasties: review of a rare condition. The Bone & Joint Journal;98-B(1):14-20. — DOI: 10.1302/0301-620X.98B1.36712
- Tower SS (2010). Arthroprosthetic Cobaltism: Neurological and Cardiac Manifestations in Two Patients with Metal-on-Metal Arthroplasty. Journal of Bone and Joint Surgery;92(17):2847-2851. — DOI: 10.2106/JBJS.J.00125
- Devlin JJ, Pomerleau AC, Brent J, et al. (2013). Clinical Features, Testing, and Management of Patients with Suspected Prosthetic Hip-Associated Cobalt Toxicity: a Systematic Review. Journal of Medical Toxicology;9(4):405-415. — DOI: 10.1007/s13181-013-0320-0
- Machado C, Appelbe A, Wood R (2012). Arthroprosthetic Cobaltism and Cardiomyopathy. Heart, Lung and Circulation;21(11):759-760. — DOI: 10.1016/j.hlc.2012.03.013
- Smith AJ, Dieppe P, Vernon K, et al. (2012). Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. The Lancet;379(9822):1199-1204. — DOI: 10.1016/S0140-6736(12)60353-5
- Cohen D (2012). How safe are metal-on-metal hip implants? BMJ;344:e1410. — DOI: 10.1136/bmj.e1410
- McMinn DJW, Snell KIE, Daniel J, et al. (2012). Mortality and implant revision rates of hip arthroplasty in patients with osteoarthritis: registry based cohort study. BMJ;344:e3319. — DOI: 10.1136/bmj.e3319
- Nemery B, Verbeken EK, Demedts M (2001). Giant Cell Interstitial Pneumonia (Hard Metal Lung Disease, Cobalt Lung). Seminars in Respiratory and Critical Care Medicine;22(4):435-448. — DOI: 10.1055/s-2001-17386
- Shirakawa T, Kusaka Y, Fujimura N, et al. (1989). Occupational Asthma from Cobalt Sensitivity in Workers Exposed to Hard Metal Dust. Chest;95(1):29-37. — DOI: 10.1378/chest.95.1.29
- Swennen B, Buchet JP, Stanescu D, et al. (1993). Epidemiological survey of workers exposed to cobalt oxides, cobalt salts, and cobalt metal. Occupational and Environmental Medicine;50(9):835-842. — DOI: 10.1136/oem.50.9.835
- Du Z, Liu X, Wang Z, et al. (2021). Cobalt-related interstitial lung disease or hard metal lung disease: A case series of Chinese workers. Toxicology and Industrial Health;37(5):280-288. — DOI: 10.1177/07482337211000989
- Linna A, Uitti J, Oksa P, et al. (2020). Effects of occupational cobalt exposure on the heart in the production of cobalt and cobalt compounds: a 6-year follow-up. International Archives of Occupational and Environmental Health;93(3):365-374. — DOI: 10.1007/s00420-019-01488-3
- Morin Y, Daniel P (1967). Quebec Beer-Drinkers' Cardiomyopathy: Etiological Considerations. JAMA;202(13):1145. — DOI: 10.1001/jama.1967.03130260067015
PubMed Topic Searches
- PubMed — Arthroprosthetic cobaltism and metal-on-metal hips
- PubMed — Systemic cobalt toxicity from hip implants
- PubMed — Hard metal lung disease (cobalt lung)
- PubMed — Cobalt occupational asthma and hard metal dust
- PubMed — Blood cobalt/chromium surveillance after arthroplasty
Connections
- Cobalt Toxicity Hub
- Cobalt Toxicity and the Heart (Cardiomyopathy)
- Cobalt Overview
- Vitamin B12
- Chromium
- Iron
- Toxic Minerals
- Orthopedics
- Cardiomyopathy
- Heart Failure
- Arrhythmia
- Pulmonology
- Hypothyroidism
- Comprehensive Metabolic Panel
- Heavy Metals