Uric Acid Test: Gout, Kidney Health, and Cardiovascular Risk

The serum uric acid test measures the concentration of uric acid in the blood, providing critical information about purine metabolism, kidney function, and risk for several chronic diseases. Long associated primarily with gout, uric acid is now recognized as a biomarker with broad implications for kidney stone formation, cardiovascular health, metabolic syndrome, and overall longevity. Both elevated and depressed uric acid levels carry clinical significance.
Table of Contents
- Overview
- When Ordered
- Reference Ranges
- Gout and Hyperuricemia
- Kidney Stone Risk
- Cardiovascular Connection
- Causes of High and Low Uric Acid
- Dietary Purine Sources
- Treatment Approaches
- References
- Featured Videos
Overview
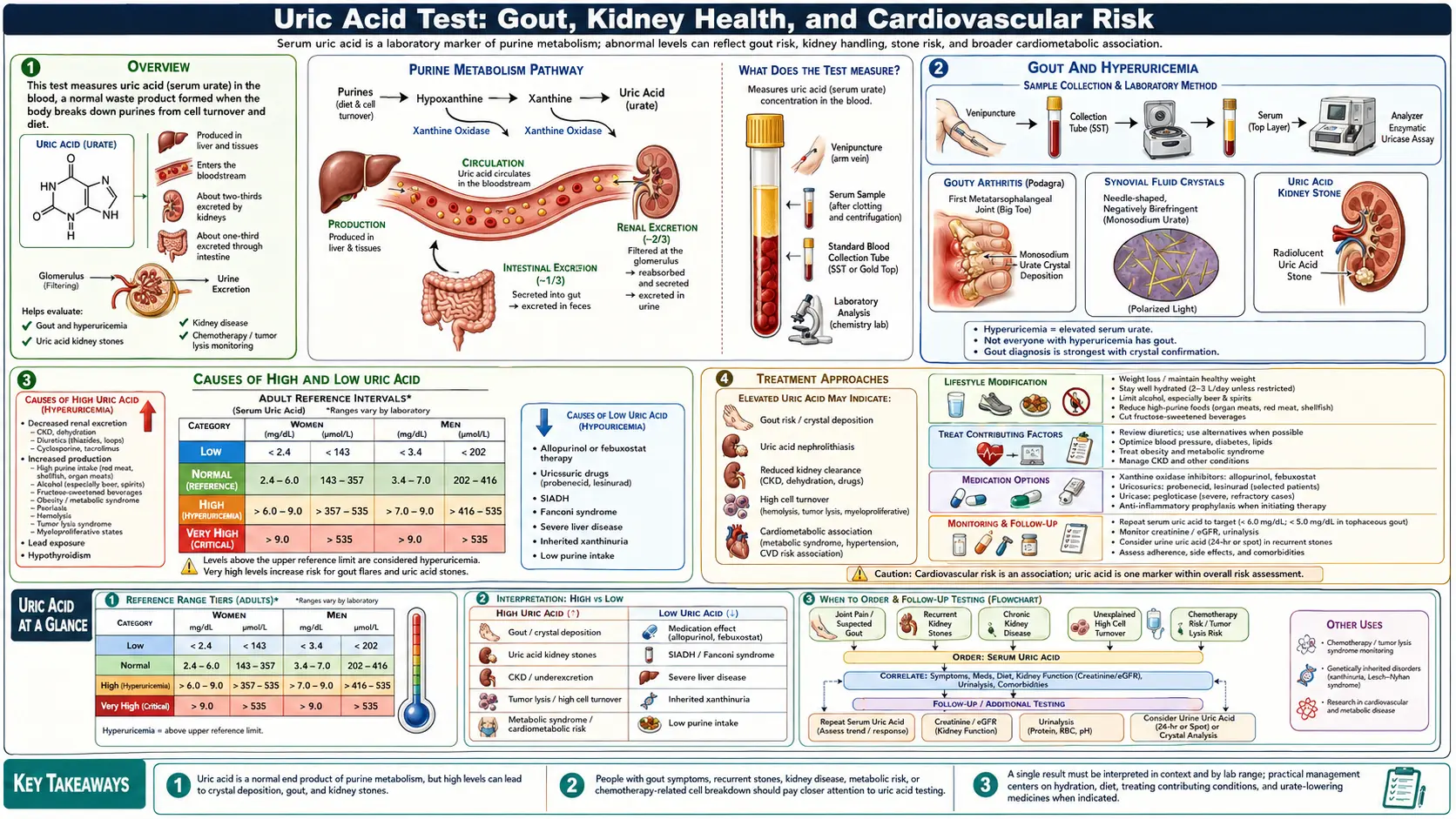
Uric acid is the final breakdown product of purines — nitrogen-containing compounds found in DNA, RNA, and ATP. When cells die or when purine-rich foods are metabolized, the purines adenine and guanine are broken down sequentially through hypoxanthine and xanthine into uric acid, a reaction catalyzed by the enzyme xanthine oxidase. Unlike most mammals, humans lack uricase — the enzyme that converts uric acid into the more soluble allantoin — which means uric acid accumulates to a relatively high degree in human blood.
