Adaptogens for Stress Management
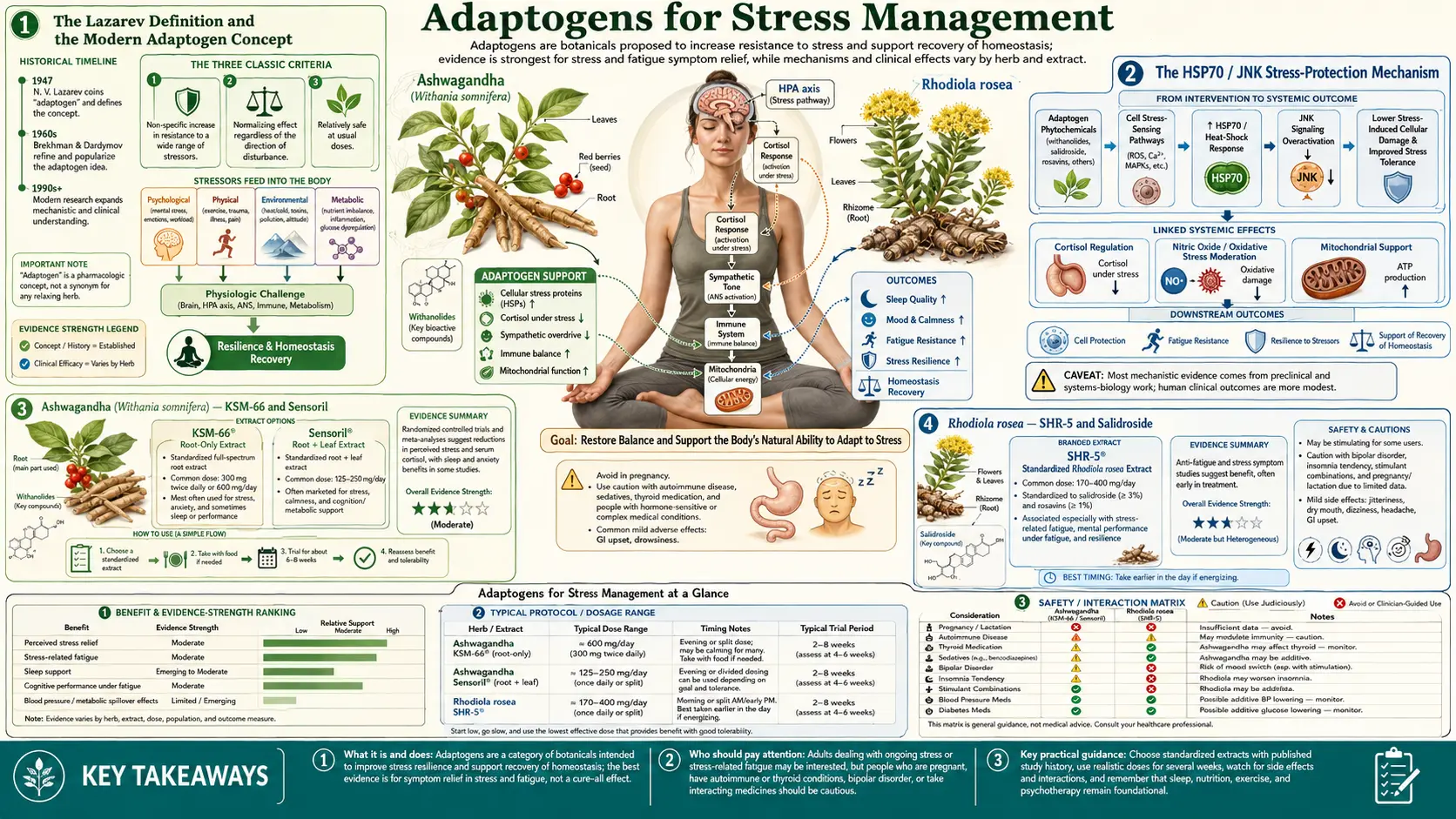
"Adaptogen" is a specific pharmacological category defined in 1957 by the Soviet toxicologist Nikolai Lazarev: a substance must (1) be relatively non-toxic at normal doses, (2) produce a non-specific increase in resistance to a broad range of physical, chemical, and biological stressors, and (3) exert a normalizing influence on the body regardless of the direction of the stress-induced abnormality. Of the thirty or so plants traditionally claimed to meet this definition, four have accumulated the largest body of high-quality randomized clinical-trial evidence in the modern literature: Ashwagandha (Withania somnifera), Rhodiola rosea, Holy Basil (Ocimum sanctum/tenuiflorum), and Schisandra chinensis. The molecular mechanism that ties them together appears to be upregulation of the heat-shock protein HSP70 and the stress-sensor kinase JNK, plus modulation of the HPA axis and the sympathetic nervous system at multiple levels. This deep-dive walks through each of the four, the standardized extracts with clinical-trial support, dosing protocols, time-to-effect, and the safety profile under chronic use.
