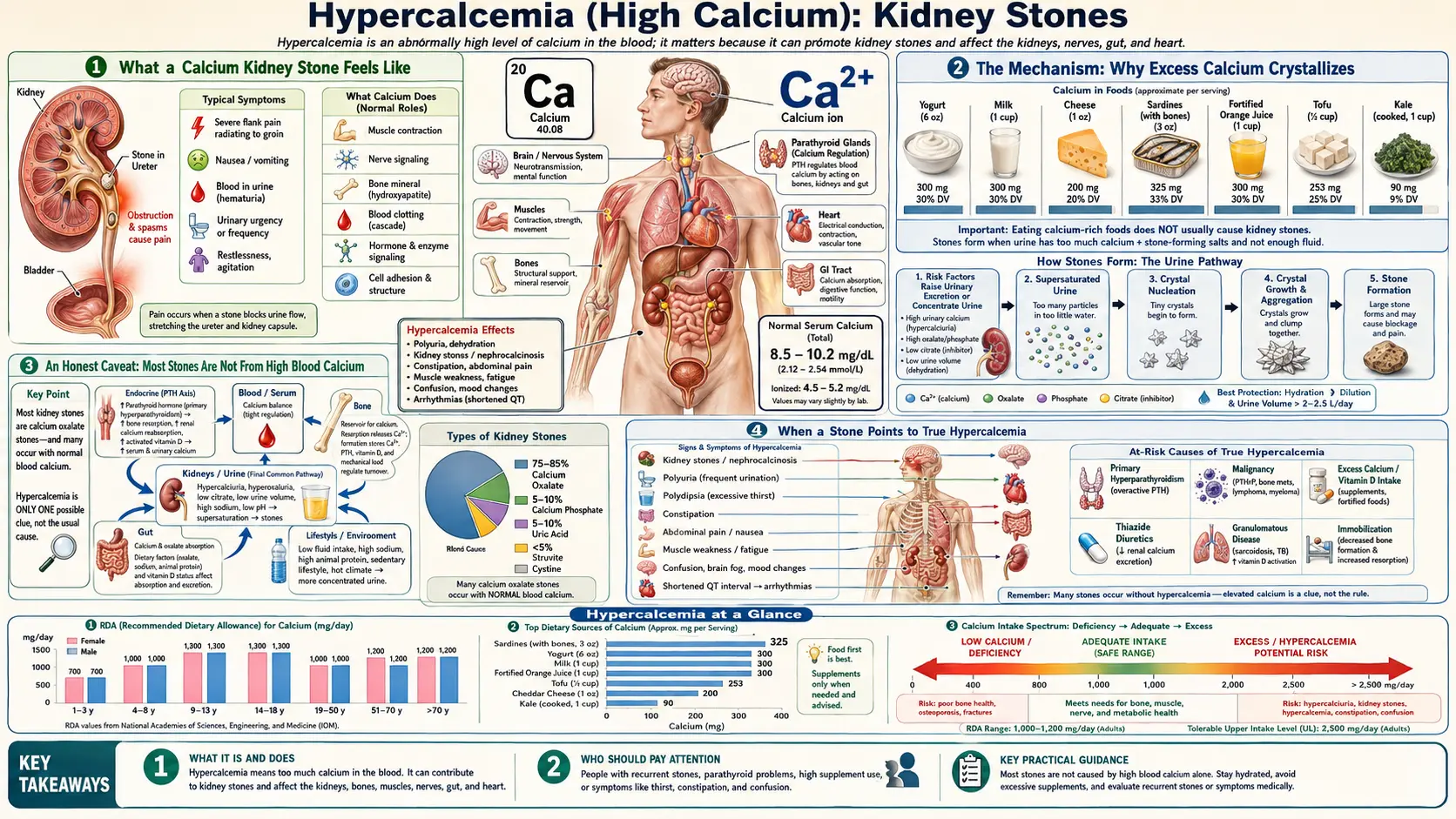
Hypercalcemia (High Calcium): Kidney Stones
Kidney stones are the symptom most people associate with “too much calcium,” and there is real truth in that — most stones are built from calcium. But the connection is more surprising than it looks. Stones rarely come from eating too much calcium; far more often they come from too much calcium spilling into the urine, which can happen even when blood calcium is perfectly normal. And when blood calcium itself is genuinely high — the condition called hypercalcemia — a stone may be the first clue that something, often an overactive parathyroid gland, has been quietly raising calcium for years. This page explains the renal side of high calcium specifically: how a stone announces itself, why excess calcium in the urine crystallizes, why a stone is a clue rather than a diagnosis, and when kidney pain is an emergency.