Approximately two-thirds of uric acid is excreted by the kidneys; the remaining one-third passes through the gastrointestinal tract. When production exceeds excretion — or when renal clearance is impaired — serum uric acid rises, a condition called hyperuricemia. Hyperuricemia is defined as serum uric acid above 6.8 mg/dL, the saturation point at which monosodium urate crystals begin to form in tissues.
Uric acid serves as one of the body's most potent antioxidants in plasma, which may explain why evolution preserved elevated uric acid levels despite their pathological consequences. In intracellular compartments, however, uric acid paradoxically promotes oxidative stress and inflammation.
When Ordered
A serum uric acid test is ordered in the following clinical situations:
- Suspected gout: Acute joint pain, redness, and swelling — particularly in the first metatarsophalangeal joint (big toe), ankle, or knee
- Monitoring gout treatment: To assess response to urate-lowering therapy and ensure levels are maintained below the saturation threshold
- Kidney stone evaluation: Uric acid stones account for 5–10% of all kidney stones and are associated with chronically acidic urine and hyperuricosuria
- Metabolic syndrome screening: Uric acid is elevated in insulin resistance and may be ordered as part of a comprehensive metabolic workup
- Cardiovascular risk assessment: Emerging evidence supports uric acid as an independent cardiovascular risk factor
- Before and during cancer chemotherapy: Tumor lysis syndrome causes massive cell death and purine release, dramatically raising uric acid
- Kidney disease monitoring: Impaired renal function reduces uric acid clearance; conversely, high uric acid damages renal tubules
- Hypertension investigation: Hyperuricemia is associated with essential hypertension, particularly in adolescents and young adults
Reference Ranges
Serum Uric Acid — Male (mg/dL)
Serum Uric Acid — Female (mg/dL)
Women have lower uric acid levels than men because estrogen promotes renal uric acid excretion. After menopause, women's uric acid levels rise substantially and approach male levels, which correlates with the increased incidence of gout in postmenopausal women. The critical threshold for urate crystal formation is 6.8 mg/dL for both sexes — the saturation concentration of monosodium urate in plasma at 37°C.
For individuals with gout, the therapeutic target during urate-lowering therapy is typically below 6.0 mg/dL, and below 5.0 mg/dL for those with tophi or frequent attacks.
Gout and Hyperuricemia
Gout is the most common form of inflammatory arthritis and results from the deposition of monosodium urate (MSU) crystals in joint spaces and surrounding tissues. When serum uric acid exceeds the saturation threshold (6.8 mg/dL), urate begins to crystallize, particularly in cooler peripheral joints and avascular structures like cartilage and tendons.
Acute gout attacks occur when deposited crystals are shed into the joint fluid, triggering an intense inflammatory cascade mediated by the NLRP3 inflammasome, interleukin-1β, and neutrophil activation. The result is severe pain, swelling, erythema, and warmth that typically peaks within 12–24 hours and resolves over 7–14 days without treatment.
The natural history of gout progresses through distinct stages:
- Asymptomatic hyperuricemia: Elevated uric acid without symptoms; most individuals never progress to clinical gout
- Acute intermittent gout: Episodic flares separated by asymptomatic intercritical periods; flares become more frequent over time if untreated
- Chronic tophaceous gout: Persistent crystalline deposits (tophi) in soft tissues, tendons, and joints; can cause chronic arthritis and joint destruction
Classic gout locations include the first metatarsophalangeal joint (podagra), mid-foot, ankle, knee, wrist, and elbow. Tophi most commonly appear at the Achilles tendon, helix of the ear, fingers, and over bursae.
Importantly, serum uric acid may actually fall during an acute gout attack due to acute-phase protein responses and renal urate excretion, potentially giving a falsely reassuring result. Testing is best done several weeks after an acute episode resolves.
