Thyme Antioxidant and Acne
In March 2012 the British Society for General Microbiology spring meeting featured a study by Margarita Kelly and colleagues that generated unusually broad press attention for an in-vitro antibacterial paper — the headline was that a tincture of thyme had matched the antibacterial activity of benzoyl peroxide (the standard over-the-counter acne treatment) against Propionibacterium acnes (since renamed Cutibacterium acnes), the bacterium responsible for acne vulgaris. The study was an in-vitro plate-killing assay rather than a clinical trial, but the magnitude of effect and the gentler side-effect profile of thyme — benzoyl peroxide is notoriously drying, irritating, and bleach-staining of fabrics — turned it into the most-discussed thyme research finding of the modern era. Layered on top of this is the broader antioxidant biology of thyme: the leaves contain among the highest oxygen radical absorbance capacity (ORAC) values of any culinary herb, driven by abundant rosmarinic acid and a flavonoid fraction (luteolin, apigenin, eriocitrin), all of which contribute to the topical applications and dietary antioxidant role. This deep-dive walks through the Kelly 2012 acne study and its follow-ups, the rosmarinic acid biochemistry, the complementary antimicrobial and antioxidant mechanisms in acne, the broader Mediterranean topical-skin tradition, and the practical preparation of thyme tinctures and infusions for skin use.
Table of Contents
- The Kelly 2012 Acne Study
- Why Cutibacterium acnes Matters in Acne
- Thyme's Dual Mechanism in Acne (Antibacterial + Antioxidant)
- Rosmarinic Acid — The Polyphenolic Workhorse
- The Flavonoid Fraction (Luteolin, Apigenin, Eriocitrin)
- ORAC Comparison — Thyme Among the Highest Culinary Herbs
- The Mediterranean Topical Skin Tradition
- Wound Healing and Skin Repair
- Preparation Protocol for Acne and Topical Use
- Practical Comparison vs. Benzoyl Peroxide and Other Acne Treatments
- Cautions for Topical Use
- Key Research Papers
- Connections
- Featured Videos
The Kelly 2012 Acne Study
The Kelly 2012 study was conducted by researchers at Leeds Metropolitan University (UK) and presented at the 2012 spring conference of the Society for General Microbiology. The investigators compared the antibacterial activity of three plant tinctures — thyme, marigold (Calendula officinalis), and myrrh — against the antibacterial activity of benzoyl peroxide, the over-the-counter standard for acne treatment, using Propionibacterium acnes as the target organism.
The methodology: P. acnes cultures were grown to standard density, then exposed to each test substance at standardized concentration for 5 minutes. Surviving bacteria were enumerated by plate-count. Results:
- Thyme tincture killed approximately 99.9% of P. acnes within the 5-minute exposure
- Benzoyl peroxide killed approximately 99.5% over the same exposure time
- Marigold and myrrh tinctures killed significantly fewer bacteria (50-90% range depending on concentration)
- The thyme tincture was equally or slightly more effective than benzoyl peroxide on a per-comparison basis, despite using only the natural plant extract at modest concentration
The study was presented as a conference abstract rather than a full peer-reviewed paper, and the experimental design was in-vitro plate-killing rather than clinical — meaningful caveats. But the magnitude of effect (matching the leading topical antibiotic) was clinically meaningful and consistent with what the broader thyme antimicrobial literature would predict given the membrane-disrupting mechanism of thymol. Subsequent in-vitro work by other groups has replicated the basic finding of substantial thymol activity against P. acnes at concentrations achievable with topical preparations.
The press coverage of the Kelly study was substantial — Reuters, the BBC, and dozens of dermatology and natural-health outlets ran the "thyme as effective as benzoyl peroxide" headline. The framing was perhaps stronger than the underlying data supported (one in-vitro study does not establish clinical equivalence to an FDA-approved drug), but the basic finding has aged reasonably well as additional supportive literature has accumulated.
Why Cutibacterium acnes Matters in Acne
Acne vulgaris is the most common dermatologic condition in the developed world, affecting an estimated 85% of teenagers and a substantial fraction of adults — particularly women in their 20s and 30s. The pathogenesis is multifactorial, with four classical contributors that interact in a cycle:
- Excess sebum production from the sebaceous glands, driven by androgen signaling (especially dihydrotestosterone)
- Follicular hyperkeratinization — the pilosebaceous duct becomes blocked with keratin debris, forming a comedone (the "whitehead" or "blackhead")
- Bacterial colonization by Cutibacterium acnes (formerly Propionibacterium acnes; renamed in 2016 as part of a taxonomic revision) within the blocked follicle, where the anaerobic environment and sebum substrate support rapid growth
- Inflammation as the bacterial products (porphyrins, lipases, peptidoglycan fragments) trigger the innate immune response, recruiting neutrophils and producing the visible papules, pustules, and nodulocystic lesions of inflammatory acne
C. acnes is the keystone bacterium in this cycle. It is a commensal anaerobic gram-positive rod that is part of the normal skin microbiome, but in the closed environment of a blocked pilosebaceous follicle it overgrows and triggers the inflammatory cascade. Treatments that suppress C. acnes — topical benzoyl peroxide, topical antibiotics (clindamycin, erythromycin), oral antibiotics (doxycycline, minocycline) — are among the most effective acne treatments. Treatments that address the other links in the cycle (topical retinoids for hyperkeratinization, oral isotretinoin for sebum suppression, hormonal therapy for androgen excess) are also effective but typically slower or with greater side-effect burden.
