High-Sensitivity C-Reactive Protein (hs-CRP) Test
High-sensitivity C-reactive protein (hs-CRP) is one of the most clinically useful and widely ordered markers of systemic inflammation. Unlike the standard CRP test, which detects high-level acute inflammation, the hs-CRP assay is sensitive enough to detect low-grade chronic inflammation — the type silently driving heart disease, diabetes, cancer, and neurodegenerative conditions long before symptoms appear. It is considered an independent cardiovascular risk predictor and is a cornerstone of preventive cardiovascular assessment.
Table of Contents
- What hs-CRP Measures
- Why It Is Ordered
- How the Test Is Performed
- Reference Ranges and Interpretation
- What Abnormal Results Mean
- Conditions It Helps Detect
- How to Improve Your Numbers
- Limitations and Considerations
- Key Research Papers
- Featured Videos
What hs-CRP Measures
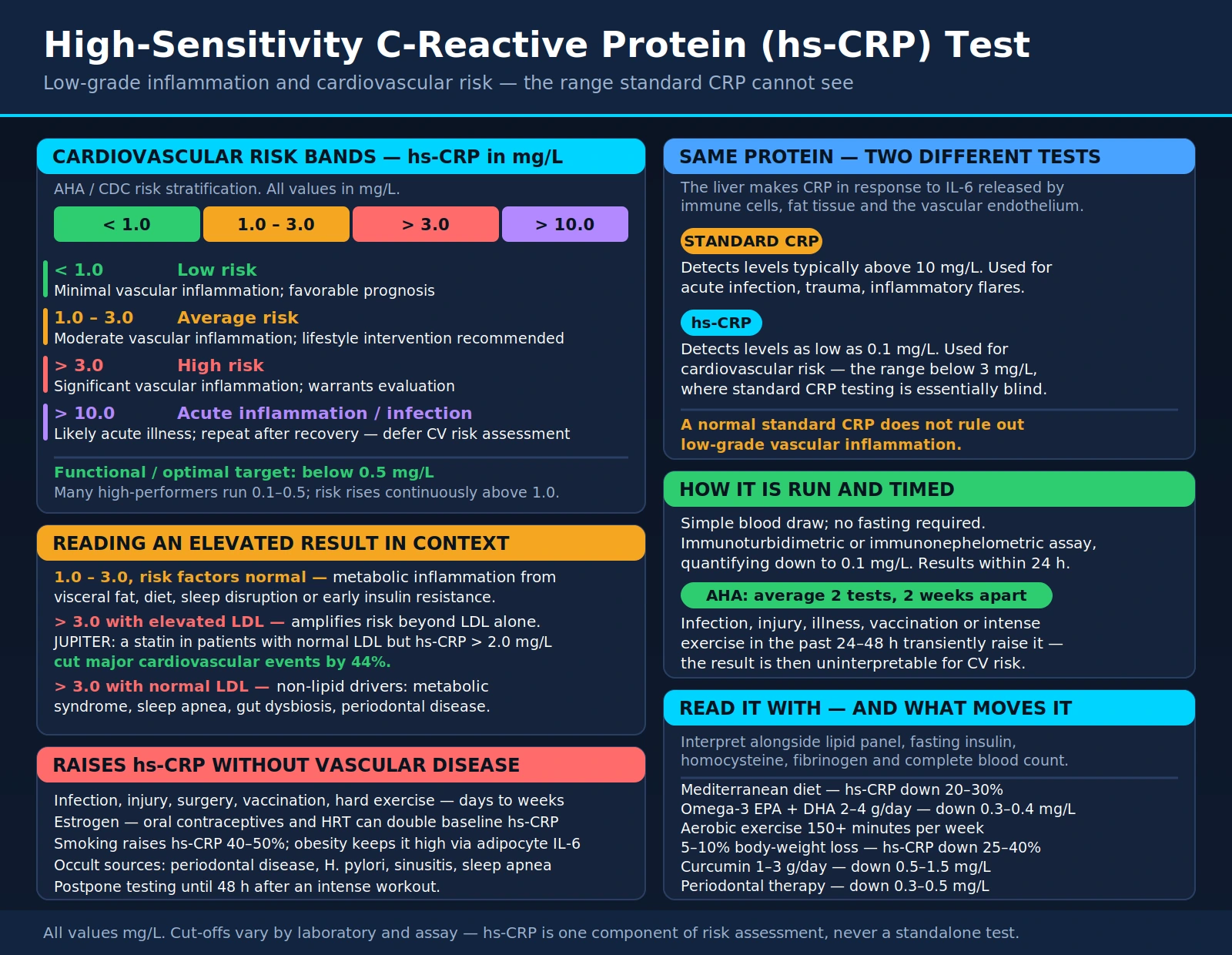
C-reactive protein is an acute-phase reactant produced by the liver in response to interleukin-6 (IL-6), a pro-inflammatory cytokine released by immune cells, fat tissue (adipocytes), and the vascular endothelium. CRP is a pattern recognition molecule of the innate immune system that binds to damaged cells and pathogens, activates complement, and facilitates phagocytosis.