Kidney Stone Risk
Uric acid kidney stones form under specific conditions: hyperuricosuria (excessive urinary uric acid excretion), persistently acidic urine (pH below 5.5), and reduced urine volume. Unlike calcium oxalate stones — which are radiopaque — uric acid stones are radiolucent and may not be visible on plain X-ray, requiring CT scan or ultrasound for detection.
Uric acid stones account for approximately 5–10% of all kidney stones in the general population, rising to 40–50% in patients with type 2 diabetes and metabolic syndrome. The strong association with diabetes and obesity stems from insulin resistance impairing ammonium excretion in the renal tubule, which acidifies the urine and promotes uric acid precipitation.
Risk factors for uric acid nephrolithiasis include:
- Hyperuricemia and hyperuricosuria
- Persistently low urine pH (below 5.5)
- Type 2 diabetes and metabolic syndrome
- Chronic diarrhea (causes volume depletion and acidic urine)
- High purine diet
- Prior uric acid stone episodes
Treatment of uric acid stones focuses on alkalinizing the urine (target pH 6.0–6.5) with potassium citrate, increasing fluid intake, and reducing uric acid levels with allopurinol when hyperuricemia is present. Uric acid stones are unique among kidney stone types in that they can be dissolved medically without surgery when properly treated with alkalinization.
Cardiovascular Connection
Growing evidence implicates hyperuricemia as an independent risk factor for cardiovascular disease, hypertension, and cardiac mortality. Multiple large epidemiological studies have found that elevated uric acid predicts incident hypertension, coronary artery disease, heart failure, stroke, and atrial fibrillation — even after adjusting for traditional risk factors.
Several mechanisms link uric acid to cardiovascular pathology:
- Endothelial dysfunction: Uric acid impairs nitric oxide bioavailability by scavenging NO and downregulating endothelial nitric oxide synthase (eNOS), reducing vasodilation and promoting arterial stiffness
- Oxidative stress: Intracellular uric acid activates NADPH oxidase and promotes reactive oxygen species generation in vascular smooth muscle cells
- Inflammation: Soluble uric acid activates the NLRP3 inflammasome and promotes IL-1β, IL-6, and TNF-α production in macrophages and endothelial cells
- Renin-angiotensin system activation: Uric acid stimulates renin production and angiotensin II activity in the renal afferent arteriole, contributing to hypertension
- Platelet aggregation: Uric acid may enhance platelet aggregability, increasing thrombotic risk
Whether uric acid is causally related to cardiovascular disease or merely a marker of underlying metabolic dysfunction remains debated. Several Mendelian randomization studies have yielded mixed results. However, the consistent epidemiological associations and plausible biological mechanisms support at minimum treating hyperuricemia in high-risk cardiovascular patients.
Causes of High and Low Uric Acid
Causes of Hyperuricemia (High Uric Acid)
- Dietary: High purine intake (organ meats, shellfish, red meat), high fructose consumption (particularly from soft drinks and fruit juice), alcohol (especially beer)
- Reduced renal excretion: Chronic kidney disease, diuretic use (thiazides and loop diuretics), cyclosporine, low-dose aspirin, dehydration
- Overproduction: Myeloproliferative disorders, lymphoma, leukemia, psoriasis, hemolytic anemia, tumor lysis syndrome
- Metabolic: Insulin resistance, obesity, metabolic syndrome, hypothyroidism, hypoparathyroidism
- Genetic: Lesch-Nyhan syndrome (HPRT deficiency), Kelley-Seegmiller syndrome
Causes of Hypouricemia (Low Uric Acid)
- Fanconi syndrome (renal tubular urate wasting)
- Wilson's disease
- SIADH (syndrome of inappropriate ADH secretion)
- Uricosuric drugs (probenecid, losartan, fenofibrate)
- Xanthine oxidase deficiency (xanthinuria)
- Severe liver disease
- Very low purine diet
Low uric acid (below 2.0 mg/dL) has been associated in epidemiological studies with increased risk of multiple sclerosis, Parkinson's disease, and Alzheimer's disease, possibly because uric acid's antioxidant function in plasma protects neurons. However, this association does not establish causality, and uric acid-raising interventions are not currently recommended for neuroprotection.
