Hypercalcemia (High Calcium): Constipation and Digestive
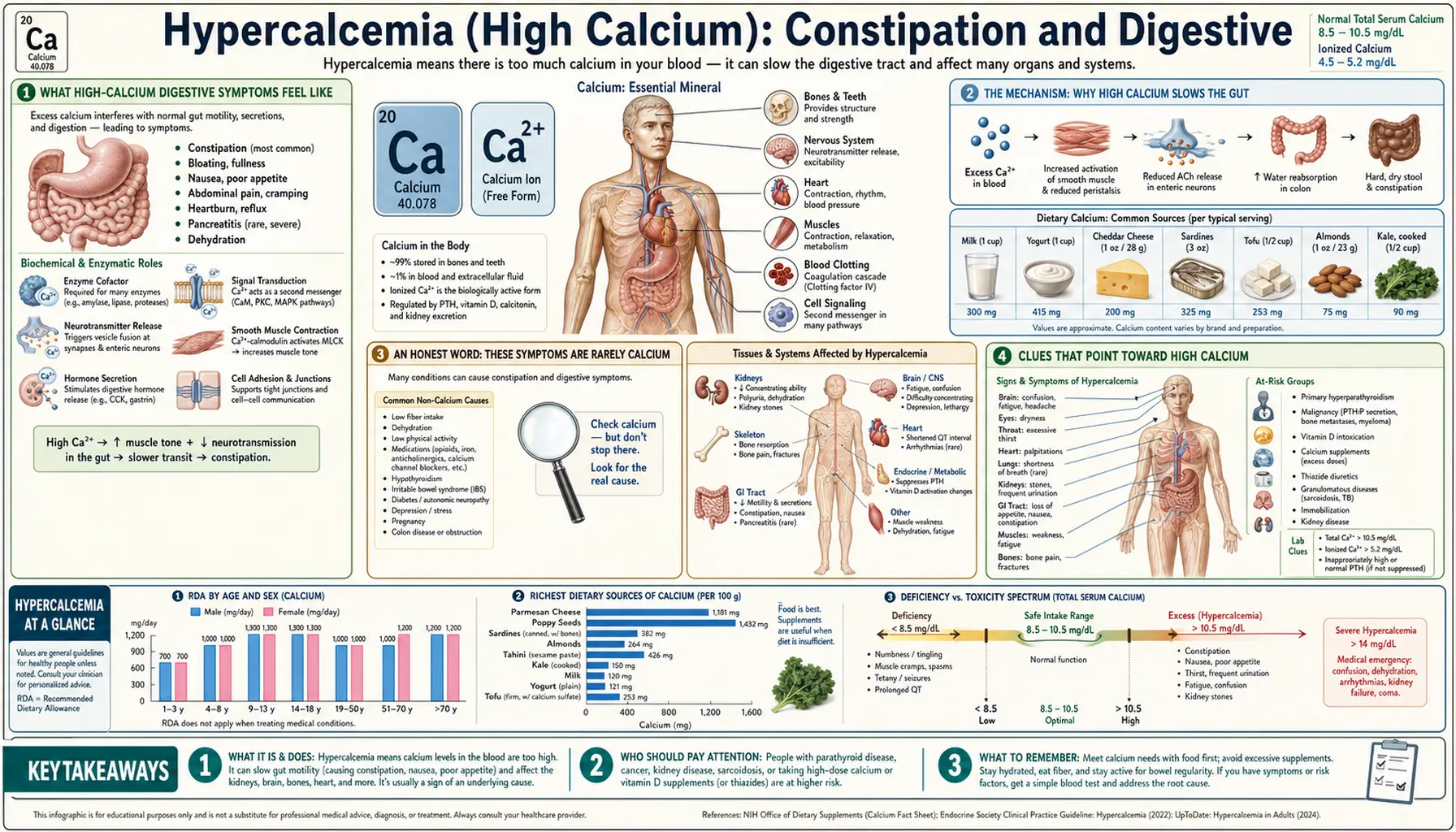
When calcium climbs too high in the blood — a condition called hypercalcemia — the digestive tract often slows down. The first signs are usually quiet and easy to dismiss: a fading appetite, queasiness, a vague stomach ache, and stubborn constipation. The old medical mnemonic for hypercalcemia — “stones, bones, groans, and psychiatric moans” — puts these abdominal “groans” right at the center, because high calcium genuinely quiets the muscle that moves food along the gut. The honest catch is that constipation, nausea, and poor appetite are some of the most common and non-specific complaints in all of medicine — a high calcium level is an uncommon cause, and these symptoms are far more often something ordinary. This page explains the digestive symptoms specifically: how they feel, the muscle mechanism behind them, why they almost never point to calcium on their own, and the few clues that should prompt a simple blood test.
