Omega-3 Index Blood Test
The Omega-3 Index measures the percentage of EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) in red blood cell membranes — reflecting your body's true tissue omega-3 status over the past 8–12 weeks. Unlike simply measuring omega-3 levels in serum (which reflects recent intake), the red blood cell membrane test is a stable, validated biomarker of long-term omega-3 nutrition that directly predicts cardiovascular, neurological, and inflammatory disease risk. It is considered the most clinically meaningful way to assess omega-3 adequacy.
Table of Contents
- What the Omega-3 Index Measures
- Why It Is Ordered
- How the Test Is Performed
- Reference Ranges and Interpretation
- What Abnormal Results Mean
- Conditions It Helps Detect
- How to Improve Your Numbers
- Limitations and Considerations
- Key Research Papers
- Featured Videos
What the Omega-3 Index Measures
The Omega-3 Index specifically quantifies EPA and DHA as a percentage of total fatty acids in red blood cell (erythrocyte) membranes. Because red blood cells turn over every 90–120 days, this measurement reflects the average omega-3 status over the past three months — analogous to how HbA1c reflects average blood sugar over the same period. This long-term integration makes it far more reliable than a single dietary assessment or serum level measurement.
EPA and DHA are long-chain polyunsaturated omega-3 fatty acids derived primarily from marine sources (fatty fish and algae). They are fundamental structural and signaling components of cell membranes throughout the body — especially in cardiomyocytes (heart muscle cells), neurons, and immune cells. Their incorporation into membranes alters membrane fluidity, modulates ion channel function, influences inflammatory signaling cascades, and regulates gene expression through PPAR-alpha and other nuclear receptors.
The Omega-3 Index was developed and validated by researchers William Harris and Clemens von Schacky, who showed it to be a strong, independent predictor of fatal heart attack risk. It is distinct from ALA (alpha-linolenic acid), the short-chain omega-3 found in flaxseed and walnuts; the body converts ALA to EPA and DHA inefficiently (less than 5–10% conversion rate in most adults), meaning plant-only omega-3 intake rarely achieves a therapeutic index.
Why It Is Ordered
Clinicians and integrative practitioners order the Omega-3 Index in the following circumstances:
- Cardiovascular risk assessment beyond traditional lipid panel markers, particularly in patients with borderline lipid values or family history of heart disease
- Evaluation of anti-inflammatory status and guidance on dietary or supplementation strategy for patients with chronic inflammatory conditions
- Depression, anxiety, or cognitive decline evaluation, where low omega-3 status is a modifiable contributing factor
- Monitoring response to omega-3 supplementation or fatty fish dietary changes
- Arrhythmia risk assessment, as EPA+DHA levels in cardiomyocytes are directly linked to electrical stability and sudden cardiac death risk
- Pregnancy and neonatal health planning, since DHA is critical for fetal brain and retinal development
- Dry eye disease and inflammatory eye conditions associated with systemic omega-3 insufficiency
- Pediatric neurodevelopmental assessment in children with ADHD or learning differences, where omega-3 status is modifiable
How the Test Is Performed
The Omega-3 Index is measured from a small blood sample — typically a standard venous blood draw or a finger-prick dried blood spot (DBS) card sent to a specialized laboratory. No fasting is required. The laboratory separates red blood cells from the plasma, extracts total fatty acids from the cell membranes, and uses gas chromatography (GC) or GC-mass spectrometry to quantify each fatty acid as a percentage of total membrane fatty acids. EPA and DHA percentages are added together to give the final Omega-3 Index value.
The dried blood spot method makes this test accessible via at-home testing kits (a simple finger lancet + card mailed to the lab), with accuracy comparable to venous blood testing. Results are typically reported within 1–2 weeks. Because the measurement reflects 3 months of intake, testing more frequently than quarterly provides minimal additional information during supplementation trials — test at baseline, then retest after 3 months to assess response.
The OmegaQuant Analytics laboratory (founded by Dr. William Harris) is the most widely validated reference laboratory for this test and offers both consumer and clinical testing options.
