Thyme Antimicrobial Spectrum
Thyme essential oil ranks alongside oregano oil as one of the two most broad-spectrum and most potent antimicrobial essential oils in the herbal pharmacy — the two herbs share the dominant active phenolic monoterpenes thymol and carvacrol but in different proportions. Published minimum inhibitory concentration (MIC) data document activity against a wide range of clinically important pathogens: methicillin-resistant Staphylococcus aureus (MRSA), Candida albicans (including fluconazole-resistant isolates), Escherichia coli, Salmonella enterica, Pseudomonas aeruginosa, Listeria monocytogenes, Klebsiella pneumoniae, and the dermatophytes Trichophyton and Microsporum. The applied uses fall into three categories: oral / dental antimicrobials (thymol is the principal active in the Listerine mouthwash family, in concentrations that have been clinically validated for plaque and gingivitis reduction), food preservation (thyme essential oil is on the FDA GRAS list as a food additive and is increasingly used in antimicrobial food packaging and natural-preservative formulations), and topical therapeutic preparations (skin, nail, wound). This deep-dive walks through the MIC data by pathogen class, the membrane-disrupting mechanism that distinguishes phenolic-monoterpene antimicrobials from beta-lactam antibiotics, the clinical mouthwash and dental literature, and the chemotype variability that determines which thyme essential oil to buy for antimicrobial use.
Table of Contents
- Thyme vs. Oregano — The Phenolic Monoterpene Family
- Membrane-Disrupting Mechanism (Why No Resistance)
- Gram-Positive Bacteria (MRSA, Streptococcus, Listeria)
- Gram-Negative Bacteria (E. coli, Salmonella, Pseudomonas, Klebsiella)
- Antifungal Activity (Candida, Dermatophytes, Aspergillus)
- Oral and Dental Applications (Mouthwash, Thymol in Listerine)
- Food Preservation and Antimicrobial Packaging
- Topical Skin and Nail Applications
- Chemotype Variability (Thymol vs. Carvacrol vs. Linalool)
- Cautions for Internal Antimicrobial Use
- Key Research Papers
- Connections
- Featured Videos
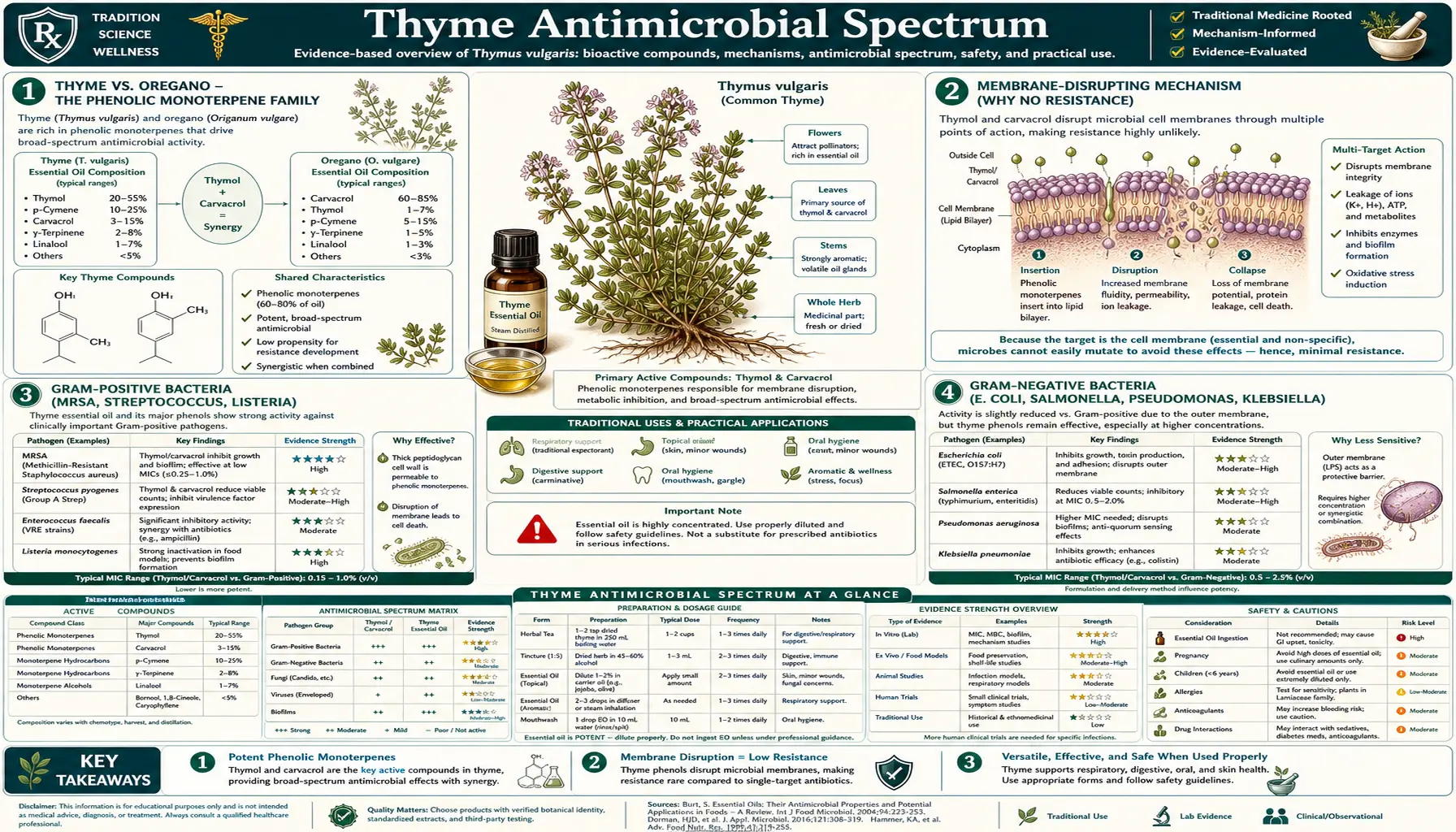
Thyme vs. Oregano — The Phenolic Monoterpene Family
Thyme and oregano are closely related Lamiaceae (mint family) herbs that share the same dominant active chemistry — the phenolic monoterpene isomers thymol and carvacrol — in different proportions. The structural difference between the two molecules is a single methyl-group position on the aromatic ring; functionally they are nearly interchangeable, with carvacrol being slightly more potent than thymol against most tested pathogens.