The standard CRP test measures levels typically above 10 mg/L, making it useful for detecting acute infection, trauma, or flares of inflammatory disease. The high-sensitivity version (hs-CRP) uses more refined immunoassay technology to detect levels as low as 0.1 mg/L — extending its clinical utility into the range associated with cardiovascular risk (below 3 mg/L), where conventional CRP testing is essentially blind.
Chronically elevated hs-CRP at levels of 1–3 mg/L reflects ongoing low-grade vascular and systemic inflammation — a state that is not caused by active infection but rather by metabolic dysfunction, visceral adiposity, oxidative stress, poor diet, sedentary lifestyle, sleep disruption, and other modifiable lifestyle factors.
Why It Is Ordered
Clinicians order hs-CRP in the following clinical contexts:
- Cardiovascular risk stratification, particularly in patients with intermediate Framingham risk scores where the result may tip the decision toward or away from statin therapy
- Monitoring of chronic inflammatory conditions including rheumatoid arthritis, lupus, and inflammatory bowel disease (alongside standard CRP)
- Metabolic syndrome and insulin resistance evaluation, where hs-CRP frequently runs elevated alongside fasting insulin, triglycerides, and low HDL
- Assessment of visceral adiposity-related inflammation in overweight and obese patients
- Evaluation of unexplained fatigue, brain fog, or systemic symptoms that may reflect subclinical inflammation
- Monitoring response to anti-inflammatory interventions — dietary changes, exercise programs, weight loss, or pharmacotherapy
- Risk assessment in patients with type 2 diabetes, where elevated hs-CRP independently predicts cardiovascular events beyond HbA1c and lipid levels
- Preventive wellness panels in functional and integrative medicine to detect inflammation before clinical disease manifests
The American Heart Association and the CDC jointly endorse hs-CRP as a clinically useful cardiovascular risk marker and support its use in intermediate-risk patients as an adjunct to traditional risk calculators.
How the Test Is Performed
The hs-CRP test is a simple blood draw performed in a clinical laboratory. No fasting is required, though many practitioners order it alongside fasting lipids and glucose for a comprehensive metabolic panel, making the combined blood draw fasting. The test uses high-sensitivity immunoturbidimetric or immunonephelometric assay methods that can quantify CRP at concentrations as low as 0.1 mg/L.
Results are typically available within 24 hours. Because hs-CRP is an acute-phase reactant, any active infection, injury, illness, intense exercise in the preceding 24–48 hours, or recent vaccination can transiently elevate it — making the result uninterpretable for cardiovascular risk purposes. Under these circumstances, the test should be repeated once the acute condition has fully resolved.
For cardiovascular risk assessment, the American Heart Association recommends averaging two hs-CRP measurements taken two weeks apart for greater precision, as there is modest biological day-to-day variability in the marker.
Reference Ranges and Interpretation
hs-CRP Cardiovascular Risk Stratification (mg/L)
| hs-CRP Level (mg/L) | Cardiovascular Risk Category | Clinical Interpretation |
|---|---|---|
| < 1.0 | Low risk | Minimal vascular inflammation; favorable prognosis |
| 1.0 – 3.0 | Average risk | Moderate vascular inflammation; lifestyle intervention recommended |
| > 3.0 | High risk | Significant vascular inflammation; warrants evaluation and intervention |
| > 10.0 | Acute inflammation / infection | Likely acute illness; repeat after recovery |
The functional/optimal medicine target is hs-CRP below 0.5 mg/L. Many high-performing individuals with excellent diet, sleep, exercise, and low stress maintain levels in the 0.1–0.5 mg/L range. While conventional medicine uses the 3.0 mg/L threshold to define "high risk," research increasingly demonstrates that incremental cardiovascular risk begins at levels above 1.0 mg/L, and the relationship between hs-CRP and cardiovascular events is continuous — not a simple cut-off.