Reference Ranges and Interpretation
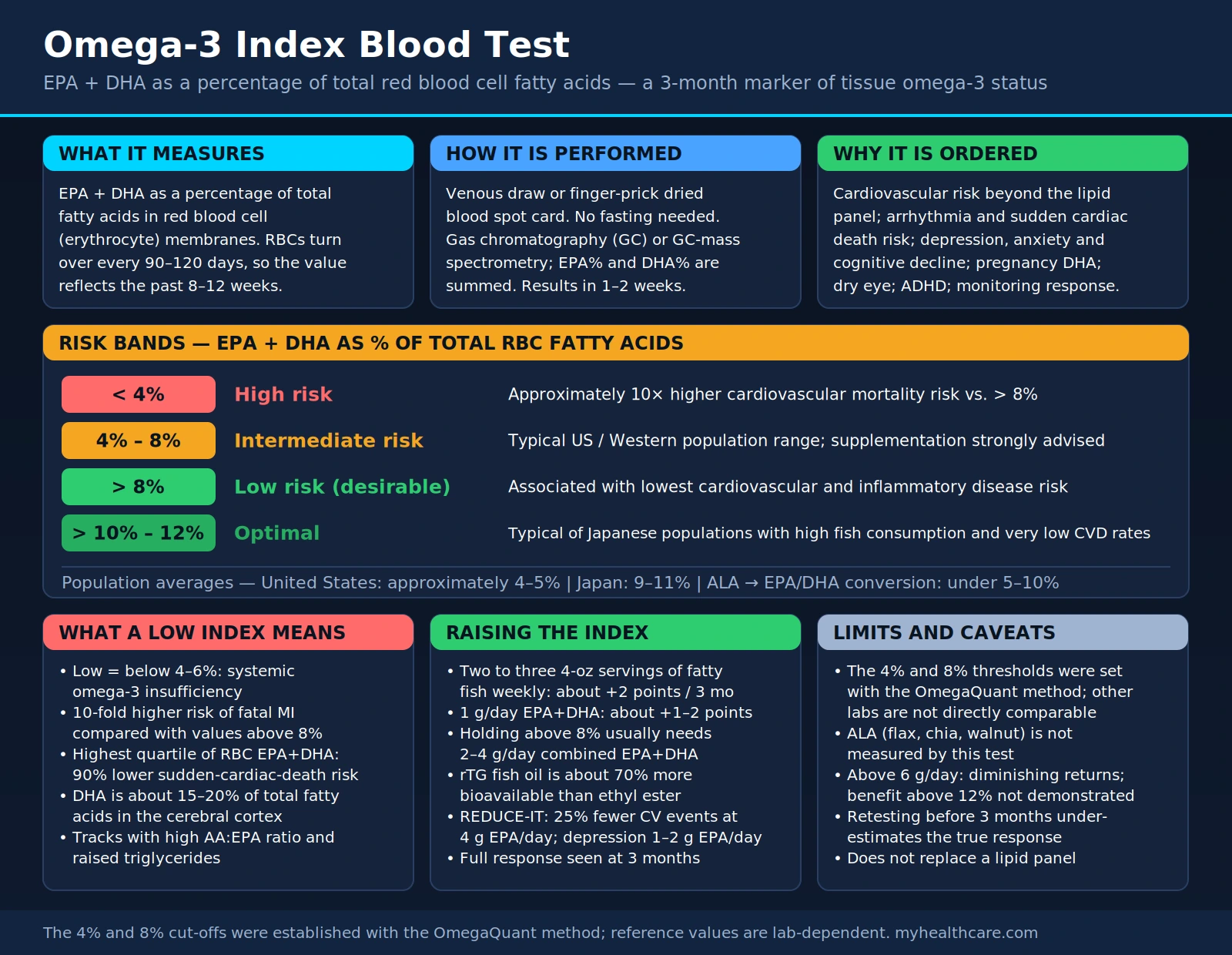
Omega-3 Index Risk Categories (EPA + DHA as % of total RBC fatty acids)
| Omega-3 Index (%) | Risk Category | Clinical Context |
|---|---|---|
| < 4% | High risk | Approximately 10× higher cardiovascular mortality risk vs. >8% |
| 4% – 8% | Intermediate risk | Typical US/Western population range; supplementation strongly advised |
| > 8% | Low risk (desirable) | Associated with lowest cardiovascular and inflammatory disease risk |
| > 10% – 12% | Optimal | Levels typical of Japanese populations with high fish consumption and very low CVD rates |
The average American has an Omega-3 Index of approximately 4–5%, placing the majority of the US population in the intermediate-to-high cardiovascular risk zone. By contrast, people in Japan — where oily fish consumption is culturally central — average 9–11%, correlating with markedly lower rates of sudden cardiac death and cardiovascular disease despite similar traditional risk factor profiles.