Table of Contents
- What a Calcium Kidney Stone Feels Like
- The Mechanism: Why Excess Calcium Crystallizes
- An Honest Caveat: Most Stones Are Not From High Blood Calcium
- When a Stone Points to True Hypercalcemia
- Causes: From Hypercalciuria to Hypercalcemia
- Getting Checked
- How Stones and High Calcium Are Managed
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What a Calcium Kidney Stone Feels Like
A small stone sitting quietly in the kidney usually causes nothing at all — many are discovered by accident on a scan done for some other reason. The drama begins when a stone breaks loose and starts to travel down the narrow tube (the ureter) that drains the kidney to the bladder. That journey produces one of the most intense pains in all of medicine, and it has a fairly recognizable shape:
- Pain that comes in waves. The classic stone pain, called renal colic, rises and falls in surges as the ureter squeezes against the obstruction. It is not a steady ache; it crescendos, eases, and crescendos again.
- A flank-to-groin path. It typically starts in the side or back, just below the ribs, and radiates downward and forward toward the lower abdomen, groin, or genitals as the stone moves lower.
- Restlessness. Unlike the pain of an inflamed abdomen — where people lie very still — stone pain often makes people pace, writhe, and shift constantly, unable to find a position that helps.
- Blood in the urine. The stone scrapes the lining of the urinary tract, so urine may look pink, red, or tea-colored, or the blood may be visible only under a microscope (see dark urine).
- Urinary urgency and nausea. A stone near the bladder can cause a constant urge to urinate; the shared nerves between the kidney and the gut mean nausea and vomiting are common companions.
Crucially, this acute event is about the stone physically obstructing the urinary tract — it is a plumbing problem. It is not, by itself, a symptom of high blood calcium. A person can have textbook renal colic with entirely normal blood calcium. That distinction sits at the heart of this page: the stone is the headline, but whether hypercalcemia is the underlying story is a separate question, answered only by a blood test. The non-urinary symptoms of genuinely high blood calcium — the fatigue and confusion, the excess thirst and bone pain, the constipation — are covered on their own sibling pages.
The Mechanism: Why Excess Calcium Crystallizes
To understand stones, it helps to think of urine as a glass of slightly over-sweetened iced tea. You can dissolve a certain amount of sugar; past that point, no more will dissolve and crystals settle out. Urine works the same way with calcium and its partner salts. When urine becomes supersaturated — holding more dissolved calcium and oxalate (or phosphate) than it comfortably can — those minerals begin to crystallize, clump, and grow into a stone. About four out of five kidney stones are calcium stones, most of them calcium oxalate.
The single most important driver of that supersaturation is hypercalciuria — too much calcium in the urine. And here is the point that surprises almost everyone: hypercalciuria is usually not caused by high blood calcium. In the most common form, called idiopathic hypercalciuria, blood calcium is perfectly normal; the kidney simply leaks more calcium into the urine than it should, or the gut absorbs and the bones release a little extra that is then dumped by the kidney. The body keeps the blood level tightly controlled and offloads the surplus into the urine — which is exactly where it can crystallize.
An analogy. Picture the bloodstream as a bank that keeps an exact balance no matter what, and the urine as the overnight drop-box outside. If a little extra cash keeps arriving, the bank's balance stays unchanged — but the drop-box overflows. Hypercalciuria is an overflowing drop-box: the “account” (blood calcium) reads normal, yet a stone forms in the box (the urine) because that is where the surplus piles up.
Several other factors stack on top of high urinary calcium to tip the balance toward a stone:
- Low urine volume. The most powerful and most fixable factor. Concentrated urine (from not drinking enough, or heavy sweating) is supersaturated even at normal calcium levels — like letting the iced tea evaporate down to syrup.
- Dietary oxalate. Oxalate is calcium's crystallizing partner in the most common stones, and high-oxalate diets raise risk in susceptible people (spinach and other greens are notably high; see also oxalates and cooking).
- Low urinary citrate. Citrate is the urine's natural anti-stone agent — it binds calcium and keeps it dissolved. Low citrate removes that protection.
- A counter-intuitive dietary calcium effect. Eating more dietary calcium (from food, at meals) actually lowers stone risk, because calcium in the gut binds oxalate and blocks its absorption. Restricting dietary calcium — the old advice — backfires and raises risk. Calcium supplements taken away from food behave differently and may modestly raise risk. This distinction is one of the most important and most misunderstood facts in stone prevention.