- Common thyme (Thymus vulgaris, thymol chemotype) — typically 40-60% thymol, 5-15% carvacrol, 15-25% p-cymene, 5-10% gamma-terpinene, with thymol clearly dominant
- Oregano (Origanum vulgare, Mediterranean type) — typically 50-80% carvacrol, 5-15% thymol, 5-15% p-cymene, with carvacrol clearly dominant
- Spanish thyme (Thymus zygis) — intermediate, often used interchangeably with T. vulgaris in the European pharmacopeia
- Wild thyme (Thymus serpyllum) — lower in phenolic monoterpenes overall (15-30%), with higher linalool and geraniol — milder and less directly antimicrobial
The practical implication: when MIC tables in the antimicrobial literature compare "thyme essential oil" and "oregano essential oil" side-by-side against a panel of pathogens, the two are usually within a 2-fold range of each other — with oregano slightly more potent against most tested species because carvacrol is slightly more potent than thymol. The two herbs are interchangeable for most antimicrobial purposes, with the choice depending on flavor, tolerability (thyme is milder), and whatever happens to be in the pantry. The Bronchipret-style respiratory indication is more firmly attached to thyme because of the traditional cough-syrup history; the antimicrobial gut-cleansing folk indication is more firmly attached to oregano (the oil-of-oregano dietary supplement category). For the related Oregano deep dive, see the dedicated page.
Membrane-Disrupting Mechanism (Why No Resistance)
Thymol and carvacrol kill bacteria, fungi, and yeasts by disrupting the integrity of the cell membrane — a fundamentally different mechanism from the conventional pharmaceutical antibiotics that target specific enzymes, ribosomes, or cell-wall synthesis machinery. The membrane-disruption mechanism has several practical consequences that distinguish phenolic-monoterpene antimicrobials from conventional antibiotics:
- Broad spectrum. Every bacterial, fungal, and yeast cell has a lipid bilayer membrane. The membrane-active mechanism therefore works against essentially all of them — gram-positive, gram-negative, aerobic, anaerobic, intracellular, biofilm-embedded. Conventional antibiotics with narrower mechanisms have narrower spectra by design.
