Celiac Disease Panel (tTG-IgA)
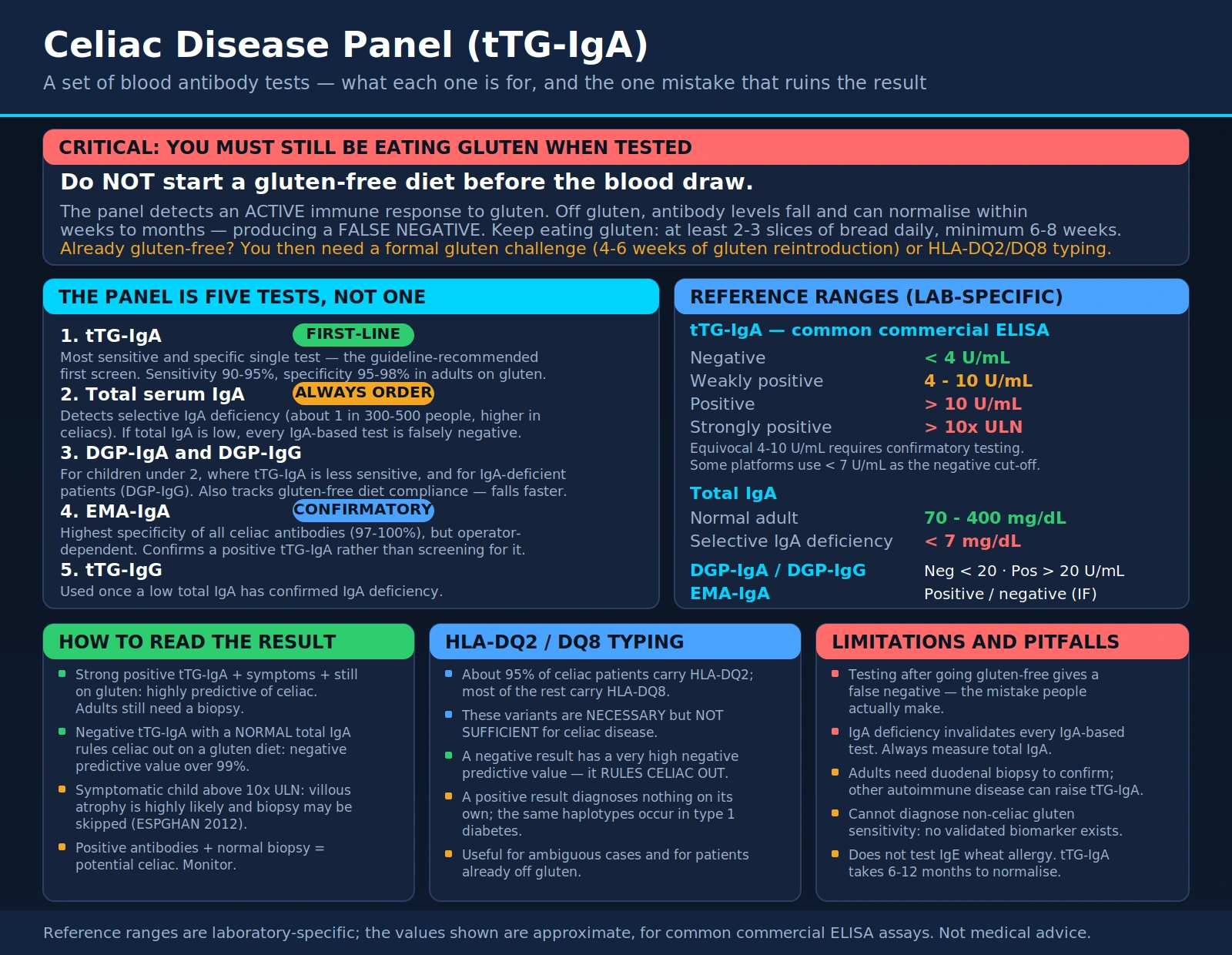
Table of Contents
- What the Celiac Disease Panel Measures
- Why the Celiac Panel Is Ordered
- How the Test Is Performed
- Components of the Celiac Panel
- Reference Ranges and Result Interpretation
- Conditions and Associations
- How Gluten Damages the Small Intestine
- How to Improve Outcomes After Diagnosis
- Limitations of Celiac Panel Testing
- Key Research Papers
- Connections
- Featured Videos
What the Celiac Disease Panel Measures
The celiac disease panel is a set of blood tests that detect autoimmune antibodies produced in response to gluten, a protein found in wheat, barley, and rye. Celiac disease is an immune-mediated condition in which gluten exposure triggers the immune system to attack the lining of the small intestine, specifically the finger-like projections called villi that are responsible for nutrient absorption. The resulting intestinal damage -- called villous atrophy -- causes malabsorption of nutrients including iron, calcium, folate, vitamin D, and vitamin B12.