When blood calcium is genuinely elevated — true hypercalcemia — the kidney faces a much larger calcium load to filter, urinary calcium climbs, and the stone risk rises further. So high blood calcium is a real and important cause of stones; it is simply the less common one. The far more frequent path is a normal-blood, high-urine calcium picture.
An Honest Caveat: Most Stones Are Not From High Blood Calcium
It would be misleading to let anyone walk away from this page believing a kidney stone means their blood calcium is high. In the great majority of stone formers, blood calcium is completely normal, and the problem lives entirely in the urine. Treating a stone as proof of hypercalcemia is a mistake in both directions: it can frighten people who are fine, and it can let a real cause go unexamined if the right test is never ordered.
Kidney stones are also extremely common — affecting roughly one in ten people over a lifetime — and they have many causes that have nothing to do with calcium toxicity:
- Dehydration and low urine output — the leading modifiable cause, and the reason hot climates and physically demanding jobs raise stone rates.
- Diet — high salt (which drives calcium into the urine), high animal protein, high oxalate, and low fluid intake.
- Other stone types entirely — uric acid stones (linked to gout, obesity, and acidic urine), struvite stones (from certain urinary infections), and rare cystine stones (an inherited disorder) form by mechanisms unrelated to calcium.
- Genetics and family history — stone-forming tendencies, including idiopathic hypercalciuria, run strongly in families.
- Gut and metabolic conditions — inflammatory bowel disease, bariatric surgery, and chronic diarrhea raise oxalate absorption and lower citrate.
So the honest framing is this: a calcium stone tells you that your urine chemistry favored crystallization. It does not tell you that your blood calcium is high. True hypercalcemia is an uncommon cause of stones — but an important one, because it is treatable and because it points to a specific underlying condition. The next section explains how to tell when a stone is waving that particular flag.
When a Stone Points to True Hypercalcemia
Because true hypercalcemia is the uncommon cause, doctors do not assume it — but they do look for it, because missing it means missing a fixable disease. Certain features make underlying high blood calcium more likely and should prompt a calcium blood test rather than treating the stone in isolation:
- Recurrent stones, especially from a young age. One stone in midlife is most often a urine-chemistry and hydration story. Repeated stones — or stones in someone young — raise the odds of an ongoing metabolic driver such as hypercalcemia.
- Stones on both sides, or many at once. Bilateral or multiple stones suggest a body-wide tendency rather than a one-off.
- The classic non-urinary symptoms alongside the stone. The old medical mnemonic for hypercalcemia is “stones, bones, groans, and psychiatric moans” — kidney stones, bone pain, abdominal groans (constipation, nausea), and psychiatric moans (fatigue, low mood, confusion). When a stone arrives in company with several of these, hypercalcemia climbs the list.
- Excessive thirst and frequent urination. High blood calcium impairs the kidney's ability to concentrate urine, so persistent thirst and high urine volume can accompany the stone.
- Calcium found high on a routine blood test. Often the sequence runs the other way: a stone prompts a blood panel, and the calcium comes back high — uncovering, most commonly, primary hyperparathyroidism that had been silent for years.
The most common cause of true hypercalcemia behind stones is primary hyperparathyroidism, in which a parathyroid gland steadily over-produces parathyroid hormone and pushes calcium up. It is so important in this context that the workup of a recurrent stone former routinely includes a calcium level for exactly this reason — covered next.
The companion pages describe the non-stone symptoms in depth and should not be duplicated here: fatigue and confusion, excess thirst and bone pain, and constipation and digestive effects.
Causes: From Hypercalciuria to Hypercalcemia
It is worth separating the two distinct calcium problems that lead to stones, because they call for different responses.
Causes of high urinary calcium (normal blood calcium) — the common path:
- Idiopathic hypercalciuria. The most frequent metabolic abnormality in stone formers. Blood calcium is normal; the kidney and gut handle calcium in a way that loads the urine. It runs in families.
- High dietary salt. Sodium and calcium are handled together by the kidney, so a salty diet drags more calcium into the urine — one of the most actionable causes.
- High animal protein and low fluids. Both raise the urine's stone-forming tendency, the latter by simple concentration.
- Low dietary calcium, paradoxically. Too little calcium at meals leaves oxalate free to be absorbed and excreted, raising calcium-oxalate risk.
Causes of high blood calcium (true hypercalcemia) — the uncommon but important path:
- Primary hyperparathyroidism. By far the leading cause of hypercalcemia in people who are otherwise well. An overactive parathyroid gland raises both blood and urine calcium, and kidney stones are a classic presentation. See hyperparathyroidism.