Table of Contents
- What High-Calcium Digestive Symptoms Feel Like
- The Mechanism: Why High Calcium Slows the Gut
- An Honest Word: These Symptoms Are Rarely Calcium
- Clues That Point Toward High Calcium
- Common Causes of High Calcium
- A Note on Nausea, Vomiting, and Pancreatitis
- Getting Checked
- How High Calcium Is Corrected
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What High-Calcium Digestive Symptoms Feel Like
The digestive symptoms of high calcium tend to creep in slowly and stay vague, which is exactly why they are so easy to attribute to stress, diet, or simply getting older. When calcium rises gradually — the usual pattern — the gut quiets down in a cluster of related ways:
- Constipation. This is the classic gut symptom of hypercalcemia. Stools become harder, less frequent, and harder to pass; the bowel feels sluggish and incompletely emptied. It is constipation driven by slowed muscle, not by a lack of fiber, so it often does not respond well to the usual fiber-and-fluid advice while the calcium stays high.
- Loss of appetite. Food simply stops appealing. People describe feeling full after a few bites, having no interest in meals they used to enjoy, and sometimes losing weight without trying. (See also loss of appetite as a general symptom.)
- Nausea and occasional vomiting. A persistent queasiness sits in the background, sometimes tipping over into vomiting when calcium is higher. (See also nausea and vomiting.)
- Vague abdominal discomfort. A dull ache, bloating, or a generally “off” stomach — rarely sharp, rarely in one fixed spot.
These four travel together more often than alone, and they share a single explanation: the smooth muscle that propels food and waste through the digestive tract is being damped down. Constipation is usually the symptom people notice and remember; nausea and a poor appetite are the companions that make a high-calcium picture more likely than ordinary, isolated constipation.
A useful contrast: these are different symptoms from the fatigue, low mood, and mental fog that high calcium can also cause, and different again from the excessive thirst and bone pain of more advanced hypercalcemia. They frequently overlap, but this page is only about the digestive ones — the “groans” of the old mnemonic. When several of these clusters appear at once, the case for checking a calcium level grows stronger.
The Mechanism: Why High Calcium Slows the Gut
To understand why high calcium constipates, it helps to know that calcium is one of the body's master “on” switches. Inside every smooth-muscle cell — including the muscle wrapped around your intestines — a rise in calcium is the trigger that tells the cell to contract. The gut moves its contents along by peristalsis: coordinated, wave-like contractions of that smooth muscle, paced by the gut's own nerve network. Normal peristalsis depends on muscle cells that contract and then fully relax, over and over, in rhythm.
Here is the apparent paradox: if calcium is the contraction signal, why does too much of it slow the gut down rather than speed it up? The answer lies in how excitable nerve and muscle membranes are. Calcium in the blood sits on the outside of these cells and helps stabilize their electrical membranes — it raises the threshold a cell must cross before it will fire. When blood calcium climbs, that stabilizing effect strengthens: nerve and muscle membranes become less excitable and harder to trigger. The pacemaker signals that normally roll down the gut as smooth, propulsive waves become weak and poorly coordinated. The muscle is not paralyzed, but its rhythm is blunted, transit slows, and the result is sluggish motility — constipation, a heavy full stomach, and the queasy appetite-killing sense that nothing is moving.
An analogy. Picture the gut wall as a line of rowers pulling a boat, each stroke (a contraction) following the one before in a steady cadence set by a coxswain (the gut's pacemaker nerves). Calcium is the coxswain's drumbeat that times each pull. A normal beat keeps the strokes crisp and synchronized and the boat gliding forward. Flood the boat with so much “drumbeat” that the signal becomes a constant blare, and the rowers can no longer tell one stroke from the next — the cadence falls apart, the strokes go soft and ragged, and the boat slows to a drift. That drift is constipation. Quiet the blare back to a clean beat — bring blood calcium back into range — and the cadence returns, usually within days.
The same loss of membrane excitability that quiets the gut also helps explain why severe hypercalcemia produces sluggishness elsewhere — the muscles, the nerves, the kidneys, and the brain. The gut is simply one of the first and most noticeable places it shows. This is why the underlying biology of calcium signaling, governed by the parathyroid–vitamin D axis, sits at the root of the whole hypercalcemia picture rather than the gut alone.