The panel measures circulating immunoglobulin antibodies directed against specific self-proteins that are central to the inflammatory cascade triggered by gluten. The primary autoantigen targeted is tissue transglutaminase-2 (tTG-2), an enzyme that modifies the gliadin component of gluten, making it more immunogenic. The panel also assesses deamidated gliadin peptide (DGP) antibodies and, when IgA deficiency is suspected, IgG-class antibodies.
Celiac disease affects approximately 1% of the worldwide population, though the majority of cases remain undiagnosed. In the United States, it is estimated that only about 17-30% of individuals with celiac disease have received a formal diagnosis, making serological screening of symptomatic patients a public health priority. The celiac panel offers a non-invasive first step before the gold-standard diagnostic procedure -- small intestinal biopsy.
Why the Celiac Panel Is Ordered
Clinicians order the celiac disease panel for a range of symptomatic and high-risk-group indications:
Classic gastrointestinal symptoms:
- Chronic diarrhea or loose stools, especially fatty, pale, or foul-smelling stools (steatorrhea)
- Abdominal bloating and distension, excessive gas
- Abdominal pain and cramping after eating gluten-containing foods
- Nausea and vomiting
- Constipation (less common but present in a subset of adult celiacs)
Extraintestinal manifestations: Celiac disease is a systemic condition, and many patients present with symptoms outside the gut:
- Iron-deficiency anemia unresponsive to oral iron: One of the most common presentations in adults, caused by impaired iron absorption in the proximal small intestine.
- Osteoporosis or osteopenia at a young age: Calcium and vitamin D malabsorption causes reduced bone mineral density.
- Dermatitis herpetiformis: An itchy, blistering skin rash on the elbows, knees, and buttocks that is pathognomonic for celiac disease and responds to a gluten-free diet.
- Peripheral neuropathy: Gluten ataxia and peripheral neuropathy caused by immune-mediated nerve damage.
- Infertility and recurrent pregnancy loss: Untreated celiac disease is associated with reduced fertility in both men and women and increased risk of miscarriage.
- Short stature and delayed puberty in children: Growth retardation due to chronic malnutrition.
- Elevated liver enzymes: Celiac hepatitis (autoimmune hepatitis triggered by gluten exposure) can cause unexplained transaminase elevation.
- Fatigue and brain fog ("gluten fog"): Cognitive difficulties associated with nutritional deficiencies and neuroinflammation.
- Aphthous ulcers (mouth sores): Recurrent oral ulceration is more common in celiac disease.
High-risk groups warranting screening even without symptoms:
- First-degree relatives of diagnosed celiac disease patients (10-15% prevalence)
- Patients with type 1 diabetes mellitus (shared genetic predisposition -- HLA-DQ2/DQ8)
- Patients with autoimmune thyroid disease (Hashimoto's thyroiditis, Graves' disease)
- Patients with Down syndrome, Turner syndrome, or Williams syndrome
- Patients with selective IgA deficiency (also increases celiac risk)
How the Test Is Performed
The celiac disease panel requires a standard venous blood draw. Critically, the patient must be consuming a gluten-containing diet at the time of testing. The antibody tests detect an active immune response to gluten -- if the patient has already begun a gluten-free diet, antibody levels fall and can normalize within weeks to months, producing a false-negative result. Clinicians must instruct patients to continue eating gluten (ideally equivalent to at least 2-3 slices of bread daily for a minimum of 6-8 weeks before testing) to ensure diagnostic accuracy.
No other special preparation is required. The blood sample is analyzed for specific antibody levels using enzyme-linked immunosorbent assay (ELISA) or fluorescent enzyme immunoassay (FEIA) methods. Results are typically returned within 2-5 business days.
If serological testing is positive or strongly suspected clinically despite negative serology, the definitive diagnosis requires upper endoscopy with multiple duodenal biopsies showing characteristic histological features: villous atrophy, crypt hyperplasia, and increased intraepithelial lymphocytes (Marsh classification grade 3+). HLA-DQ2/DQ8 genetic typing can be used to exclude celiac disease (negative HLA typing has a very high negative predictive value) or to evaluate ambiguous cases.