- Excess calcium and vitamin D intake. Very high doses of calcium plus vitamin D supplements — or, historically, the “milk-alkali” pattern of huge antacid use — can push blood calcium up. This is the form most directly tied to calcium toxicity from intake.
- Granulomatous diseases. Conditions such as sarcoidosis can cause the body to over-activate vitamin D, raising calcium absorption.
- Cancer. Several cancers raise blood calcium, though this typically presents with marked illness rather than an isolated stone.
Sorting the urinary from the blood problem — and, within the blood problem, identifying hyperparathyroidism — is the whole purpose of the evaluation, because the fix differs completely: drink more and eat smarter for hypercalciuria; treat the parathyroid gland (often with surgery) for hyperparathyroidism.
Getting Checked
Evaluating a kidney stone happens on two timelines: the urgent question of the stone itself, and the slower question of why it formed.
Confirming and locating the stone. When someone arrives with renal colic, imaging confirms the stone and shows its size and position. A low-dose non-contrast CT scan is the most accurate test and the usual choice; ultrasound is often used first in pregnancy and in younger patients to avoid radiation. A urinalysis checks for blood and signs of infection, which changes how urgently the stone must be treated.
Finding the cause — where the calcium question is answered. This is the step that distinguishes a urine problem from a blood problem:
- A blood calcium level. A Comprehensive Metabolic Panel reports serum calcium directly, alongside kidney function. A high calcium is the trigger to pursue hypercalcemia — and if it is high, a parathyroid hormone (PTH) level is checked, because a calcium that is high while PTH is also high (or inappropriately normal) is the signature of primary hyperparathyroidism.
- A 24-hour urine collection. The cornerstone of stone prevention. The patient collects all urine over a full day, and the lab measures calcium, oxalate, citrate, volume, sodium, and uric acid. This reveals hypercalciuria, low citrate, low volume, and other targets — the specific levers to pull — even when blood calcium is normal.
- Stone analysis. If the stone is captured (by straining the urine), sending it to the lab to identify its composition — calcium oxalate, calcium phosphate, uric acid, struvite, or cystine — directly shapes prevention.
The practical upshot: a single stone in an otherwise healthy adult may need only basic blood work and advice, while recurrent stones earn the full metabolic workup, including the 24-hour urine and a careful look at blood calcium for hidden hyperparathyroidism.
How Stones and High Calcium Are Managed
Management runs on three fronts: getting the current stone out, preventing the next one, and — if blood calcium is genuinely high — treating the underlying cause of the hypercalcemia.
Passing or removing the current stone. Small stones (under about 5 mm) usually pass on their own with hydration, pain control, and sometimes a medication (an alpha-blocker such as tamsulosin) that relaxes the ureter to ease passage. Larger or stuck stones, or a stone causing infection or blocked kidney drainage, may need a procedure: shock-wave lithotripsy (sound waves that break the stone from outside), ureteroscopy (a thin scope that retrieves or lasers the stone), or, for large stones, percutaneous removal. The full account of acute stone care lives on the dedicated kidney stones page.
Preventing the next stone — the part patients can most influence. Prevention is built on the urine chemistry, and the evidence here is unusually strong:
- Drink more — the single most effective measure. Aim for enough fluid to produce roughly 2–2.5 liters of urine a day (pale urine is the simple target). Diluting the urine fights supersaturation directly. A landmark trial showed this alone roughly halved recurrence.
- Don't restrict dietary calcium — keep it normal, from food. A diet with normal calcium plus lower salt and lower animal protein outperformed a low-calcium diet for preventing recurrent calcium-oxalate stones. Cutting calcium backfires; cutting salt and excess meat helps.
- Cut sodium. Less salt means less calcium spilled into the urine.
- Moderate oxalate if you are an oxalate-stone former — and pair high-oxalate foods with a calcium-containing food at the same meal so the calcium binds the oxalate in the gut.
- Medications when diet is not enough. A thiazide diuretic reduces urinary calcium; potassium citrate raises protective citrate (and is especially useful for low-citrate or uric-acid stones); for uric-acid stones, allopurinol and urine alkalinization help.
Treating true hypercalcemia, when present. If the cause is primary hyperparathyroidism, the definitive treatment is usually surgical removal of the overactive gland (parathyroidectomy), which can stop the stone cycle at its source. If the cause is excess calcium and vitamin D intake, the fix is simply stopping the excess. Severe hypercalcemia of any cause is treated more urgently with intravenous fluids and other medications — but that is the territory of the markedly high blood calcium described on the fatigue and confusion and thirst and bone pain pages, not of the everyday stone.
