ACTH Stimulation Test: Adrenal Insufficiency Diagnosis
The ACTH stimulation test (cosyntropin test or Synacthen test) is the gold standard for diagnosing adrenal insufficiency. By injecting a synthetic form of adrenocorticotropic hormone and measuring the cortisol response, clinicians can determine whether the adrenal glands are capable of producing adequate cortisol on demand — a question that can mean the difference between a manageable chronic condition and a life-threatening adrenal crisis.
Table of Contents
- Overview
- When Ordered
- Test Procedure
- Normal Cortisol Response
- Standard vs Low-Dose Protocol
- Primary vs Secondary Adrenal Insufficiency
- Morning Cortisol Screening
- Addison's Disease Diagnosis
- References
- Featured Videos
Overview
The ACTH stimulation test (also called the cosyntropin stimulation test or Synacthen test) evaluates adrenal gland function by measuring the cortisol response to synthetic adrenocorticotropic hormone (ACTH). Cosyntropin is a synthetic analog of the first 24 amino acids of natural ACTH — a truncated sequence that retains full biological activity at the adrenal cortex without the immunogenic properties of the full 39-amino acid molecule.
The test is the gold standard for diagnosing adrenal insufficiency — the inability of the adrenal glands to produce adequate cortisol in response to physiologic demand. Unlike a random or morning cortisol level, which reflects basal production, the stimulation test actively challenges the adrenal axis and measures the reserve capacity of the gland. This makes it far more sensitive and clinically reliable for diagnosing both overt and partial adrenal insufficiency.
Critically, the ACTH stimulation test distinguishes between two fundamentally different forms of adrenal insufficiency. In primary adrenal insufficiency (Addison's disease), the adrenal glands themselves are damaged or destroyed and cannot respond to ACTH regardless of dose. In secondary or tertiary adrenal insufficiency, the pituitary or hypothalamus fails to signal the adrenals adequately, but the adrenal glands themselves remain functional — a distinction with major implications for treatment and prognosis.
When Ordered
Clinicians order the ACTH stimulation test when adrenal insufficiency is suspected based on symptoms, history, or preliminary lab findings. Common indications include:
- Unexplained chronic fatigue, weakness, and generalized malaise that does not improve with rest
- Unintentional weight loss with loss of appetite and nausea or vomiting
- Salt craving and orthostatic hypotension (dizziness upon standing)
- Hyperpigmentation of skin and mucous membranes — particularly the palmar creases, gums, and buccal mucosa — suggesting elevated ACTH in primary disease
- Hyponatremia (low sodium), hyperkalemia (high potassium), or unexplained hypoglycemia on routine labs
- Suspected autoimmune adrenal disease, particularly in patients with other autoimmune conditions (type 1 diabetes, Hashimoto's thyroiditis, vitiligo)
- Long-term corticosteroid users being tapered — to confirm HPA axis recovery before discontinuation
- Patients with a pituitary adenoma, history of pituitary surgery or radiation, or traumatic brain injury, where pituitary ACTH secretion may be impaired
- Critical illness with hemodynamic instability disproportionate to the severity of the underlying condition — relative adrenal insufficiency in the ICU setting
- Morning cortisol in the indeterminate range of 3–18 mcg/dL, requiring functional confirmation
The test is not indicated when morning cortisol is clearly above 18 mcg/dL (adrenal insufficiency very unlikely) or clearly below 3 mcg/dL (adrenal insufficiency very likely and confirmed by clinic context without need for a stimulation challenge).