What Abnormal Results Mean
An elevated hs-CRP result does not diagnose a specific disease — it signals that inflammation is present somewhere in the body. The clinical meaning depends heavily on context:
- hs-CRP 1.0–3.0 mg/L with normal standard risk factors: Suggests metabolic inflammation, possibly from visceral fat, dietary pattern, sleep disruption, or early insulin resistance. Lifestyle intervention is the primary response.
- hs-CRP > 3.0 mg/L with elevated LDL: Significantly amplifies cardiovascular risk beyond what LDL alone predicts. The JUPITER trial demonstrated that statin therapy in patients with normal LDL but elevated hs-CRP (>2.0 mg/L) reduced major cardiovascular events by 44%.
- hs-CRP > 3.0 mg/L with normal LDL: Points toward non-lipid drivers of inflammation — metabolic syndrome, sleep apnea, gut dysbiosis, periodontal disease, or occult inflammatory condition. Comprehensive workup is warranted.
- hs-CRP > 10 mg/L: Indicates acute phase response from active infection, injury, autoimmune flare, or inflammatory disease. Cardiovascular risk assessment should be deferred until the acute condition resolves and the marker returns to baseline.
- Persistently elevated hs-CRP despite treatment: May indicate occult infection (periodontal disease, H. pylori, chronic sinusitis), undiagnosed autoimmune disease, sleep apnea, or resistance to lifestyle interventions.
Interpreting hs-CRP alongside other markers — lipid panel, fasting insulin, homocysteine, fibrinogen, and complete blood count — provides a much richer picture of cardiovascular and metabolic risk than any single test.
Conditions It Helps Detect
Elevated hs-CRP is associated with a remarkably broad range of conditions, reflecting inflammation's central role in chronic disease:
- Cardiovascular disease: Atherosclerosis, coronary artery disease, heart attack, stroke, and peripheral arterial disease all correlate with elevated hs-CRP, which independently predicts events even after adjusting for LDL cholesterol and other traditional risk factors.
- Type 2 diabetes: hs-CRP is elevated years before diabetes diagnosis, reflecting the inflammatory nature of beta-cell dysfunction and insulin resistance. It predicts progression from prediabetes to overt diabetes.
- Metabolic syndrome: Visceral adiposity generates large quantities of IL-6, driving CRP production. hs-CRP is a reliable surrogate marker of central obesity-driven inflammation.
- Autoimmune diseases: Rheumatoid arthritis, lupus, ankylosing spondylitis, and inflammatory bowel disease are tracked with CRP/hs-CRP as a disease activity marker and treatment response guide.
- Cancer: Prospective cohort studies link chronically elevated hs-CRP with increased risk of colorectal, lung, breast, and other cancers — consistent with the role of chronic inflammation in tumor microenvironment promotion.
- Depression and cognitive decline: Meta-analyses find hs-CRP elevations in major depression, with neuroinflammation proposed as a mechanistic link. Elevated hs-CRP also predicts cognitive decline in older adults.
- Sleep apnea: Obstructive sleep apnea generates repetitive hypoxic stress that markedly elevates hs-CRP; treating apnea often brings CRP down substantially.
- Periodontal disease: Bacterial biofilms in the gums chronically activate the immune system, elevating hs-CRP. Dental treatment demonstrably reduces systemic hs-CRP.
How to Improve Your Numbers
Because hs-CRP reflects modifiable lifestyle and metabolic factors, it responds robustly to targeted interventions:
- Anti-inflammatory diet: A Mediterranean-pattern diet rich in olive oil, fatty fish, vegetables, legumes, and berries consistently reduces hs-CRP by 20–30%. The PREDIMED trial reported a hazard ratio of 0.69 (95% CI 0.53–0.91) for major cardiovascular events — about a 30% relative reduction — in participants assigned a Mediterranean diet supplemented with extra-virgin olive oil.