Table of Contents
- The Lazarev Definition and the Modern Adaptogen Concept
- The HSP70 / JNK Stress-Protection Mechanism
- Ashwagandha (Withania somnifera) — KSM-66 and Sensoril
- Rhodiola rosea — SHR-5 and Salidroside
- Holy Basil (Tulsi, Ocimum sanctum)
- Schisandra chinensis
- Adaptogen Combinations and Cycling
- Dosing, Time-to-Effect, and Quality Sourcing
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
The Lazarev Definition and the Modern Adaptogen Concept
Nikolai Lazarev, a Soviet toxicologist working at the All-Union Scientific Research Institute of Pharmaceutical Chemistry, coined the term adaptogen in 1957 to describe a category of substance he believed could produce a state of "non-specific increased resistance" to stress. His student Israel Brekhman extended the work through the 1960s and 1970s, primarily studying Eleutherococcus senticosus (Siberian "ginseng," not a true Panax ginseng). The Soviet military and space programs funded the research as a search for compounds that could keep pilots, soldiers, and cosmonauts performing under sustained operational stress without the side-effect profile of stimulants like amphetamines.
The modern formalized criteria, articulated by Alexander Panossian, the leading contemporary adaptogen researcher, are:
- Decreases stress-induced damage and increases stress resistance — measured in animal models by survival time under cold, hypoxia, exhaustion, or chemical toxicity.
- Produces a normalizing effect — restores function regardless of whether the stress-induced abnormality is high or low. An adaptogen given to a hypertensive patient should lower blood pressure; the same adaptogen given to a hypotensive patient should raise it.
- Is harmless and does not disturb body functions more than necessary — broad therapeutic index, no significant withdrawal syndrome, no chronic toxicity at normal doses.
The European Medicines Agency formally accepted "adaptogen" as a pharmacological category in 2008, applying the term to Eleutherococcus, Rhodiola, Schisandra, and a small number of others. The U.S. FDA does not recognize the category and regulates adaptogens as dietary supplements under DSHEA. This regulatory difference is consequential: European pharmacopoeial-grade extracts have stricter standardization requirements than U.S. supplements.
The HSP70 / JNK Stress-Protection Mechanism
Panossian and colleagues, working at the Swedish Herbal Institute and later at the Armenian Drug and Medical Technology Agency, characterized the molecular mechanism that unifies the major adaptogens. Their 2009 Phytomedicine paper showed that Rhodiola, Schisandra, and Eleutherococcus all activate the same intracellular stress-response pathway: upregulation of heat-shock protein 70 (HSP70) and modulation of the c-Jun N-terminal kinase (JNK) stress-sensor pathway.
HSP70 is a molecular chaperone that protects proteins from misfolding and aggregation under stress. Cells preconditioned by sub-lethal stress (mild heat, mild hypoxia, mild oxidative challenge) upregulate HSP70 and become substantially more resistant to subsequent lethal stress. The phenomenon is called preconditioning or hormesis. Adaptogens appear to chemically mimic the preconditioning signal — the body responds as if it had been mildly stressed and upregulates HSP70 in anticipation of larger stress that may follow.