- Resistance-resistant. Bacteria can mutate their ribosomes (against macrolides), their cell-wall enzymes (against beta-lactams), or their efflux pumps (against many drug classes) to acquire resistance to conventional antibiotics. They cannot easily mutate their entire membrane lipid composition to resist a membrane-disrupting agent — doing so would require changing the basic chemistry of life. To date, MRSA, fluconazole-resistant Candida, and other multi-drug-resistant pathogens remain fully susceptible to thymol and carvacrol in vitro.
- Synergy with conventional antibiotics. By compromising membrane integrity, thymol increases the intracellular concentration of co-administered conventional antibiotics — reversing the efflux-pump mechanism that causes much clinical antibiotic resistance. Combinations of thymol + ciprofloxacin, thymol + erythromycin, and thymol + tetracycline have all been shown to be synergistic against resistant clinical isolates in laboratory studies.
- Less selective. The flip side of the broad mechanism is that thymol can also disrupt human cell membranes at high enough concentrations. In vivo, the human gut and respiratory mucosa contain protective mucus, antioxidant enzymes, and rapid turnover that buffer against this; in vitro cytotoxicity studies show thymol cytotoxic to mammalian cells at concentrations roughly 10-50x higher than the bacterial MIC, providing a workable therapeutic index for topical and oral mucosal applications, narrower for systemic exposure.
The detailed biophysics: thymol's lipophilic phenol structure allows it to partition into the lipid bilayer of the target membrane. Once embedded, it disrupts the orderly packing of the phospholipid acyl chains, increasing membrane fluidity and permeability. At higher concentrations, it depolarizes the proton-motive force (the trans-membrane proton gradient that bacteria use to generate ATP), causes leakage of intracellular potassium and ATP, and ultimately causes cell lysis. Carvacrol works by the same mechanism with slightly higher potency, attributed to its slightly more hydrophobic side-chain geometry.
Gram-Positive Bacteria (MRSA, Streptococcus, Listeria)
Gram-positive bacteria are characterized by a thick peptidoglycan cell wall outside a single cell membrane. The cell wall itself is permeable to small lipophilic molecules like thymol, so thymol gets ready access to the underlying membrane. Published MIC values for thyme essential oil against gram-positive clinical pathogens:
- Methicillin-sensitive Staphylococcus aureus (MSSA) — thyme essential oil MIC typically 0.05-0.5% v/v (500-5,000 mcg/mL)
- Methicillin-resistant Staphylococcus aureus (MRSA) — thyme essential oil MIC essentially identical to MSSA, often 0.05-0.5% v/v. Methicillin resistance does not protect against thymol because the resistance mechanism (altered penicillin-binding protein 2a) is irrelevant to membrane disruption.
- Streptococcus pyogenes (group A strep) — thyme MIC 0.1-0.5% v/v
- Streptococcus mutans (cariogenic oral strep) — thyme / thymol MIC 0.04-0.2% v/v; the basis for thymol mouthwash plaque-control efficacy
- Enterococcus faecalis (including vancomycin-resistant VRE) — thyme MIC 0.1-1% v/v
- Listeria monocytogenes — thyme MIC 0.05-0.25% v/v; the basis for thyme oil incorporation into ready-to-eat food packaging
- Bacillus subtilis, Bacillus cereus — thyme MIC 0.05-0.5% v/v
The MRSA finding is the clinically most striking. MRSA causes a substantial fraction of healthcare-associated infections and is increasingly community-acquired; treatment options are limited and expensive (vancomycin, linezolid, daptomycin). The in-vitro evidence that thymol retains potent activity against MRSA has prompted interest in thymol-impregnated wound dressings, thymol-containing topical preparations for staphylococcal skin infections, and thymol nasal swab applications for MRSA decolonization. Clinical trials in these applications are still small and mostly proof-of-concept, but the in-vitro data is consistent and the mechanism is robust. For the related Staphylococcus aureus page, see the bacteria deep dive.