Components of the Celiac Panel
A comprehensive celiac disease antibody panel includes several distinct immunological tests, each with specific clinical roles:
1. Tissue Transglutaminase IgA (tTG-IgA) -- First-line test:
This is the most sensitive and specific single test for celiac disease and is the recommended first-line serological marker by the American College of Gastroenterology and other major guidelines. tTG-IgA detects IgA-class antibodies targeting the enzyme tissue transglutaminase-2, the primary autoantigen in celiac disease. Sensitivity is 90-95% and specificity is 95-98% in adults eating gluten. However, because the test detects IgA-class antibodies, it will be falsely negative in patients with IgA deficiency (which occurs in approximately 1 in 300-500 people in the general population, but at higher rates in celiac patients).
2. Total Serum IgA -- Essential companion test:
A total IgA level must always accompany the tTG-IgA to detect IgA deficiency. If total IgA is low or undetectable, all IgA-based celiac antibody tests will be falsely negative regardless of celiac status, and IgG-class testing must be used instead.
3. Deamidated Gliadin Peptide IgA and IgG (DGP-IgA and DGP-IgG):
These tests detect antibodies against chemically modified (deamidated) fragments of gliadin, the alcohol-soluble component of gluten. DGP antibodies are particularly useful in young children under 2 years old, where tTG-IgA sensitivity is lower, and in IgA-deficient patients (DGP-IgG in this context). DGP tests are also used to monitor dietary compliance on a gluten-free diet -- they fall more quickly than tTG-IgA after gluten elimination.
4. Endomysial Antibody IgA (EMA-IgA) -- Highly specific confirmatory test:
EMA-IgA has the highest specificity of all celiac antibodies (97-100%) but is more technically demanding (requires indirect immunofluorescence on primate esophagus tissue) and operator-dependent. It is used primarily to confirm positive tTG-IgA results rather than as a first-line screen. EMA levels correlate with the degree of intestinal damage.
5. Tissue Transglutaminase IgG (tTG-IgG):
Used when IgA deficiency has been confirmed by low total IgA. Less sensitive than tTG-IgA in IgA-sufficient patients, but valuable in the IgA-deficient context.
Reference Ranges and Result Interpretation
Reference ranges are laboratory-specific; approximate ranges using common commercial ELISA assays:
- tTG-IgA:
- Negative: <4 U/mL (or <7 U/mL on some platforms)
- Weakly positive: 4-10 U/mL (equivocal zone requiring confirmatory testing)
- Positive: >10 U/mL (strongly suggests celiac disease)
- Strongly positive: >10x ULN (highly predictive of villous atrophy even without biopsy in symptomatic children per ESPGHAN 2012 criteria)
- Total IgA: Normal adult range 70-400 mg/dL; values <7 mg/dL are consistent with selective IgA deficiency.
- DGP-IgA and DGP-IgG: Negative: <20 U/mL; Positive: >20 U/mL (varies by platform).
- EMA-IgA: Reported as positive/negative by immunofluorescence; any positivity is considered significant given the test's high specificity.
Interpretation framework:
- A strongly positive tTG-IgA in a symptomatic patient on a gluten-containing diet is highly predictive of celiac disease. Duodenal biopsy is still recommended in most adults to confirm before committing to lifelong dietary restriction.
- A negative tTG-IgA with normal total IgA effectively rules out celiac disease in a patient on a gluten-containing diet (negative predictive value >99%).
- Weakly positive results require clinical judgment -- repeat testing, EMA-IgA confirmation, genetic testing, or biopsy depending on clinical context.
- Positive antibodies with normal small bowel biopsy may represent "potential celiac disease" -- these patients carry the genetic predisposition and immune sensitization but have not yet developed villous atrophy. Close monitoring is warranted.
Conditions and Associations
The celiac panel, when positive, confirms celiac disease and helps identify associated conditions that require management:
Nutritional deficiencies caused by malabsorption:
- Iron deficiency anemia: The most common nutritional deficiency in adult celiac disease. Iron is absorbed primarily in the duodenum and proximal jejunum -- the areas most damaged by celiac-related villous atrophy.
- Folate deficiency: Folate is also absorbed in the proximal small intestine. Deficiency causes megaloblastic anemia and elevates cardiovascular risk through homocysteine accumulation.
- Vitamin B12 deficiency: Less common than iron and folate deficiency in celiac (B12 is absorbed in the terminal ileum, which is less commonly affected), but occurs in severe cases and with concurrent atrophic gastritis.
- Vitamin D and calcium deficiency: Leads to osteoporosis, osteomalacia, hypocalcemia, and secondary hyperparathyroidism.
- Zinc deficiency: Causes impaired wound healing, immune dysfunction, and growth retardation in children.