The JNK pathway is one of three major stress-activated MAP kinase cascades. JNK responds to oxidative stress, DNA damage, inflammatory cytokines, and physical insult; its activation drives apoptosis when stress exceeds the cell's repair capacity. Adaptogens appear to modulate JNK in a context-dependent way, suppressing pathological over-activation while preserving the appropriate physiological response.
Additional documented mechanisms include direct effects on the HPA axis (blunting of CRH-stimulated ACTH release), modulation of monoamine neurotransmitters (Rhodiola is a mild monoamine oxidase inhibitor), and effects on the cortisol-binding protein and on GABA-A receptor signaling (Ashwagandha withanolides bind GABA-A in vitro).
Ashwagandha (Withania somnifera) — KSM-66 and Sensoril
Ashwagandha is the most extensively studied modern adaptogen, with over forty randomized controlled trials in the indexed literature. The active constituents are the withanolides — a class of steroidal lactones — with withanolide A, withaferin A, and withanoside IV being the most pharmacologically significant.
Two standardized extracts dominate the clinical trial literature:
- KSM-66 — a full-spectrum root-only extract standardized to 5% withanolides, developed by Ixoreal Biomed. The 2012 Chandrasekhar trial (Indian J Psychol Med) tested 300 mg twice daily for 60 days in 64 adults with chronic stress; the active group showed a 27.9% reduction in morning serum cortisol vs 7.9% in placebo (p<0.001), and substantial improvements on the Perceived Stress Scale, Depression Anxiety Stress Scale, and General Health Questionnaire.
- Sensoril — a root-and-leaf extract standardized to 10% withanolide glycosides, 32% oligosaccharides, and <0.5% withaferin A, developed by Natreon. Auddy and colleagues (J Am Nutraceutical Assoc 2008) tested 125-500 mg/day for 60 days and found dose-dependent reductions in cortisol and improvements in fasting blood glucose, blood pressure, and self-reported well-being scores.
The Lopresti and colleagues 2019 trial (Medicine) tested 240 mg/day of a different standardized extract for 60 days in 60 adults and found significant reductions in morning cortisol and DASS-21 stress and anxiety subscale scores. Salve and colleagues (Cureus 2019) confirmed similar effects on the State-Trait Anxiety Inventory.
Typical clinical dosing is 300-600 mg/day in two divided doses, taken with meals. Time to noticeable effect is 2-4 weeks; full effect by 8-12 weeks. Ashwagandha is well-tolerated; the most common side effect is mild gastrointestinal upset. There are case reports of liver injury (typically reversible) and the herb is contraindicated in pregnancy (potential abortifacient activity) and in hyperthyroidism (Ashwagandha can raise free T4 and free T3 by 10-20%).
Rhodiola rosea — SHR-5 and Salidroside
Rhodiola rosea is a high-altitude plant native to the mountainous regions of Europe, Asia, and North America. The principal active constituents are the rosavins (rosavin, rosin, rosarin — unique to R. rosea and used as authentication markers) and salidroside (also called rhodioloside). The most thoroughly studied standardized extract is SHR-5, developed by the Swedish Herbal Institute and standardized to 3% rosavins and 1% salidroside.
Rhodiola produces effects that are notably different from Ashwagandha. Where Ashwagandha is calming and lowers cortisol, Rhodiola is mildly stimulating and improves mental performance under fatigue. The 2009 Olsson trial (Planta Medica) tested 576 mg/day of SHR-5 in 60 adults with stress-related fatigue and found significant improvements on the Pines Burnout Scale, the Beck Depression Inventory, and tests of mental performance. The 2012 Edwards review (Phytother Res) pooled trials in burnout, fatigue, and depression and concluded Rhodiola has reproducible effects on these conditions.