Test Procedure
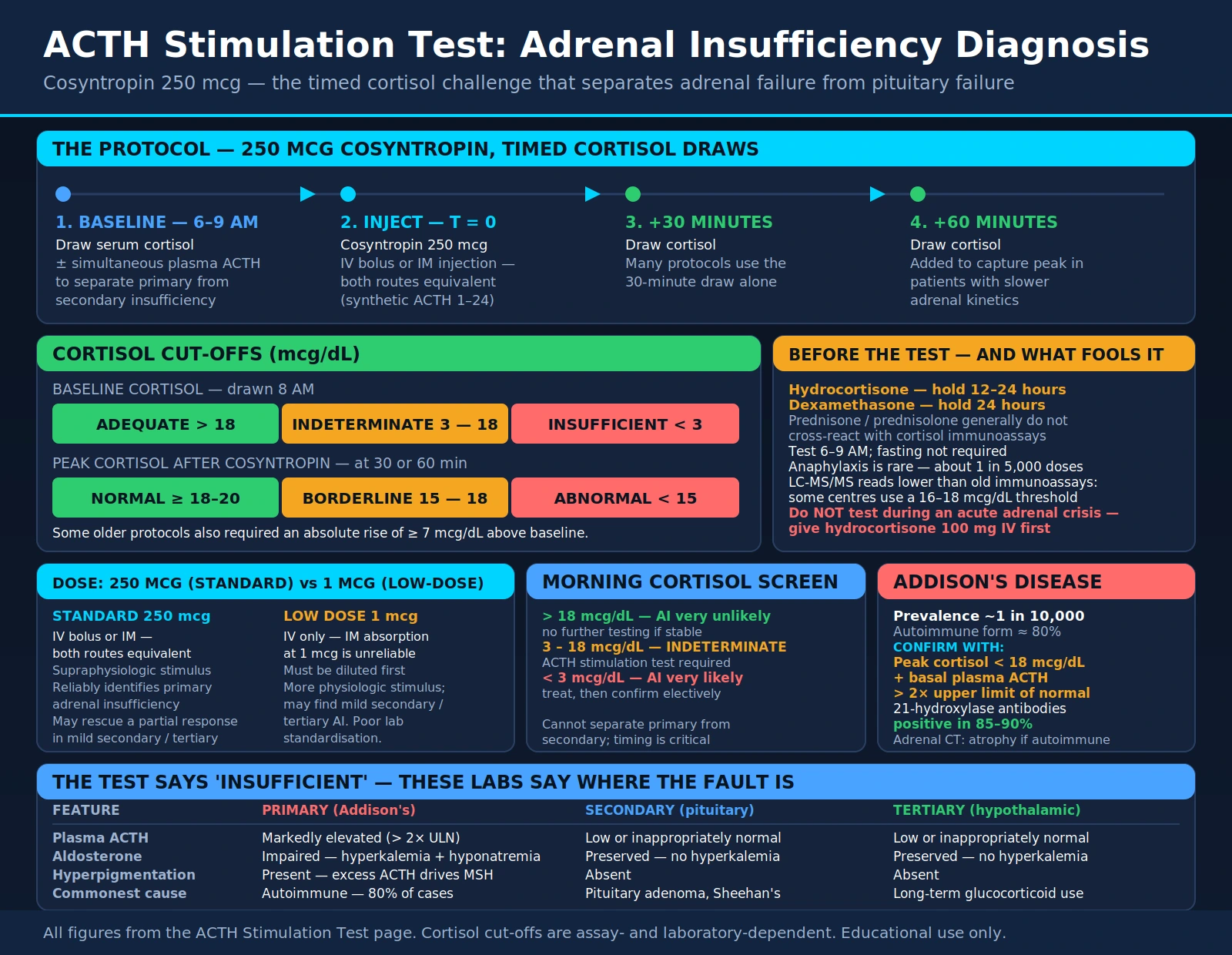
The ACTH stimulation test is typically performed as an outpatient procedure in the morning, when the adrenal axis is most active (6–9 AM). Morning testing optimizes the baseline cortisol level and reduces variability. The steps are straightforward:
- Baseline blood draw: A venous blood sample is drawn for cortisol measurement. If distinguishing primary from secondary adrenal insufficiency is a goal, a simultaneous plasma ACTH level may also be drawn at this point.