Gram-Negative Bacteria (E. coli, Salmonella, Pseudomonas, Klebsiella)
Gram-negative bacteria have an additional outer lipopolysaccharide (LPS) membrane outside the peptidoglycan cell wall, which acts as a permeability barrier that excludes many otherwise-active antimicrobials (one reason many natural antimicrobials are weaker against gram-negative than gram-positive species). Thymol can cross the LPS outer membrane reasonably well because of its small, lipophilic structure, but typical MIC values against gram-negative species are 2-4x higher than the corresponding gram-positive MIC. Still, the activity is clinically relevant:
- Escherichia coli (including ESBL-producing and multidrug-resistant clinical isolates) — thyme MIC typically 0.1-1% v/v. Activity confirmed against the diarrheagenic enterotoxigenic E. coli (ETEC) and the enterohemorrhagic E. coli O157:H7. For more on Escherichia coli see the bacteria deep dive.
- Salmonella enterica (Typhimurium, Enteritidis) — thyme MIC 0.1-0.5% v/v. The basis for thyme essential oil incorporation into poultry-feed and ready-to-eat food packaging applications.
- Pseudomonas aeruginosa — the most resistant of the gram-negative pathogens; thyme MIC typically 1-2.5% v/v. Notably, thyme oil disrupts Pseudomonas biofilms, which is clinically important because biofilm formation is the principal mechanism of Pseudomonas persistence in cystic fibrosis lung infection, chronic wound infection, and indwelling-catheter infection. For more on Pseudomonas aeruginosa, see the bacteria deep dive.
- Klebsiella pneumoniae (including carbapenem-resistant CRKP) — thyme MIC 0.1-1% v/v
- Helicobacter pylori — the gastric pathogen responsible for peptic ulcer disease and a major risk factor for gastric cancer. Thyme essential oil shows activity at MIC 0.05-0.25% v/v in vitro; clinical adjunctive use of thyme in H. pylori eradication regimens has been explored in small trials with mixed results.
- Campylobacter jejuni (foodborne diarrhea pathogen) — thyme MIC 0.05-0.25% v/v
- Vibrio cholerae — thyme MIC 0.05-0.5% v/v
The Pseudomonas biofilm activity is particularly notable because biofilm-embedded bacteria are notoriously refractory to conventional antibiotics — the biofilm matrix excludes drugs and creates anaerobic microenvironments where many antibiotics are ineffective. Phenolic monoterpenes like thymol penetrate the biofilm matrix and disrupt the embedded organisms' membranes. This has prompted research into thymol-containing topical preparations for chronic wound infection, where Pseudomonas biofilm is a major obstacle to healing.
Antifungal Activity (Candida, Dermatophytes, Aspergillus)
Fungal cell membranes have a different sterol composition from bacterial membranes — ergosterol rather than cholesterol, with different acyl-chain composition. The standard antifungal drug class (azoles like fluconazole, ketoconazole) targets ergosterol biosynthesis. Thymol and carvacrol act on the membrane downstream of the biosynthetic pathway, which means they retain activity against azole-resistant fungal isolates and offer a complementary mechanism for combination therapy.
- Candida albicans (the most common human fungal pathogen, oral and vaginal candidiasis) — thyme essential oil MIC typically 0.05-0.25% v/v. Activity is preserved against fluconazole-resistant isolates.
- Non-albicans Candida (C. glabrata, C. krusei, C. parapsilosis) — thyme MIC similar to C. albicans, an important advantage given the rising prevalence of non-albicans Candida species that are intrinsically less susceptible to fluconazole
- Dermatophytes (Trichophyton rubrum, T. mentagrophytes, Microsporum canis, Epidermophyton floccosum) — the causative organisms of tinea pedis (athlete's foot), tinea cruris (jock itch), tinea corporis (ringworm), and tinea capitis. Thyme oil MIC typically 0.05-0.25% v/v. Traditional Mediterranean topical use of thyme for fungal skin infections has good in-vitro backing.
- Aspergillus species (A. niger, A. fumigatus, A. flavus) — thyme MIC 0.1-1% v/v. The food-preservation application against Aspergillus mold spoilage of stored grain is the dominant agricultural use.
- Malassezia furfur (causative of tinea versicolor and seborrheic dermatitis) — thyme MIC 0.05-0.25% v/v
The Candida activity has clinical traction for oral candidiasis (thrush) management with thyme-containing mouthwashes and rinses, particularly in patients on inhaled corticosteroids for asthma (a common cause of oropharyngeal thrush). It also figures in the natural-medicine literature on intestinal candidiasis and "candida overgrowth" syndromes — though that broader naturopathic application is not as evidence-supported as the localized oral and topical uses.