Two trials worth highlighting:
- Darbinyan 2007 (Nord J Psychiatry) — a 6-week trial of 340-680 mg/day of SHR-5 in 89 patients with mild-to-moderate depression found significant improvement on the Hamilton Depression Rating Scale and Beck Depression Inventory at both doses, with no significant difference between the dose groups.
- Mao 2015 (Phytomedicine) — the first randomized comparison of Rhodiola to sertraline (Zoloft) for depression. Rhodiola produced smaller absolute improvement than sertraline but with substantially fewer adverse events, yielding similar overall risk-benefit.
Typical clinical dosing is 200-600 mg/day taken in the morning or early afternoon (Rhodiola can cause insomnia if taken in the evening). Time to effect is unusually fast for an adaptogen — many patients report noticeable improvement within 3-7 days. Rhodiola is generally well-tolerated; the principal adverse effects are insomnia (avoid evening dosing), restlessness (lower dose), and rarely, increased blood pressure in susceptible individuals.
Holy Basil (Tulsi, Ocimum sanctum)
Holy Basil (Sanskrit tulsi, scientific Ocimum sanctum or the synonym Ocimum tenuiflorum) is one of the most revered plants in Ayurvedic tradition and is grown in households across the Indian subcontinent for daily consumption as a tea or chewed leaf. The active constituents include eugenol, rosmarinic acid, ursolic acid, and ocimumosides A and B.
Holy Basil is the most thoroughly multi-system adaptogen. Marc Cohen's 2014 J Ayurveda Integr Med comprehensive review summarized the trial evidence: significant effects on blood glucose (mean fasting glucose reductions of 17.6 mg/dL across pooled trials), blood pressure, lipid profile, anxiety scores (Hamilton Anxiety Rating Scale improvements of 35-39% in two trials), cognitive function, and immune markers.
The most-cited stress trial is Bhattacharyya and colleagues (2008 Nepal Med Coll J), testing 1,200 mg/day of Holy Basil leaf extract for 6 weeks in 35 adults with generalized anxiety disorder. The active group showed a 38.1% reduction in Hamilton Anxiety Rating Scale scores vs 23.9% in the comparator (p<0.001), with dose-dependent improvement in depression and stress subscale scores. The Saxena 2012 trial (Evid Based Complement Alternat Med) in 158 adults with stress-related symptoms confirmed significant improvements at 6 weeks.
Typical dosing is 300-600 mg of standardized extract twice daily, or 2-3 cups of Tulsi tea daily. Holy Basil is generally regarded as one of the safest adaptogens; the principal cautions are mild antiplatelet activity (use cautiously with anticoagulants), potential hypoglycemia in diabetics on insulin or sulfonylureas (monitor blood glucose), and theoretical reduction of fertility at very high doses based on animal studies.
Schisandra chinensis
Schisandra chinensis is a climbing vine native to northeastern China and the Russian Far East. The fruit is called wu wei zi (five-flavor berry) in traditional Chinese medicine, named for the fact that the dried berry contains all five classical flavors (sour, sweet, bitter, pungent, salty). The active constituents are the schisandra lignans — schisandrin A and B (also called gomisin A and B), schisandrol, and schisantherin — concentrated primarily in the seed.
Schisandra has the most distinctive multi-organ profile of the four major adaptogens. Beyond CNS effects, schisandra lignans are documented hepatoprotective agents — they upregulate hepatic phase I and phase II detoxification enzymes and protect hepatocytes from chemical injury. This profile makes Schisandra the adaptogen of choice for patients with chronic stress combined with hepatic insufficiency, chemical exposure, or alcohol-related liver dysfunction.
The clinical trial database is smaller than for Ashwagandha or Rhodiola but consistent. The 1999 Panossian Phytother Res trial showed 270 mg/day of standardized schisandra extract significantly reduced fatigue and improved mental performance under stress. Aslanyan and colleagues (Phytomedicine 2010) tested a combined Rhodiola-Schisandra-Eleutherococcus formula (the ADAPT-232 / Chisan formulation) in 50 women under acute psychological stress and found significant improvements in attention, speed, and accuracy.