- Magnesium deficiency: Worsens calcium absorption and neuromuscular function.
Associated autoimmune conditions:
- Type 1 diabetes mellitus: Shares HLA-DQ2/DQ8 haplotypes; 5-10% of type 1 diabetics have celiac disease.
- Autoimmune thyroid disease: Hashimoto's thyroiditis and Graves' disease are more prevalent in celiac patients than the general population.
- Autoimmune hepatitis: Elevated transaminases caused by celiac-associated liver inflammation normalize in many patients after adoption of a gluten-free diet.
- Sjogren's syndrome, lupus, rheumatoid arthritis: Celiac disease co-occurs with multiple other autoimmune conditions at higher-than-expected rates, consistent with shared immune dysregulation mechanisms.
Complications of untreated or poorly controlled celiac disease:
- Refractory celiac disease: A rare complication where villous atrophy and symptoms persist despite strict gluten-free diet adherence. Classified as type I (lymphocyte immunophenotype normal) and type II (abnormal clonal intraepithelial lymphocytes) -- the latter carries risk of enteropathy-associated T-cell lymphoma (EATL), a serious but uncommon complication.
- Non-Hodgkin lymphoma: Long-term uncontrolled celiac disease modestly increases risk of intestinal lymphoma.
- Adenocarcinoma of the small intestine: Increased risk in longstanding untreated disease, though absolute risk remains low.
- Infertility and adverse pregnancy outcomes: Resolves with gluten-free diet in most patients.
How Gluten Damages the Small Intestine
Understanding the mechanism of gluten-induced intestinal damage helps patients appreciate why strict, lifelong dietary adherence is essential. The process involves both innate and adaptive immune responses:
Step 1 -- Gluten enters the small intestine: When a person with celiac disease consumes wheat, barley, or rye, the gliadin component of gluten (a prolamin protein fraction) is only partially digested by intestinal enzymes and reaches the mucosa of the small intestine. Gliadin fragments cross the epithelial barrier through pathways that are abnormally permeable in celiac patients.
Step 2 -- Tissue transglutaminase deamidates gliadin: In the lamina propria (the connective tissue layer beneath the intestinal epithelium), the enzyme tissue transglutaminase-2 (tTG-2) chemically modifies (deamidates) glutamine residues in gliadin peptides to glutamate. This deamidation dramatically increases gliadin's affinity for HLA-DQ2 and HLA-DQ8 molecules on the surface of antigen-presenting cells. Approximately 95% of celiac patients carry HLA-DQ2 and most of the remainder carry HLA-DQ8 -- these genetic variants are necessary (though not sufficient) for celiac disease to develop.
Step 3 -- Adaptive immune activation: HLA-DQ2/DQ8-bearing antigen-presenting cells present deamidated gliadin peptides to CD4+ T helper cells, triggering a Th1/Th17 inflammatory response. These activated T cells release pro-inflammatory cytokines including interferon-gamma, interleukin-21, and interleukin-15, orchestrating the immune attack on the intestinal mucosa.
Step 4 -- Autoantibody production: The activated immune response also stimulates B cells to produce the celiac-specific autoantibodies measured in the serological panel -- anti-tTG IgA and IgG, anti-DGP, and anti-EMA antibodies. tTG-2 itself becomes an autoantigen targeted by the immune attack, perpetuating intestinal inflammation.
Step 5 -- Villous atrophy: The combined effect of inflammatory cytokines and direct immune cell activity damages the intestinal villi -- the finger-like projections that massively increase the absorptive surface area of the small intestine. Chronic damage leads to progressive villous blunting and flattening (atrophy), crypt hyperplasia (compensatory deepening of the crypts between villi), and accumulation of intraepithelial lymphocytes (IELs) within the epithelial layer. The end result is dramatically reduced absorptive surface area and impaired nutrient uptake.
How to Improve Outcomes After Diagnosis
The only effective treatment for celiac disease is strict, lifelong adherence to a gluten-free diet. However, achieving true dietary compliance is more complex than simply avoiding obvious wheat-containing foods. Practical strategies for optimal outcomes include:
Strict Gluten-Free Diet
- Eliminate all wheat, barley, and rye: This includes obvious sources (bread, pasta, cereals, crackers, pizza) and hidden sources in sauces, soups, processed meats, beer, medications, and even some vitamins and supplements with gluten-containing fillers.
- Understand "gluten-free" labeling: In the US, FDA regulations require products labeled "gluten-free" to contain fewer than 20 parts per million (ppm) of gluten. Most celiac patients tolerate this threshold, though highly sensitive individuals may react to even lower levels.