Oral and Dental Applications (Mouthwash, Thymol in Listerine)
The most successful and widespread therapeutic application of thymol is as the principal active in the Listerine family of mouthwashes. Listerine was originally formulated in 1879 by chemist Joseph Lawrence as a surgical antiseptic, named after Joseph Lister; the recipe combines four phenolic essential-oil constituents: thymol, eucalyptol, methyl salicylate, and menthol, dissolved in 21-26% ethanol. The thymol provides the broadest-spectrum antimicrobial activity in the formula. Listerine is the most-studied antiseptic mouthwash in the dental literature, with dozens of randomized trials documenting plaque reduction, gingivitis reduction, and modest periodontitis prevention.
Key clinical findings on thymol-containing mouthwash:
- Plaque reduction. 6-month RCTs consistently show 20-50% reduction in dental plaque vs. brushing alone or placebo mouthwash. Effect size is comparable to chlorhexidine 0.12% mouthwash without the tooth-staining and taste-disturbance side effects.
- Gingivitis reduction. Similarly documented 20-40% reduction in gingivitis index scores in 6-month trials.
- Caries reduction. Less consistent but suggestive evidence for reduced incidence of dental caries with daily thymol mouthwash use, attributed to suppression of Streptococcus mutans.
- Halitosis (bad breath). Thymol's broad antimicrobial activity in the oral cavity reduces the volatile sulfur compounds produced by anaerobic oral bacteria that cause halitosis. Effect duration is typically 4-6 hours per use.
- Post-extraction infection prevention. Used as a pre-procedure rinse in dental surgery to reduce bacterial load in the surgical field.
A separate set of applications uses thymol in dental composite materials, root-canal medicaments (the venerable Camphorated Monochlorophenol or CMCP formulation includes a thymol-related compound), and as a temporary cavity sealant ingredient. The dental profession's use of thymol predates the modern antimicrobial literature by decades and is a quietly successful example of natural-product chemistry retained in mainstream medicine.
For at-home use as an antimicrobial gargle for sore throat or oral aphthous ulcers, a thyme-tea gargle (1 teaspoon dried thyme per cup of just-off-the-boil water, steeped 10 minutes, strained, cooled to warm) used 3-4 times daily is a reasonable adjunct to standard care.
Food Preservation and Antimicrobial Packaging
Thyme essential oil is on the U.S. FDA Generally Recognized As Safe (GRAS) list as a food additive and is one of the most commercially used natural food preservatives. The use cases:
- Meat and poultry preservation. Thyme essential oil at 0.05-0.5% in marinades, surface coatings, or spray applications inhibits the growth of Salmonella, Campylobacter, Listeria, and aerobic spoilage bacteria. The technology is approved for ready-to-eat meat products in the EU and has been adopted in the deli and packaged-meat industries.
- Antimicrobial food packaging. An active area of food-science research is incorporation of thyme essential oil (and oregano, clove, and other phenolic-monoterpene-rich essential oils) into edible coatings (chitosan, gelatin films) or into the inner layer of food packaging films. The packaging slowly releases volatile thymol into the food headspace, extending shelf life of meat, fish, fresh produce, and bakery products by 2-5x.
- Grain and stored-food protection. Thyme essential oil suppresses mold growth on stored grain (Aspergillus, Penicillium, Fusarium) and is used in some organic grain storage applications as a fumigant alternative.
- Beverage preservation. Low concentrations of thyme essential oil have been studied as preservatives for fruit juices and ciders.
- Probiotic-friendly preservation. An attractive feature of phenolic-monoterpene preservatives is that at sub-lethal concentrations they inhibit pathogenic and spoilage organisms while sparing the beneficial lactic-acid bacteria used in fermented foods — the mechanism is partly differential membrane sensitivity, partly the natural co-evolution of fermentation organisms with herbs.
The food-preservation literature is mostly a parallel scientific track from the medicinal literature, but the cross-referenced MIC data and mechanistic studies inform each other. Many of the clearest published MIC values for thyme essential oil against gram-negative foodborne pathogens come from food-science journals.