Typical dosing is 500-1,000 mg of dried fruit extract (or 100-300 mg of a standardized lignan extract) twice daily. Schisandra is well-tolerated; the principal adverse effects are mild GI upset and occasional sleep disturbance if taken late in the day. It is contraindicated in epilepsy (theoretical reduction of seizure threshold) and should be used cautiously with sedatives.
Adaptogen Combinations and Cycling
Most modern adaptogen products combine two or more herbs to address complementary aspects of the stress response. The empirical experience is that combinations often produce a more balanced effect than single-herb monotherapy, though direct head-to-head trial evidence is limited.
- Ashwagandha + Rhodiola — the most common combination, pairing Ashwagandha's calming/cortisol-lowering effect with Rhodiola's mild stimulation and anti-fatigue effect. Useful for patients with both anxiety and fatigue.
- ADAPT-232 / Chisan — a fixed combination of Rhodiola, Schisandra, and Eleutherococcus extract studied in multiple Russian and Scandinavian trials for stress, fatigue, and immune function.
- Ayurvedic stress formulas — often combine Ashwagandha + Holy Basil + Brahmi (Bacopa monnieri) + Shankhpushpi.
- Traditional Chinese formulas — combine Schisandra with Reishi, Goji, and Astragalus for the "Eight Treasures" or similar formulations.
The question of cycling — on/off rotation rather than continuous use — is unsettled. Continuous-use trials of 8-12 weeks consistently show maintained effect without tolerance, and the longest-duration trials (up to a year for Ashwagandha) have not shown loss of effect. Traditional Ayurvedic and Chinese practice often involves cycling, but the rationale is closer to seasonal energetics than to receptor-tolerance pharmacology. Reasonable clinical practice: take the adaptogen daily for the duration of the stressor, hold the dose for 1-2 weeks every 3-6 months to confirm continued need.
Dosing, Time-to-Effect, and Quality Sourcing
Adaptogen dosing depends entirely on the standardization of the extract. Standardized extracts (KSM-66, Sensoril, SHR-5) are dosed lower than the equivalent crude herb because the active constituents are concentrated. Reference clinical-trial dosing:
- Ashwagandha — 300-600 mg/day of standardized extract (5% withanolides), in two divided doses with food. Time to effect: 2-4 weeks.
- Rhodiola rosea — 200-600 mg/day of standardized extract (3% rosavins, 1% salidroside), taken in morning or early afternoon. Time to effect: 3-14 days.
- Holy Basil — 300-600 mg of standardized extract twice daily, or 2-3 cups of Tulsi tea daily. Time to effect: 2-6 weeks.
- Schisandra chinensis — 500-1,000 mg of dried fruit extract twice daily. Time to effect: 2-4 weeks.
Sourcing matters more for adaptogens than for most herbs because (a) adulteration is common — cheaper plants are routinely substituted for true Rhodiola rosea, Holy Basil, and Schisandra chinensis — and (b) the active constituents are highly variable in unstandardized material. Reputable third-party-tested brands (Pure Encapsulations, Thorne, Gaia Herbs, Designs for Health, Banyan Botanicals) source from validated supply chains. The USP, NSF, and ConsumerLab certifications are useful proxies for quality. Avoid unstandardized "ground herb" capsules sold cheaply on Amazon — the actual content is often a small fraction of the labeled amount.
Cautions and Drug Interactions
Adaptogens are among the safest herbal categories but each has specific cautions:
- Pregnancy — Ashwagandha is contraindicated due to potential abortifacient activity. Rhodiola and Schisandra have insufficient safety data and are generally avoided. Holy Basil has been used traditionally in pregnancy but at much lower doses than therapeutic supplementation.