- Cosyntropin injection: 250 mcg of cosyntropin (synthetic ACTH 1–24) is administered as an intravenous (IV) bolus or intramuscular (IM) injection. Both routes are considered equivalent for the standard-dose test.
- Post-injection blood draws: Cortisol is measured at 30 minutes and/or 60 minutes after injection. Many protocols use the 30-minute draw alone; others add the 60-minute point to capture peak response in patients with slower adrenal kinetics.
Fasting is not strictly required but is often recommended to minimize variability. The test is extremely safe; adverse reactions are rare, with anaphylaxis occurring in approximately 1 in 5,000 administrations. Patients on exogenous glucocorticoids must have these withheld before testing: hold hydrocortisone 12–24 hours, dexamethasone 24 hours. Prednisone and prednisolone generally do not cross-react with most cortisol immunoassays and do not need to be withheld, though this should be confirmed with the specific assay used by the testing laboratory.
Normal Cortisol Response
The test result is interpreted based on the peak cortisol value achieved after cosyntropin injection. A normal (adequate) adrenal response requires the cortisol to rise above a defined threshold:
Baseline Cortisol (mcg/dL, drawn 8 AM)
Peak Cortisol After Cosyntropin (mcg/dL, at 30 or 60 min)
- Normal response: Peak cortisol reaches ≥18–20 mcg/dL at 30 or 60 minutes — the adrenal glands have adequate reserve capacity.
- Abnormal response: Failure to reach 18–20 mcg/dL suggests adrenal insufficiency, regardless of the baseline level.
- Absolute rise criterion: Some older protocols require a rise of ≥7 mcg/dL from baseline in addition to the absolute threshold. This is less commonly used in modern practice because a patient starting at a high baseline (e.g., 20 mcg/dL due to stress) might not show a 7 mcg/dL rise even with a fully normal adrenal response.
- Assay-dependent thresholds: The historical threshold of 18–20 mcg/dL was established with older immunoassays. Newer liquid chromatography-tandem mass spectrometry (LC-MS/MS) assays measure total cortisol more accurately and typically report lower values; some centers using LC-MS/MS use a threshold of 16–18 mcg/dL. Always interpret results in the context of the assay used by the specific laboratory.
Standard vs Low-Dose Protocol
Two cosyntropin doses are used in clinical practice, each with distinct advantages and limitations:
- Standard dose (250 mcg): The conventional protocol, used in the vast majority of clinical settings worldwide. It produces a supraphysiologic stimulus — far exceeding the ACTH concentrations that occur naturally even during severe physiologic stress. This supraphysiologic dose reliably identifies primary adrenal insufficiency (where glands are destroyed) and provides excellent reproducibility. However, because it exceeds physiologic ACTH levels by a large margin, it may rescue a partial response in mild secondary or tertiary adrenal insufficiency where glands retain some reserve capacity but would not respond adequately to physiologic ACTH levels. Can be given IV or IM.
- Low dose (1 mcg): Uses a more physiologic dose that better approximates peak endogenous ACTH concentrations. Some studies show improved sensitivity for detecting mild secondary or tertiary adrenal insufficiency — particularly HPA axis suppression from long-term exogenous glucocorticoids, where the adrenal glands have atrophied from disuse and may fail to respond to a physiologic ACTH signal even though structural destruction has not occurred. However, the low-dose test requires careful preparation (cosyntropin must be diluted, and IV administration is required as IM absorption at 1 mcg is unreliable), standardization across labs is poor, and clinical validation is less robust than for the standard dose.
The standard 250 mcg dose remains the preferred protocol in most clinical guidelines and is appropriate for the vast majority of patients. The low-dose test is reserved for specialized endocrinology centers evaluating subtle secondary or tertiary adrenal insufficiency, particularly in patients with a history of long-term glucocorticoid use.