Topical Skin and Nail Applications
Topical applications of dilute thyme essential oil are a folk-traditional and increasingly evidence-supported approach to several skin conditions:
- Bacterial skin infection (impetigo, folliculitis, infected eczema). 1-3% thyme essential oil in a carrier oil (sweet almond, jojoba, coconut), applied 2-3 times daily, with mechanistic and small-trial support. Should not replace prescription antibiotics for cellulitis or severe infection but is a reasonable adjunct for mild superficial infection in patients seeking to limit antibiotic exposure.
- Fungal skin infection (athlete's foot, ringworm, jock itch). 2-5% thyme essential oil in carrier oil, applied 2x daily, with good in-vitro backing against the relevant dermatophytes. Tea tree oil is the more famous topical antifungal essential oil; thyme is a reasonable second choice with broader bacterial activity if the lesion is mixed.
- Onychomycosis (nail fungus). 5-10% thyme essential oil in carrier oil, applied to affected nail twice daily. Nail fungus is notoriously slow to treat (6-12 months for full nail growout) and topical penetration is poor through nail keratin; thyme oil is not a substitute for prescription oral terbinafine when full nail clearance is the goal, but is reasonable for mild superficial cases or as adjunct.
- Wound infection prevention. 0.5-1% thyme essential oil in carrier oil or hydrogel base, applied to minor cuts and abrasions after standard cleansing. Should not be used on deep, contaminated, or animal-bite wounds without medical evaluation.
- Acne. The most-cited modern dermatologic application; covered in detail in the companion Antioxidant and Acne deep-dive.
- Lice and scabies. Some folk-medicine and small-trial support for thyme essential oil as part of an essential-oil treatment for head lice; activity is real but the more concentrated tea tree oil and the prescription permethrin are more effective.
For all topical essential-oil applications, the general rule is: never apply undiluted essential oil to skin — the high phenolic concentration causes irritation and chemical burn. Always dilute to no more than 5% in a carrier oil for routine use, lower for facial application. Patch test on the inner forearm before broader use.
Chemotype Variability (Thymol vs. Carvacrol vs. Linalool)
One of the most important and underappreciated aspects of buying thyme essential oil for medicinal use is the chemotype variability. The same Latin binomial — Thymus vulgaris — covers at least six genetically distinct essential-oil chemotypes that produce dramatically different essential oils with different therapeutic indications. The standard chemotypes:
- Thymol chemotype — the canonical "thyme essential oil" of the European pharmacopeia. 40-60% thymol, the strongest antimicrobial chemotype, the standard for respiratory and antimicrobial use. This is what the medicinal literature generally describes.
- Carvacrol chemotype — less common in commercial thyme oil but available. 50-80% carvacrol, slightly more potent antimicrobially than thymol chemotype but functionally similar; closer to oregano essential oil in composition.
- Linalool chemotype — the gentlest chemotype, dominant in linalool (70-80%), with floral aroma similar to lavender. Mild antimicrobial activity but well-tolerated on sensitive skin; the preferred chemotype for pediatric topical use and for facial applications.
- Geraniol chemotype — sweet, rose-like aroma. Modest antimicrobial activity. Mostly perfumery use.
- Alpha-terpineol chemotype — lilac-like aroma. Mostly perfumery.
- Trans-sabinene hydrate chemotype — rare, mild aromatic profile.
The chemotype is determined by the plant's genetics (set at seed) and is not changeable by growing conditions. The same field can contain individual plants of multiple chemotypes; commercial producers usually clone-propagate from a single mother plant to ensure chemotype consistency. The certificate of analysis (COA) from any reputable essential-oil supplier should specify the chemotype (often written as "Thymus vulgaris ct. thymol" or "ct. linalool") and provide a gas chromatography report showing the actual percentage of major constituents. Buy thyme oil only from suppliers that publish the COA — unspecified "thyme oil" may be any of the six chemotypes, possibly adulterated with synthetic thymol, and may not deliver the medicinal effect described in this article.
For antimicrobial use: thymol chemotype, ideally 40%+ thymol per GC analysis. For pediatric or sensitive-skin application: linalool chemotype. For respiratory steam inhalation in healthy adults: thymol chemotype, 5-6 drops in a large bowl of hot water.