- Hyperthyroidism — Ashwagandha can raise free T4 and free T3 by 10-20% and is contraindicated in Graves' disease and uncontrolled thyrotoxicosis. Conversely it can be helpful in subclinical hypothyroidism.
- Autoimmune disease — theoretical concern that adaptogens with immune-stimulating effects (Eleutherococcus more than the four covered here) could worsen autoimmune disease. The clinical experience with Ashwagandha and Holy Basil in autoimmune patients is mixed; cautious use under monitoring.
- Sedatives and antidepressants — Rhodiola has mild MAO-inhibiting activity in vitro; theoretical interaction with SSRIs, SNRIs, and traditional MAOIs. Ashwagandha may potentiate benzodiazepines and GABA-A-active drugs. Schisandra induces hepatic CYP3A4 and may reduce blood levels of drugs metabolized by that enzyme (calcium channel blockers, many statins).
- Anticoagulants — Holy Basil has mild antiplatelet activity; use cautiously with aspirin, clopidogrel, or warfarin.
- Diabetes medications — both Ashwagandha and Holy Basil can lower blood glucose; patients on insulin or sulfonylureas should monitor glucose during initiation.
- Surgery — discontinue all adaptogens 1-2 weeks before scheduled surgery due to potential effects on bleeding, glucose, and anesthetic metabolism.
Key Research Papers
- Panossian A, Wikman G, Effects of adaptogens on the central nervous system (Pharmaceuticals 2010) — PubMed 27713248
- Panossian A, Wikman G, Sarris J, Rosenroot (Rhodiola rosea): traditional use, chemical composition, pharmacology and clinical efficacy Search PubMed
- Chandrasekhar K, Kapoor J, Anishetty S, A prospective randomized double-blind, placebo-controlled study of safety and efficacy of high-concentration full-spectrum extract of Ashwagandha root (KSM-66) in reducing stress and anxiety — PubMed 23439798
- Lopresti AL et al., An investigation into the stress-relieving and pharmacological actions of an Ashwagandha (Withania somnifera) extract (Medicine 2019) — PubMed 31517876
- Salve J et al., Adaptogenic and anxiolytic effects of Ashwagandha root extract in healthy adults (Cureus 2019) — PubMed 32021735
- Olsson EM, von Schéele B, Panossian AG, A randomised, double-blind, placebo-controlled, parallel-group study of the standardised extract SHR-5 of the roots of Rhodiola rosea in the treatment of subjects with stress-related fatigue (Planta Med 2009) — PubMed 19016404
- Darbinyan V et al., Clinical trial of Rhodiola rosea extract SHR-5 in the treatment of mild to moderate depression (Nord J Psychiatry 2007) — PubMed 17990195
- Mao JJ et al., Rhodiola rosea versus sertraline for major depressive disorder: a randomized placebo-controlled trial (Phytomedicine 2015) — PubMed 25837277
- Cohen MM, Tulsi — Ocimum sanctum: a herb for all reasons (J Ayurveda Integr Med 2014) — PubMed 25624701
- Saxena RC et al., Efficacy of an extract of Ocimum tenuiflorum (OciBest) in the management of general stress (Evid Based Complement Alternat Med 2012) — Search PubMed
- Panossian A, Wagner H, Stimulating effect of adaptogens: an overview with particular reference to their efficacy following single dose administration — PubMed 16261511
- Aslanyan G et al., Double-blind, placebo-controlled, randomised study of single dose effects of ADAPT-232 on cognitive functions (Phytomedicine 2010) — Search PubMed
Connections
- Stress Management Benefits Hub
- HPA Axis Regulation
- HRV Training
- Cold and Sauna Exposure
- Stress Management (Main Page)
- Ashwagandha
- Rhodiola
- Holy Basil (Tulsi)
- Schisandra
- Bacopa monnieri (Brahmi)
- Eleuthero (Siberian Ginseng)
- Reishi Mushroom
- Astragalus
- Cortisol Lab Test
- Adrenal Fatigue