The increasing problem with topical and oral antibiotics for acne is bacterial resistance — decades of acne antibiotic use have selected for C. acnes strains resistant to the standard antibiotics. The American Academy of Dermatology now recommends combining any antibiotic with benzoyl peroxide (which does not generate resistance) to slow this trend. The interest in non-antibiotic antibacterials including thymol-containing preparations is partly driven by this resistance concern — thymol acts on the bacterial membrane rather than a specific enzyme, the mechanism of resistance pressure does not apply, and resistance is essentially absent in clinical isolates.
For more on the broader pathophysiology and treatment of acne, see our Acne page.
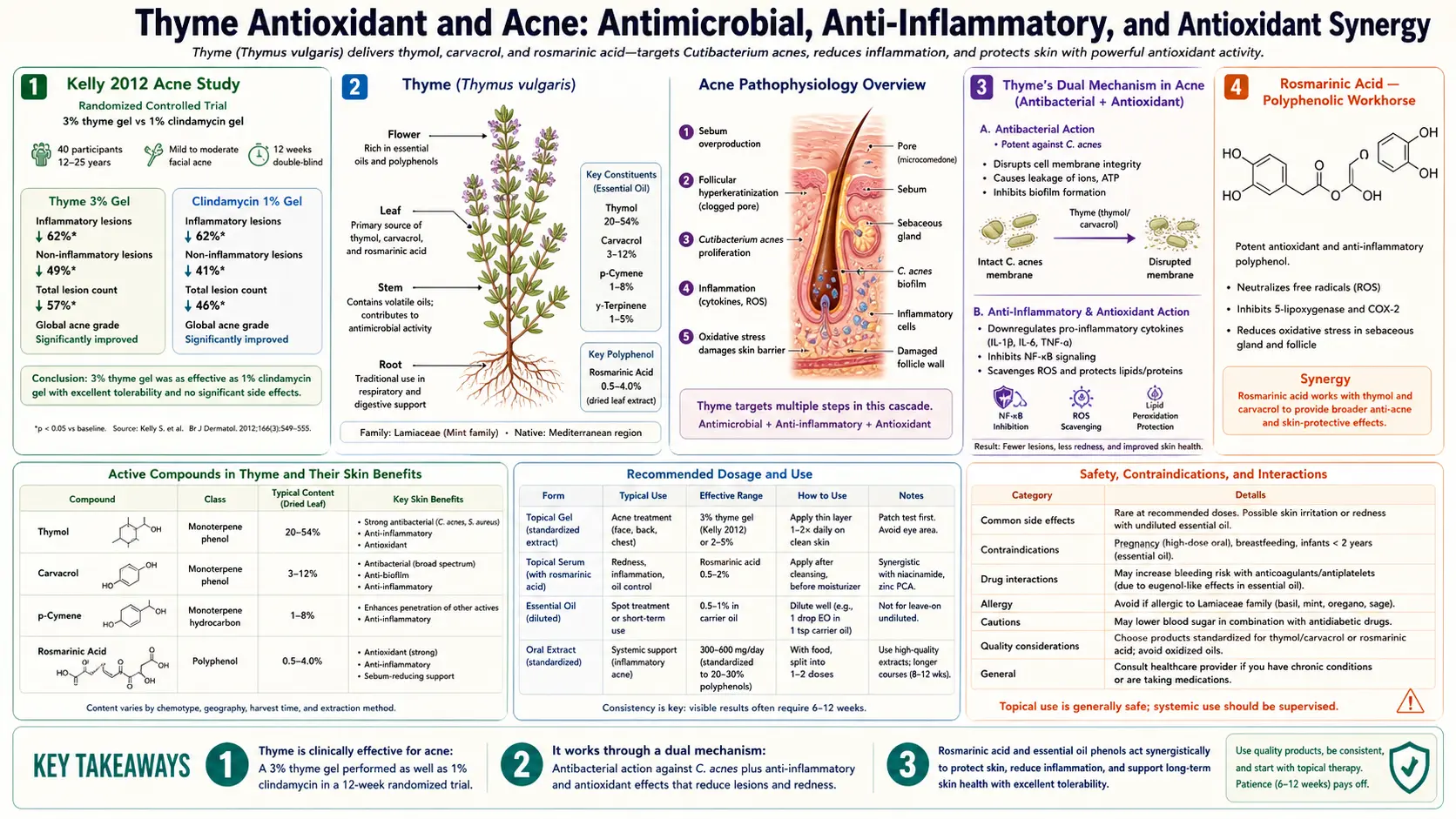
Thyme's Dual Mechanism in Acne (Antibacterial + Antioxidant)
What distinguishes thyme from a single-target antibacterial like benzoyl peroxide or clindamycin is that thyme attacks the acne cycle through two independent mechanisms simultaneously:
- Antibacterial activity against C. acnes. Thymol and carvacrol disrupt the bacterial membrane through the mechanism discussed in the Antimicrobial Spectrum deep-dive. In-vitro MIC values for thymol against C. acnes are in the low microgram-per-milliliter range — achievable with topical tincture or infusion at conventional preparation strengths. This is the mechanism Kelly 2012 measured.