When to Seek Care / Red Flags
Most stone pain, though severe, is not immediately dangerous — but a stone plus certain features can signal a blocked, infected kidney, which is a true emergency. Seek urgent or emergency care for:
- Fever or chills with the pain. This is the most important red flag: a blocked kidney that becomes infected (obstructive pyelonephritis) can turn into sepsis quickly and needs emergency drainage. Stone pain with fever is never “wait and see.”
- Severe, uncontrollable pain or relentless vomiting — especially if you cannot keep down fluids, which leads to dehydration that worsens everything.
- Little or no urine, or signs of both kidneys blocked — a medical emergency, particularly in someone with a single kidney.
- Visible blood in the urine for the first time, or pain plus inability to urinate.
- Stone symptoms during pregnancy — these need prompt, specialized evaluation.
Beyond the acute event, get a calcium level checked — not emergently, but don't skip it — if you have recurrent stones, stones at a young age, or a stone accompanied by the “stones, bones, groans, and moans” pattern of persistent fatigue and confusion, bone pain and thirst, or unexplained constipation. Catching silent hyperparathyroidism this way can prevent years of further stones — the whole reason a stone is treated as a clue, not just a plumbing problem.
Key Research Papers
- Worcester EM, Coe FL (2010). Calcium Kidney Stones. New England Journal of Medicine;363(10):954-963. — DOI: 10.1056/NEJMcp1001011
- Coe FL, Evan A, Worcester E (2011). Pathophysiology-Based Treatment of Idiopathic Calcium Kidney Stones. Clinical Journal of the American Society of Nephrology;6(8):2083-2092. — DOI: 10.2215/CJN.11321210
- Borghi L, Schianchi T, Meschi T, et al. (2002). Comparison of Two Diets for the Prevention of Recurrent Stones in Idiopathic Hypercalciuria. New England Journal of Medicine;346(2):77-84. — DOI: 10.1056/NEJMoa010369
- Curhan GC, Willett WC, Rimm EB, Stampfer MJ (1993). A Prospective Study of Dietary Calcium and Other Nutrients and the Risk of Symptomatic Kidney Stones. New England Journal of Medicine;328(12):833-838. — DOI: 10.1056/NEJM199303253281203
- Curhan GC, Willett WC, Speizer FE, Spiegelman D, Stampfer MJ (1997). Comparison of Dietary Calcium with Supplemental Calcium and Other Nutrients as Factors Affecting the Risk for Kidney Stones in Women. Annals of Internal Medicine;126(7):497-504. — DOI: 10.7326/0003-4819-126-7-199704010-00001
- Curhan GC, Willett WC, Knight EL, Stampfer MJ (2004). Dietary Factors and the Risk of Incident Kidney Stones in Younger Women: Nurses' Health Study II. Archives of Internal Medicine;164(8):885-891. — DOI: 10.1001/archinte.164.8.885
- Taylor EN, Curhan GC (2007). Oxalate Intake and the Risk for Nephrolithiasis. Journal of the American Society of Nephrology;18(7):2198-2204. — DOI: 10.1681/ASN.2007020219
- Qaseem A, Dallas P, Forciea MA, et al. (2014). Dietary and Pharmacologic Management to Prevent Recurrent Nephrolithiasis in Adults: A Clinical Practice Guideline From the American College of Physicians. Annals of Internal Medicine;161(9):659-667. — DOI: 10.7326/M13-2908
- Pearle MS, Goldfarb DS, Assimos DG, et al. (2014). Medical Management of Kidney Stones: AUA Guideline. Journal of Urology;192(2):316-324. — DOI: 10.1016/j.juro.2014.05.006
- Minisola S, Pepe J, Piemonte S, Cipriani C (2015). The diagnosis and management of hypercalcaemia. BMJ;350:h2723. — DOI: 10.1136/bmj.h2723
PubMed Topic Searches
- PubMed — Calcium kidney stones and pathophysiology
- PubMed — Idiopathic hypercalciuria and stone formation
- PubMed — Dietary vs supplemental calcium and stone risk
- PubMed — Primary hyperparathyroidism and stones
- PubMed — Stone prevention: fluids, thiazides, citrate
Connections
- Hypercalcemia Symptom Hub
- Hypercalcemia and Constipation & Digestive
- Hypercalcemia and Fatigue & Confusion
- Hypercalcemia and Thirst & Bone Pain
- Calcium Overview
- Calcium and Bone Health
- Calcium Food Sources
- Kidney Stones
- Hyperparathyroidism
- Sarcoidosis
- Kidney Disease
- Dark Urine
- Vitamin D
- Magnesium
- Comprehensive Metabolic Panel