- Prevent cross-contamination: Shared cooking surfaces, toasters, cutting boards, utensils, and colanders can transfer enough gluten to cause intestinal damage. A dedicated celiac household or rigorous cross-contamination prevention protocols are essential.
- Oats: Pure, uncontaminated oats are tolerated by the majority of celiac patients but must be specifically labeled "gluten-free oats" as commercial oat supplies are heavily cross-contaminated with wheat. A small subset of celiac patients react to avenin (the oat prolamin) itself.
Nutritional Repletion
- Iron: Replete iron deficiency with oral or intravenous iron supplementation as appropriate. Monitor ferritin, serum iron, and CBC to track response. As the intestinal mucosa heals on a gluten-free diet, iron absorption improves.
- Vitamin D and calcium: Supplement based on measured 25-hydroxyvitamin D and dietary calcium intake. Consider bone density (DEXA) scanning at diagnosis and periodically thereafter.
- Folate: Many gluten-free grains are not fortified with folate (unlike wheat products in the US), so active supplementation with methylfolate is often necessary.
- Vitamin B12, zinc, magnesium: Assess and supplement deficiencies based on laboratory testing.
Monitoring After Diagnosis
- Repeat tTG-IgA and DGP antibodies at 6 and 12 months after starting a gluten-free diet to confirm they are falling toward normal -- antibody normalization correlates with intestinal healing.
- Follow-up duodenal biopsy is recommended in adults 12-24 months after starting a gluten-free diet to confirm histological healing. Many adult celiacs show slow mucosal recovery (complete healing in only 65-80% of adults after 2 years of strict diet).
- Annual review with a registered dietitian experienced in celiac disease significantly improves dietary adherence and nutritional outcomes.
Limitations of Celiac Panel Testing
- Must test on a gluten-containing diet: This is the most critical limitation. A gluten-free diet initiated before testing will cause antibody levels to fall, producing false-negative results. Patients who have already eliminated gluten require either a formal gluten challenge (4-6 weeks of gluten reintroduction) or HLA genetic typing to assess disease likelihood.
- IgA deficiency causes false negatives: Selective IgA deficiency, which is more common in celiac patients than the general population, renders all IgA-based tests invalid. Total IgA must always be measured alongside the panel.
- Positive serology requires biopsy confirmation in adults: Antibody positivity alone is not sufficient for diagnosis in adults. Other conditions (autoimmune liver disease, inflammatory bowel disease, rheumatoid arthritis) can occasionally elevate tTG-IgA. Duodenal biopsy remains the diagnostic gold standard.
- Cannot diagnose non-celiac gluten sensitivity (NCGS): NCGS is a distinct condition in which individuals experience gastrointestinal and extraintestinal symptoms from gluten in the absence of celiac disease autoimmunity or enteropathy. There are currently no validated biomarkers for NCGS -- it is a diagnosis of exclusion after celiac disease and wheat allergy have been ruled out.
- Antibodies normalize slowly after diet change: tTG-IgA levels typically take 6-12 months to normalize on a strict gluten-free diet, making early follow-up testing less informative. Persistently elevated antibodies after 12-24 months of claimed dietary adherence suggest ongoing gluten exposure (often unintentional).
- Wheat allergy vs. celiac disease: The celiac panel does not test for IgE-mediated wheat allergy, which is immunologically distinct from celiac disease and requires allergy-specific testing. Wheat allergy can coexist with celiac disease.
Key Research Papers
The following PubMed literature searches cover the evidence base for celiac disease panel testing and clinical management.
- tTG-IgA sensitivity and specificity for celiac diagnosis — PubMed
- Celiac disease prevalence and underdiagnosis — PubMed
- Villous atrophy Marsh classification in celiac disease — PubMed
- Gluten-free diet and mucosal healing in adults with celiac disease — PubMed
- Celiac disease and iron deficiency anemia — PubMed
- Celiac disease, bone density, and vitamin D — PubMed
- HLA-DQ2/DQ8 genetic risk in celiac disease — PubMed
- Deamidated gliadin peptide antibodies in pediatric celiac — PubMed
- Celiac disease associations with autoimmune thyroid and type 1 diabetes — PubMed
- Non-celiac gluten sensitivity diagnosis and differentiation — PubMed
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Celiac Disease
Connections
- All Lab Tests
- Inflammatory Markers
- Iron Panel
- Complete Blood Count (CBC)
- Vitamin B12 Test
- Vitamin D Test
- Comprehensive Metabolic Panel (CMP)
- Celiac Disease
- Vitamin D3
- Folate (Vitamin B9)
- Iron
- Calcium
- Zinc