Primary vs Secondary Adrenal Insufficiency
The ACTH stimulation test result alone does not specify the cause of adrenal insufficiency — it confirms that insufficient cortisol was produced in response to the stimulus. Distinguishing primary from secondary disease requires additional context and lab data:
- Primary adrenal insufficiency (Addison's disease): The adrenal glands themselves are damaged or destroyed. No matter how much ACTH is administered, the glands cannot respond. The cortisol response is flat. Plasma ACTH is markedly elevated because the pituitary, sensing absent cortisol feedback, drives ACTH production to maximum. Aldosterone production is also impaired in primary disease (the zona glomerulosa is destroyed along with the zona fasciculata), leading to the characteristic hyperkalemia and hyponatremia. Causes in developed countries: autoimmune (80%), tuberculosis, adrenal hemorrhage (Waterhouse-Friderichsen syndrome), bilateral adrenal metastases, HIV/AIDS, fungal infections (histoplasmosis, coccidioidomycosis).
- Secondary adrenal insufficiency: The pituitary gland does not secrete adequate ACTH. The adrenal glands are structurally intact but atrophied from prolonged disuse. Plasma ACTH is low or inappropriately normal. Because the zona glomerulosa is regulated by the renin-angiotensin system (not ACTH), aldosterone secretion is preserved — hyperkalemia does not occur, distinguishing it from primary disease. Causes: pituitary adenoma, Sheehan's syndrome (postpartum pituitary infarction), pituitary surgery or radiation, traumatic brain injury, lymphocytic hypophysitis.
- Tertiary adrenal insufficiency: The hypothalamus fails to produce adequate corticotropin-releasing hormone (CRH), so the pituitary receives no signal to make ACTH. Functionally indistinguishable from secondary disease in the ACTH stimulation test result and plasma ACTH level. The most common cause by far is long-term exogenous glucocorticoid use (prednisone, dexamethasone, inhaled corticosteroids in high doses), which suppresses the entire HPA axis through negative feedback.
Key distinguishing labs: plasma ACTH (elevated in primary, low or normal in secondary/tertiary); aldosterone response to cosyntropin (blunted or absent in primary, preserved in secondary/tertiary); 21-hydroxylase antibodies (positive in autoimmune Addison's); adrenal CT (bilateral enlargement in TB/infection/hemorrhage; atrophy in autoimmune Addison's; normal or pituitary pathology in secondary).
Morning Cortisol Screening
Before ordering an ACTH stimulation test, many clinicians obtain a morning cortisol (drawn at 8–9 AM) as an initial, lower-cost screen. This single blood draw can often stratify patients into low-probability, high-probability, and indeterminate groups:
- > 18 mcg/dL: Adrenal insufficiency is very unlikely. The morning surge in the HPA axis has produced an adequate basal cortisol level. No further testing is needed in a clinically stable patient without a highly suggestive history.
- < 3 mcg/dL: Adrenal insufficiency is very likely. This level is far below what the adrenal axis should produce at peak morning output. In the right clinical context (salt craving, hyperpigmentation, hyponatremia), treatment can be initiated and the ACTH stimulation test can be performed electively to confirm and classify.
- 3–18 mcg/dL (indeterminate): The ACTH stimulation test is required. This intermediate range cannot reliably exclude or confirm adrenal insufficiency based on basal cortisol alone, as individual variation, illness-related stress responses, and assay differences all contribute to overlap.
Limitations of morning cortisol: The test is exquisitely sensitive to timing (must be drawn 8–9 AM), acute physical or emotional stress (which can falsely elevate cortisol), laboratory assay variation, and obesity (which alters cortisol-binding globulin levels). It cannot distinguish primary from secondary disease. These limitations make the full ACTH stimulation test necessary whenever the morning cortisol result is indeterminate or the clinical suspicion remains high despite a normal result.
Addison's Disease Diagnosis
Addison's disease (primary adrenal insufficiency) is a rare but potentially fatal condition affecting approximately 1 in 10,000 people in developed countries. The autoimmune form, which accounts for roughly 80% of cases in the Western world, involves progressive destruction of the adrenal cortex by autoreactive T cells, with loss of cortisol and aldosterone production over months to years before clinical symptoms emerge.