- Omega-3 fatty acids: Supplemental EPA and DHA at 2–4 g/day have been shown in multiple meta-analyses to reduce hs-CRP by an average of 0.3–0.4 mg/L. The REDUCE-IT trial demonstrated profound cardiovascular benefit from high-dose EPA (icosapentaenoic acid).
- Exercise: Regular moderate-intensity aerobic exercise — 150+ minutes per week — consistently reduces hs-CRP. High-intensity interval training (HIIT) may produce faster reductions. Acute strenuous exercise transiently elevates CRP, so testing should be postponed 48 hours after intense workouts.
- Weight loss: Visceral fat is the most powerful driver of chronic CRP elevation. Each kilogram of fat loss produces measurable CRP reduction. A 5–10% reduction in body weight can lower hs-CRP by 25–40%.
- Curcumin: Bioavailable curcumin formulations (phospholipid complex, piperine-enhanced, or nanoparticle preparations) show consistent hs-CRP reductions in clinical trials, typically 0.5–1.5 mg/L with doses of 1–3 g/day.
- Sleep optimization: Both short sleep (<6 hours) and poor-quality sleep strongly elevate hs-CRP. Treating sleep apnea, improving sleep hygiene, and achieving 7–9 hours of quality sleep reduces inflammatory markers significantly.
- Smoking cessation: Smoking elevates hs-CRP by 40–50%. Cessation reduces CRP toward non-smoker levels within months, though the process is gradual.
- Statin therapy: Statins have potent anti-inflammatory properties independent of their LDL-lowering effects. Rosuvastatin 20 mg reduced hs-CRP by 37% in the JUPITER trial, driving much of its cardiovascular benefit in the study population with elevated hs-CRP and normal LDL.
- Gum disease treatment: Periodontal therapy (scaling and root planing) reduces systemic hs-CRP by 0.3–0.5 mg/L on average — a clinically meaningful reduction often overlooked by non-dental practitioners.
Limitations and Considerations
Understanding what hs-CRP cannot tell you is as important as knowing what it can:
- Non-specific marker: An elevated hs-CRP does not identify the source or type of inflammation. It must always be interpreted in the full clinical context alongside symptoms, history, and complementary laboratory data.
- Acute-phase confounders: Any recent infection, injury, surgery, vaccination, or intense exercise can falsely elevate hs-CRP for days to weeks. Timing of the test matters enormously.
- Sex and hormonal effects: Oral contraceptives and hormone replacement therapy containing estrogen significantly elevate hs-CRP — sometimes doubling baseline levels — independent of underlying inflammation or cardiovascular risk.
- Obesity artifact: In morbidly obese individuals, hs-CRP may be chronically elevated purely due to adipocyte-derived IL-6, making cardiovascular risk stratification less precise.
- Not a standalone test: Guidelines recommend using hs-CRP as one component of a composite risk assessment rather than as a single decision-making tool. It adds most value in intermediate-risk patients where traditional risk calculators leave clinical uncertainty.
- Standard vs. high-sensitivity CRP: The two assays measure the same protein but at different concentration ranges. For cardiovascular risk assessment, only the hs-CRP assay is appropriate — a normal standard CRP result does not rule out low-grade vascular inflammation.
Key Research Papers
The following curated PubMed literature searches cover the major evidence base for hs-CRP as a clinical marker. Each link opens a live filtered PubMed query.
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Estruch R, Ros E, Salas-Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts (PREDIMED). N Engl J Med. 2018;378(25):e34. PMID: 29897866
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- hs-CRP and sleep apnea — PubMed literature search
- hs-CRP and cancer risk — PubMed literature search
External Authoritative Resources
- MedlinePlus — C-Reactive Protein (CRP) Test
- Lab Tests Online — CRP (AACC)
- StatPearls — C-Reactive Protein (NCBI Bookshelf)
Connections
- All Lab Tests
- Inflammatory Markers
- Lipid Panel
- Homocysteine
- Apolipoprotein B (ApoB)
- Lipoprotein(a)
- Fasting Insulin
- Hemoglobin A1C
- Omega-3 Index
- Cardiovascular Disease
- Atherosclerosis
- Coronary Artery Disease
- Type 2 Diabetes
- Turmeric
- Curcumin
- Vitamin D3
- Magnesium
- Salmon