What Abnormal Results Mean
A low Omega-3 Index (below 4–6%) indicates systemic omega-3 insufficiency with several downstream implications:
- Cardiovascular vulnerability: Cardiomyocytes with low EPA+DHA in their membranes are more electrically unstable, predisposing to ventricular arrhythmias and sudden cardiac death. Low index values are associated with a 10-fold higher risk of fatal MI compared to values above 8%.
- Pro-inflammatory bias: With insufficient EPA and DHA as substrates, the body preferentially produces pro-inflammatory eicosanoids from arachidonic acid (AA). The AA-to-EPA ratio in cell membranes is a direct measure of the inflammatory-versus-anti-inflammatory balance, and a low Omega-3 Index usually accompanies a high AA:EPA ratio.
- Neurological impact: DHA constitutes approximately 15–20% of total fatty acids in the cerebral cortex. Chronic deficiency impairs synaptic plasticity, neurotransmitter signaling, and neuroprotective mechanisms — contributing to depression, anxiety, cognitive aging, and neurodegenerative risk.
- Triglyceride elevation: Low EPA+DHA status correlates with higher triglyceride levels, as EPA and DHA suppress hepatic triglyceride synthesis through PPAR-alpha activation and SREBP-1c inhibition.
- Platelet aggregation: Omega-3 deficiency shifts the balance toward more pro-aggregatory thromboxane A2 production relative to anti-aggregatory prostacyclin and thromboxane A3 from EPA, increasing clot risk.
Conditions It Helps Detect
The Omega-3 Index connects to a broad range of conditions, reflecting the central importance of these fatty acids in human physiology:
- Sudden cardiac death and arrhythmia: The original validation study for the Omega-3 Index showed that patients in the highest quartile of RBC EPA+DHA had a 90% lower risk of sudden cardiac death compared to those in the lowest quartile.
- Hypertriglyceridemia: Prescription-strength omega-3 therapy (Vascepa/icosapentaenoic acid; Lovaza/EPA+DHA) is FDA-approved for severe hypertriglyceridemia and demonstrated 25% cardiovascular event reduction in the REDUCE-IT trial at 4 g EPA/day.
- Major depression: Meta-analyses of randomized trials find EPA-dominant formulas reduce depression scores comparably to antidepressants in some populations, with strongest evidence for EPA doses of 1–2 g/day.
- Cognitive decline and dementia: Low DHA is associated with accelerated brain aging, smaller hippocampal volumes, and higher Alzheimer's risk in observational studies. DHA is required for synthesis of neuroprotectin D1, a potent endogenous anti-inflammatory and neuroprotective mediator.
- Preterm birth and fetal development: Low maternal Omega-3 Index during pregnancy is associated with higher preterm birth risk. DHA supplementation in the third trimester reduces preterm birth rates and supports neonatal brain and retinal development.
- Dry eye disease: Corneal goblet cells depend on membrane omega-3 content for normal mucin production and tear film stability. Omega-3 Index inversely correlates with dry eye symptom severity.
- ADHD in children: Multiple meta-analyses find EPA+DHA supplementation produces modest but consistent improvements in ADHD symptom scores, particularly inattention, in children with low baseline Omega-3 Index.
How to Improve Your Numbers
The Omega-3 Index responds predictably and reliably to dietary and supplementation changes, with full response seen after 3 months:
- Fatty fish consumption: Wild-caught salmon, sardines, mackerel, herring, and anchovies are the most potent dietary sources. Two to three 4-oz servings per week of fatty fish raises the Omega-3 Index by approximately 2 percentage points over three months. Farm-raised salmon varies considerably depending on feed composition — wild-caught is more reliably high in EPA+DHA.
- EPA+DHA supplements: Standard fish oil, krill oil, algal oil (vegan DHA source), or prescription omega-3s all raise the index when dosed appropriately. A 1 g/day combined EPA+DHA supplement raises the index by approximately 1–2 percentage points; achieving and maintaining an index above 8% typically requires 2–4 g/day of combined EPA+DHA for most individuals in the intermediate range.