Classic clinical presentation:
- Hyperpigmentation: The skin darkens — particularly palmar creases, buccal mucosa, gum line, recent scars, and pressure points — due to excess ACTH stimulating melanocyte-stimulating hormone (MSH) receptors. This hallmark sign is absent in secondary adrenal insufficiency because ACTH is not elevated.
- Fatigue and weakness: Profound, worsening with activity, often the earliest symptom.
- Salt craving and postural hypotension: From aldosterone deficiency causing sodium wasting and volume depletion.
- Hyponatremia and hyperkalemia: Electrolyte signature of mineralocorticoid deficiency; hyponatremia is also partially driven by cortisol deficiency impairing free water excretion.
- Weight loss, nausea, and anorexia: Gastrointestinal symptoms from cortisol deficiency.
- Hypoglycemia: Cortisol is a counterregulatory hormone; its absence impairs gluconeogenesis.
Confirmatory testing:
- ACTH stimulation test: flat cortisol response (peak <18 mcg/dL) + elevated basal plasma ACTH (>2× upper limit of normal).
- 21-hydroxylase antibodies (anti-CYP21A2): positive in 85–90% of autoimmune Addison's; a specific marker of the autoimmune form.
- Adrenal CT: atrophic adrenals in autoimmune; enlarged, calcified, or hemorrhagic adrenals in TB/infection/hemorrhage.
Adrenal crisis (Addisonian crisis): Life-threatening acute cortisol deficiency, triggered by physical stress (infection, surgery, trauma, vomiting) in a patient with undiagnosed or undertreated adrenal insufficiency. Presents with severe hypotension, vomiting, abdominal pain, altered mental status, and shock. Treatment priority: administer hydrocortisone 100 mg IV immediately — do not wait for lab confirmation. The ACTH stimulation test should NOT be performed during an acute crisis; treat first, confirm later when the patient is stable.
Maintenance therapy: Lifelong hydrocortisone (15–25 mg/day in divided doses) to replace cortisol, plus fludrocortisone (0.1 mg/day) for mineralocorticoid replacement in primary disease. Patients must carry an emergency injection kit (hydrocortisone 100 mg IM) and wear medical alert identification. Sick-day rules require doubling or tripling the oral dose during illness.
References
The following are curated PubMed literature searches covering the evidence base for the ACTH stimulation test, adrenal insufficiency diagnosis, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- ACTH stimulation test adrenal insufficiency — PubMed literature search
- Cosyntropin stimulation test cortisol response — PubMed literature search
- Primary vs secondary adrenal insufficiency diagnosis — PubMed literature search
- Addison's disease adrenal autoimmune — PubMed literature search
- Low-dose ACTH test sensitivity — PubMed literature search
- Morning cortisol adrenal insufficiency screening — PubMed literature search
- Glucocorticoid-induced adrenal suppression — PubMed literature search
- 21-Hydroxylase antibody Addison's disease — PubMed literature search
- Adrenal crisis management hydrocortisone — PubMed literature search
- Hypothalamic-pituitary-adrenal axis testing — PubMed literature search
- Cortisol threshold ACTH test modern immunoassay — PubMed literature search
- Adrenal insufficiency critical illness — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- All Lab Tests
- Addison's Disease
- Cushing's Syndrome
- Inflammatory Markers
- ESR Test
- Complete Blood Count
- Homocysteine
- Hypothyroidism
- Hyperthyroidism
- Hashimoto's Thyroiditis
- Type 1 Diabetes
- Pituitary Adenoma
- Hypertension
- Anemia
- Sodium
- Potassium
- Vitamin C
- Adaptogenic Herbs
- Lipid Panel
- Adrenal Insufficiency — the condition this test confirms or excludes by measuring the cortisol response to cosyntropin.