Cautions for Internal Antimicrobial Use
- Short-course only. Internal antimicrobial use of thyme essential oil (1-2 drops on a sugar cube or in honey, 2-3 times daily) is a high-dose phenolic monoterpene exposure and should be limited to 7-10 days at a time. Longer courses can produce gastric irritation, oral mucosal burning, and disruption of the normal commensal gut microbiome.
- Children. Internal essential oil dosing is contraindicated in children under 12 due to risk of mucosal burning and potential for seizure at accidental high doses. Thyme tea, syrup, and steam inhalation are appropriate for children.
- Pregnancy. Internal essential oil dosing is contraindicated; thyme tea at culinary-medicinal doses is acceptable.
- Inflammatory bowel disease. Caution with internal essential oil dosing in active IBD — the membrane-active mechanism can exacerbate mucosal inflammation in already-inflamed gut. Thyme tea is acceptable.
- Anticoagulant interaction. Thymol has weak antiplatelet activity; high-dose internal essential oil use should be avoided in patients on warfarin, clopidogrel, or high-dose aspirin.
- Allergic contact dermatitis. 1-2% of patch-tested individuals show sensitization to thymol or thyme essential oil. Patch test before any extended topical use.
- Photosensitivity. Not a significant issue for thyme (unlike some other essential oils such as bergamot), but high-concentration topical use plus intense sun exposure could theoretically produce localized photoirritation.
- Drug-microbiome interactions. Like any antimicrobial, internal thyme essential oil at therapeutic doses will alter the gut commensal microbiome. Consider co-administering a high-quality probiotic during and for 2 weeks after the antimicrobial course.
Key Research Papers
- Burt S (2004). Essential oils: their antibacterial properties and potential applications in foods — a review. International Journal of Food Microbiology. — PubMed
- Nazzaro F et al. (2013). Effect of essential oils on pathogenic bacteria. Pharmaceuticals. — PubMed
- Sienkiewicz M et al. (2012). Antibacterial activity of thyme and lavender essential oils. Medicinal Chemistry. — PubMed
- Lambert RJ et al. (2001). A study of the minimum inhibitory concentration and mode of action of oregano essential oil, thymol and carvacrol. Journal of Applied Microbiology. — PubMed
- Memar MY et al. (2017). Carvacrol and thymol: strong antimicrobial agents against resistant isolates. Reviews and Research in Medical Microbiology. — PubMed
- Ultee A et al. (2002). The phenolic hydroxyl group of carvacrol is essential for action against the food-borne pathogen Bacillus cereus. Applied and Environmental Microbiology. — PubMed
- DePaola LG et al. (1989). Chemotherapeutic inhibition of supragingival dental plaque and gingivitis development: long-term clinical trial of an essential oil mouthrinse (Listerine). Journal of Clinical Periodontology. — PubMed
- Stoeken JE et al. (2007). The long-term effect of a mouthrinse containing essential oils on dental plaque and gingivitis: a systematic review. Journal of Periodontology. — PubMed
- Pina-Vaz C et al. (2004). Antifungal activity of Thymus oils and their major compounds. Journal of the European Academy of Dermatology and Venereology. — PubMed
- Soliman KM, Badeaa RI (2002). Effect of oil extracted from some medicinal plants on different mycotoxigenic fungi. Food and Chemical Toxicology. — PubMed
- Lopez-Romero JC et al. (2015). Antibacterial effects and mode of action of selected essential oils components against Escherichia coli and Staphylococcus aureus. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Trombetta D et al. (2005). Mechanisms of antibacterial action of three monoterpenes. Antimicrobial Agents and Chemotherapy. — PubMed
PubMed Topic Searches
- PubMed: Thyme essential oil MIC values
- PubMed: Thymol vs. MRSA
- PubMed: Thymol antifungal
- PubMed: Listerine RCTs
- PubMed: Thyme food preservation
Connections
- Thyme Overview
- Thyme Benefits Hub
- Thyme for Respiratory Health
- Thyme Digestive Aid
- Thyme Antioxidant & Acne
- Oregano (Carvacrol Cousin)
- Garlic
- Tea Tree
- Clove
- Cinnamon
- Staphylococcus Aureus / MRSA
- Escherichia Coli
- Pseudomonas Aeruginosa
- Immune Boosting
- Honey
- All Herbs