Dietary Purine Sources
Dietary purines contribute approximately one-third of the body's total uric acid burden, with endogenous cell turnover accounting for the remainder. Purine content varies widely among food groups:
Very High Purine Foods (avoid in gout)
- Organ meats: liver, kidney, brain, sweetbreads (150–1000 mg purines per 100g)
- Anchovies, sardines, mackerel, herring (120–400 mg/100g)
- Meat extracts, gravies, bouillon
- Yeast extracts (Marmite, Vegemite)
High Purine Foods (limit in gout)
- Red meat, pork, lamb, venison
- Shellfish: shrimp, lobster, crab, mussels
- Beer (contains guanosine from yeast)
- Asparagus, spinach, cauliflower (moderate purines but less clinically significant)
Fructose — A Special Case
Fructose does not contain purines but is uniquely pro-uricemic through a different mechanism: fructose metabolism in the liver rapidly depletes ATP, generating AMP which is catabolized to uric acid. High fructose corn syrup in soft drinks and fruit juices is strongly associated with hyperuricemia and gout independent of purine intake. Studies show that men who drink two or more sugar-sweetened beverages daily have an 85% higher risk of gout compared to those who rarely drink them.
Protective Dietary Factors
- Dairy (especially low-fat): Reduces uric acid levels through uricosuric and anti-inflammatory effects
- Coffee: Regular coffee consumption is inversely associated with gout risk, possibly through antioxidant effects or effects on uric acid reabsorption
- Vitamin C: Increases renal uric acid excretion; 500 mg/day associated with modest uric acid reduction
- Cherries and tart cherry juice: Associated with reduced gout flare frequency in observational studies
- Adequate hydration: High urine output dilutes urinary urate and lowers stone risk
Treatment Approaches
Acute Gout Treatment
Acute flares are treated with anti-inflammatory agents rather than urate-lowering drugs (starting urate-lowering therapy during an acute attack can paradoxically prolong the flare):
- Colchicine: Most effective when started within 12–24 hours of flare onset; inhibits NLRP3 inflammasome and neutrophil migration
- NSAIDs: Indomethacin, naproxen, or ibuprofen in full anti-inflammatory doses
- Corticosteroids: Prednisone or intra-articular injection for patients who cannot tolerate NSAIDs or colchicine
- IL-1 inhibitors (canakinumab, anakinra): For refractory cases or contraindications to standard therapy
Urate-Lowering Therapy (ULT)
Long-term urate-lowering therapy is indicated for patients with two or more gout flares per year, tophi, uric acid nephrolithiasis, or uric acid above 9 mg/dL:
- Allopurinol: Xanthine oxidase inhibitor; first-line therapy; start at 100 mg/day and titrate to achieve target uric acid; maximum dose 800 mg/day. HLA-B*5801 genotyping recommended before use in high-risk populations (Han Chinese, Thai, Korean) due to Stevens-Johnson syndrome risk.
- Febuxostat: Newer, non-purine xanthine oxidase inhibitor; more potent than allopurinol at standard doses; FDA label includes cardiovascular warning based on CARES trial data
- Probenecid: Uricosuric agent that blocks renal urate reabsorption; less effective in patients with CKD or kidney stones
- Pegloticase: Pegylated recombinant uricase for refractory tophaceous gout; administered intravenously every 2 weeks
Lifestyle Modifications
- Reduce or eliminate beer, spirits, and sugar-sweetened beverages
- Limit organ meats and high-purine seafood
- Increase low-fat dairy consumption
- Maintain adequate hydration (2–3 liters of water daily)
- Achieve gradual weight loss (rapid weight loss can precipitate gout flares)
- Consider vitamin C supplementation (500–1500 mg/day)
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for uric acid testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Uric acid and gout — PubMed literature search
- Hyperuricemia cardiovascular risk — PubMed literature search
- Uric acid and hypertension — PubMed literature search
- Uric acid and metabolic syndrome — PubMed literature search
- Fructose and uric acid — PubMed literature search
- Allopurinol urate lowering — PubMed literature search
- Febuxostat cardiovascular safety — PubMed literature search
- Uric acid kidney stones — PubMed literature search
- Cherry juice uric acid — PubMed literature search
- Uric acid and insulin resistance — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- Gout
- Kidney Stones
- Hypertension
- Metabolic Syndrome
- Insulin Resistance
- Obesity
- Cardiovascular Disease
- Kidney Disease
- Arthritis
- Inflammatory Markers
- Kidney Function Tests
- Organ Meats
- Vitamin C
- Chanca Piedra: Uric Acid & Gout
- Joint Pain
- Oxidative Stress
- Urinalysis
- Vitamin B3