An Honest Word: These Symptoms Are Rarely Calcium
This is the most important section on the page, and it cuts against the impulse to worry. Constipation, nausea, and a poor appetite are among the most common symptoms in all of medicine, and high calcium is an uncommon cause of them. If you are constipated, the odds overwhelmingly favor an ordinary explanation, not a problem with your calcium level. It would be a mistake to read this page and conclude that sluggish bowels mean hypercalcemia — they almost never do.
The far more likely causes of these same symptoms include:
- Low fiber, low fluid, and inactivity — the everyday reasons for constipation, and the first things to address. (See the general constipation symptom page.)
- Medications. Opioid pain relievers are a leading cause; so are many others, including — importantly — calcium-containing antacids and supplements themselves, iron tablets, some blood-pressure drugs, and certain antidepressants.
- Irritable bowel syndrome (IBS) and other functional gut disorders, which are extremely common.
- Slow-transit constipation and pelvic-floor problems, especially with age.
- An underactive thyroid (hypothyroidism), diabetes, and other metabolic conditions that slow the gut.
- Diet changes, travel, pregnancy, dehydration, and stress.
For nausea and poor appetite the list is even broader — viral illness, reflux, medication side effects, anxiety, and countless other causes far outnumber hypercalcemia. The point is not that high calcium never does this; it genuinely can, and the digestive symptoms are real. The point is one of proportion: these symptoms by themselves are weak evidence for high calcium. What changes the picture is the company they keep — the clues in the next section.
Clues That Point Toward High Calcium
If digestive symptoms alone rarely indicate hypercalcemia, what raises the suspicion enough to justify a calcium test? A few patterns shift the odds:
- The symptoms cluster. Constipation plus a fading appetite, nausea, and unexplained tiredness — appearing together over weeks — is more suggestive than constipation alone. Hypercalcemia rarely produces a single, isolated gut complaint.
- There is excessive thirst and frequent urination alongside. High calcium makes the kidneys spill water, causing thirst and copious urination. Constipation paired with relentless thirst and heavy urine output is a more telling combination (detailed on the thirst and bone pain page).
- Mental fog, low mood, or unusual fatigue have crept in too. The fatigue-and-confusion symptoms of high calcium often accompany the digestive ones.
- There is a kidney-stone history. Hypercalcemia is closely tied to kidney stones; new gut symptoms in someone who has passed stones deserve a calcium check.
- The person takes a lot of calcium or vitamin D. Heavy use of calcium-based antacids, calcium supplements, or high-dose vitamin D is a real and growing cause (see below).
- Standard constipation measures are not working. Constipation that ignores added fiber, fluids, and activity — particularly with the features above — is worth investigating beyond the gut.
None of these proves high calcium; each simply nudges a routine blood test from “unnecessary” toward “reasonable.” And the test is cheap, fast, and definitive — which is precisely why clinicians have a low threshold to order it when the clues line up.
Common Causes of High Calcium
When a high calcium level is found, the cause matters enormously, because the digestive symptoms are just the surface of very different underlying problems. Two causes account for the overwhelming majority of cases:
- Primary hyperparathyroidism. This is the single most common cause of high calcium in people who are otherwise well, especially women after menopause. One of the four tiny parathyroid glands in the neck develops a small benign growth that pumps out too much parathyroid hormone (PTH), which steadily pulls calcium out of the bones and into the blood. The calcium is often only mildly elevated and discovered on a routine panel, sometimes with nothing more than vague constipation, fatigue, or “not feeling right.”
- Cancer (hypercalcemia of malignancy). This is the most common cause of high calcium in people who are hospitalized or seriously ill. Certain cancers raise calcium — by secreting a PTH-like protein, by spreading to bone, or by other routes. Here the calcium tends to rise higher and faster, and the symptoms — nausea, vomiting, severe constipation, drowsiness — are usually more pronounced.
Other, less frequent causes include:
- Too much calcium or vitamin D from supplements and antacids. Swallowing large amounts of calcium-containing antacids together with extra calcium — classically for heartburn or bone health — can produce the calcium-alkali syndrome (the modern, far more common version of the old “milk-alkali syndrome”): high calcium, alkaline blood, and kidney strain. High-dose vitamin D can also push calcium up by increasing how much is absorbed from food. This is one of the few self-inflicted causes — and a reason to be honest about how much calcium one is actually taking.
- Prolonged immobilization, which releases calcium from unused bone.
- Granulomatous diseases such as sarcoidosis, and certain other endocrine and inherited conditions.
Sorting out which cause is at work is the real work after a high reading, and it usually turns on one simple follow-up test — the PTH level — described in the diagnosis section.