- Choosing the right form: Re-esterified triglyceride (rTG) forms of fish oil show approximately 70% higher bioavailability than ethyl ester forms. Krill oil phospholipid form has good bioavailability even at lower doses. Algal oil provides DHA (and some EPA in newer formulations) and is the only vegan option with meaningful bioavailability.
- Reduce omega-6 competition: Reducing dietary omega-6 linoleic acid (from corn, soybean, sunflower, and safflower oils) decreases competition with EPA+DHA for incorporation into membranes and for the same desaturase enzymes. Switching to olive oil for cooking while supplementing omega-3s accelerates index improvement.
- High EPA for triglycerides: Pure EPA supplements (icosapentaenoic acid / Vascepa) are more potent triglyceride-lowering agents than mixed EPA+DHA, though DHA is more important for brain health. For combined cardiovascular and neurological benefit, a balanced EPA+DHA formula is preferred for general supplementation.
- Re-test at 3 months: Given the 90-day red blood cell lifespan, retesting before 3 months underestimates the true response. Testing at 3 months after a consistent dietary or supplementation change gives an accurate picture of the new steady-state index.
Limitations and Considerations
- Lab-specific variation: Not all labs measure the Omega-3 Index using the validated OmegaQuant method. Results from different laboratories may not be directly comparable; the risk thresholds described here (4%, 8%) were established using the OmegaQuant methodology.
- ALA does not contribute meaningfully: Alpha-linolenic acid (ALA) from flaxseed, chia, and walnuts is not measured in the standard Omega-3 Index, which specifically captures EPA+DHA in red blood cell membranes. ALA supplementation alone rarely achieves a meaningful index increase.
- Dose-response plateau: Very high doses of EPA+DHA (>6 g/day) produce diminishing returns on index improvement. Benefits from exceeding 12% have not been demonstrated and very high doses may increase LDL slightly and theoretically increase bleeding time, though clinically significant bleeding at typical supplementation doses (<4 g/day) is not well-supported by evidence.
- Contaminants in fish oil: Low-quality fish oil supplements may contain oxidized lipids (rancid oil), heavy metals, or PCBs. Third-party testing certifications (IFOS, NSF, USP) indicate product quality. Rancid fish oil may actually promote oxidative stress rather than reduce it.
- Not a standalone cardiovascular test: The Omega-3 Index provides important and independent information but does not replace lipid panels, blood pressure monitoring, HbA1c, or other standard cardiovascular risk assessments. It is best viewed as an additive tool in a comprehensive evaluation.
Key Research Papers
The following curated PubMed citations and literature searches cover the major evidence base for the Omega-3 Index. Each linked PMID opens the specific paper on PubMed.
- Harris WS, Von Schacky C (2004) — The Omega-3 Index: a new risk factor for death from coronary heart disease? Preventive Medicine. PMID: 15208124
- Search PubMed
- Search PubMed
- Search PubMed
- Sublette ME et al. (2011) — Meta-analysis of EPA for major depression. Journal of Clinical Psychiatry. PMID: 20439549
- Search PubMed
- Kar S et al. (2017) — Omega-3 Index and preterm birth: prospective cohort evidence. Nutrients. PMID: 28900017
- Search PubMed
- Dyall SC (2015) — Long-chain omega-3 fatty acids and the brain: a review of the independent and shared effects of EPA, DPA and DHA. Frontiers in Aging Neuroscience. PMID: 26829184
- Search PubMed
- Omega-3 Index and cognitive decline — PubMed literature search
- Omega-3 and dry eye disease — PubMed literature search
External Authoritative Resources
- OmegaQuant — Omega-3 Index reference (Dr. William Harris)
- Lab Tests Online — Omega-3 Fatty Acids (AACC)
- StatPearls — Omega-3 Fatty Acids (NCBI Bookshelf)
Connections
- All Lab Tests
- Omega-3 and Fish Oil for Rheumatoid Arthritis — using the index to check whether a dose is actually landing
- Lipid Panel
- Inflammatory Markers
- hs-CRP Test
- Apolipoprotein B (ApoB)
- Lipoprotein(a)
- Homocysteine
- Salmon
- Sardines
- Cardiovascular Disease
- Atherosclerosis
- Alzheimer's Disease
- Depression
- Vitamin D3
- Magnesium
- Turmeric