A Note on Nausea, Vomiting, and Pancreatitis
One uncommon but serious consequence of high calcium deserves a brief, separate mention so that severe abdominal symptoms are not waved off. Sustained or markedly elevated calcium can trigger acute pancreatitis — inflammation of the pancreas — which presents very differently from the quiet constipation described above. Pancreatitis causes severe, persistent upper-abdominal pain, often boring straight through to the back, with relentless nausea and vomiting, and it is a medical emergency.
The reason to flag it is the contrast: the everyday digestive face of hypercalcemia is mild and slow — sluggish bowels, a poor appetite, background queasiness. But intense, unremitting abdominal pain with vomiting is not the ordinary picture and should never be attributed to “just constipation.” That combination needs urgent in-person assessment, whatever the calcium level turns out to be. Hypercalcemia is only one of many causes of pancreatitis, but it is a recognized one, and it is the kind of symptom that moves a person from “book a blood test” to “be seen today” (see the red-flags section).
Getting Checked
Confirming high calcium is quick and inexpensive, and it rests on a routine blood test followed by one or two targeted follow-ups.
The first step is a blood test. A Comprehensive Metabolic Panel (CMP) — an ordinary blood draw — reports the total serum calcium directly, alongside kidney function and other electrolytes. The normal total calcium range is roughly 8.5–10.2 mg/dL (about 2.1–2.6 mmol/L), though exact ranges vary by laboratory. Because nearly half of the calcium in blood is bound to the protein albumin, a low albumin level can make the total calcium look falsely low and a high albumin can inflate it; clinicians either “correct” the calcium for albumin or measure the active ionized calcium directly when the picture is unclear. A single mildly high value is also commonly just repeated, because a tight tourniquet or lab variation can nudge the number.
If calcium is genuinely elevated, the pivotal next test is the parathyroid hormone (PTH) level, and it usually splits the diagnosis cleanly in two:
- A calcium that is high and a PTH that is high (or even “inappropriately normal”) points strongly to primary hyperparathyroidism — the parathyroid glands are driving it.
- A calcium that is high with a low, suppressed PTH points away from the parathyroids and toward another cause — most importantly cancer, or excess vitamin D, or a calcium-and-antacid load. The body has correctly shut its PTH off, so something else is pushing calcium up.
From there a clinician may add vitamin D levels, a urine calcium measurement, kidney imaging, or — if cancer is suspected — appropriate further evaluation. The key practical message is that a single inexpensive panel detects the problem, and a single follow-up hormone test usually reveals the cause.
How High Calcium Is Corrected
Treatment depends entirely on how high the calcium is and why. As the calcium falls back into range, the digestive symptoms lift — the gut's muscle regains its rhythm, appetite returns, nausea settles, and the bowels move again, often within a few days of the level normalizing. Fixing the constipation directly, while the calcium stays high, tends to disappoint; the durable fix is correcting the calcium.
- Mild elevation. Often no urgent treatment is needed beyond finding the cause. Simple, sensible measures help: stop unnecessary calcium supplements and calcium-based antacids, review the medication list, stay well hydrated, and keep moving rather than staying in bed. If primary hyperparathyroidism is the cause and it warrants treatment, the definitive fix is a minor operation to remove the overactive parathyroid gland — which resolves the calcium and its symptoms for good.
- Moderate to severe elevation. Higher levels — especially the rapid rises of hypercalcemia of malignancy — are treated more aggressively and usually in hospital. The cornerstone is intravenous fluids (normal saline) to rehydrate and help the kidneys flush calcium out. Medications called bisphosphonates reduce the release of calcium from bone over a day or two, and calcitonin can lower it more quickly for a short time. Other drugs and, for severe kidney failure, dialysis are used in selected cases.
- Treat the cause. Lowering the number once is not enough if the cause persists: removing an overactive parathyroid gland, treating an underlying cancer, or simply eliminating the excess calcium and vitamin D that produced a calcium-alkali load.
While calcium is being corrected, ordinary constipation relief is still reasonable — adequate fluids, gentle activity, and, if needed, a stool softener or laxative chosen with a clinician — but it is supportive, not the main event. The gut follows the calcium.
When to Seek Care / Red Flags
Most constipation, nausea, and poor appetite is benign and self-limited, and does not need urgent attention — but a few patterns warrant prompt or emergency care, whether or not calcium turns out to be the cause:
- Severe, persistent abdominal pain with vomiting — especially pain that bores through to the back — which can signal pancreatitis or another acute abdominal emergency. Seek care right away.
- Constipation with vomiting, a swollen abdomen, and no passage of gas or stool, which may mean a bowel obstruction — an emergency.
- Confusion, marked drowsiness, or difficulty staying awake alongside the digestive symptoms, which can indicate dangerously high calcium affecting the brain — get help urgently.
- Relentless thirst and heavy urination plus weakness and vomiting, the combination that suggests a severe hypercalcemic crisis with dehydration.
- Unexplained weight loss, blood in the stool, a change in bowel habit lasting weeks, or symptoms in someone over 50 with no prior history — not specific to calcium, but always worth timely evaluation.
- Known cancer, hyperparathyroidism, or kidney disease with new or worsening digestive symptoms — check a calcium level promptly.
For everyday, mild constipation with no alarm features, the sensible path is fiber, fluids, activity, a look at the medication and supplement list — and, if it persists or the clues above are present, a single inexpensive blood test to settle whether calcium is involved. Confirming or ruling out hypercalcemia takes one blood draw, and catching the cause early — whether a treatable parathyroid problem or something more serious — is the whole point of paying attention.
Key Research Papers
- Minisola S, Pepe J, Piemonte S, Cipriani C (2015). The diagnosis and management of hypercalcaemia. BMJ;350:h2723. — DOI: 10.1136/bmj.h2723
- Hutton E (2005). Evaluation and management of hypercalcemia. Journal of the American Academy of Physician Assistants;18(6):30-35. — DOI: 10.1097/01720610-200506000-00004
- Stewart AF (2005). Hypercalcemia Associated with Cancer. New England Journal of Medicine;352(4):373-379. — DOI: 10.1056/NEJMcp042806
- Goldner W (2016). Cancer-Related Hypercalcemia. Journal of Oncology Practice;12(5):426-432. — DOI: 10.1200/JOP.2016.011155
- Fraser WD (2009). Hyperparathyroidism. The Lancet;374(9684):145-158. — DOI: 10.1016/S0140-6736(09)60507-9
- Bilezikian JP, Brandi ML, Eastell R, et al. (2014). Guidelines for the Management of Asymptomatic Primary Hyperparathyroidism: Summary Statement from the Fourth International Workshop. The Journal of Clinical Endocrinology & Metabolism;99(10):3561-3569. — DOI: 10.1210/jc.2014-1413
- Patel AM, Goldfarb S (2010). Got Calcium? Welcome to the Calcium-Alkali Syndrome. Journal of the American Society of Nephrology;21(9):1440-1443. — DOI: 10.1681/ASN.2010030255
- Patel AM, Adeseun GA, Goldfarb S (2013). Calcium-Alkali Syndrome in the Modern Era. Nutrients;5(12):4880-4893. — DOI: 10.3390/nu5124880
- Goltzman D, Mannstadt M, Marcocci C (2018). Physiology of the Calcium-Parathyroid Hormone-Vitamin D Axis. Frontiers of Hormone Research;50:1-13. — DOI: 10.1159/000486060
- Bharucha AE, Lacy BE (2020). Mechanisms, Evaluation, and Management of Chronic Constipation. Gastroenterology;158(5):1232-1249. — DOI: 10.1053/j.gastro.2019.12.034
- Bharucha AE, Wald A (2019). Chronic Constipation. Mayo Clinic Proceedings;94(11):2340-2357. — DOI: 10.1016/j.mayocp.2019.01.031
- Bharucha AE, Dorn SD, Lembo A, Pressman A (2013). American Gastroenterological Association Technical Review on Constipation. Gastroenterology;144(1):218-238. — DOI: 10.1053/j.gastro.2012.10.028
PubMed Topic Searches
- PubMed — Hypercalcemia, constipation, and gastrointestinal symptoms
- PubMed — High calcium, smooth muscle, and gut motility
- PubMed — Primary hyperparathyroidism: symptoms and diagnosis
- PubMed — Calcium-alkali syndrome from supplements and antacids
- PubMed — Hypercalcemia and acute pancreatitis
Connections
- Hypercalcemia Symptom Hub
- Hypercalcemia and Kidney Stones
- Hypercalcemia and Fatigue & Confusion
- Hypercalcemia and Thirst & Bone Pain
- Calcium Overview
- Calcium and Bone Health
- Calcium and Muscle Function
- Magnesium
- Phosphorus
- Vitamin D
- Hyperparathyroidism
- Kidney Disease
- Gastroenterology
- Constipation
- Loss of Appetite
- Nausea & Vomiting
- Comprehensive Metabolic Panel