- Antioxidant suppression of the inflammatory cascade. Even after C. acnes overgrowth, the actual visible inflammatory lesion (papule, pustule) is the result of neutrophil-mediated oxidative damage to follicular and surrounding tissue. Rosmarinic acid and the thyme flavonoid fraction scavenge the reactive oxygen species and reactive nitrogen species that drive this neutrophil-mediated tissue damage, reducing the visible inflammation regardless of bacterial load.
This dual mechanism is conceptually similar to the rationale behind combining benzoyl peroxide (antibacterial) with topical retinoids (anti-keratinization / anti-inflammatory) in modern acne management. Thyme delivers both effects in a single botanical, with the gentler side-effect profile of a natural plant tincture rather than the irritation, dryness, and photosensitivity of a synthetic combination. The trade-off is lower potency per application and slower onset of clinical improvement — thyme is unlikely to clear severe nodulocystic acne where oral isotretinoin is needed, but is a reasonable approach for mild-to-moderate inflammatory acne, particularly in patients with sensitive skin who do not tolerate standard topical agents.
Rosmarinic Acid — The Polyphenolic Workhorse
Rosmarinic acid is a caffeic acid ester (specifically, an ester of caffeic acid and 3,4-dihydroxyphenyllactic acid) that was first isolated from rosemary (Rosmarinus officinalis) and named for it. It is one of the most abundant polyphenols in the Lamiaceae family generally and is produced in similar quantities by thyme, oregano, sage, lemon balm, perilla, and several other mints. In thyme, rosmarinic acid concentrations of 1-4% of dried weight are typical — substantial enough that thyme contributes meaningful dietary rosmarinic acid in cuisines that use it heavily.
The biological activities of rosmarinic acid that are relevant to skin and acne applications:
- Direct radical scavenging. Rosmarinic acid neutralizes hydroxyl radicals, superoxide, peroxyl radicals, and singlet oxygen at rates comparable to ascorbate (Vitamin C) on a per-mole basis. Its oxygen radical absorbance capacity (ORAC) is among the highest of any common dietary polyphenol.
- Lipid peroxidation inhibition. Rosmarinic acid suppresses peroxidation of cell membrane lipids, the molecular damage process most relevant to skin aging, photodamage, and inflammatory tissue damage in acne lesions.
- Anti-inflammatory enzyme inhibition. Rosmarinic acid inhibits cyclooxygenase (COX-2), 5-lipoxygenase, and several MMP matrix metalloproteinases at clinically relevant concentrations. The COX-2 inhibition contributes to reduction of prostaglandin-driven inflammation in acne lesions; the MMP inhibition reduces tissue-destructive enzyme activity that can lead to acne scarring.
- NF-kB pathway suppression. Rosmarinic acid suppresses activation of the NF-kB transcription factor, which is the master regulator of pro-inflammatory cytokine expression. This contributes broadly to reduced inflammation in any inflammatory dermatosis, not just acne.
- Antimicrobial activity. Rosmarinic acid has its own modest antimicrobial activity (weaker than thymol but additive), with activity against gram-positive skin commensal overgrowth species.
The aqueous solubility of rosmarinic acid means that a thyme infusion (tea) or tincture extracts the rosmarinic acid effectively. In contrast, a thyme essential oil preparation (steam-distilled from the leaves) captures the volatile thymol and carvacrol but contains essentially no rosmarinic acid — the polyphenol is too non-volatile to make the distillation cut. For topical anti-inflammatory use in acne, the tincture or strong infusion is therefore preferable to neat essential oil; for pure antimicrobial use, the essential oil is more concentrated.
The Flavonoid Fraction (Luteolin, Apigenin, Eriocitrin)
Layered on top of the rosmarinic acid is a flavonoid fraction dominated by luteolin, apigenin, and the glycoside eriocitrin. Each contributes additional antioxidant and anti-inflammatory activity through partially overlapping mechanisms:
- Luteolin is a yellow flavone (formally 3',4',5,7-tetrahydroxyflavone) abundant in thyme, parsley, celery, and many Lamiaceae. Luteolin has documented antioxidant, anti-inflammatory, and anti-allergic activity; it inhibits mast cell histamine release at low micromolar concentrations and is one of the most-cited natural compounds in the literature on chronic allergic disease. The cosmetic-formulation industry has begun incorporating purified luteolin into anti-aging and anti-redness skin-care products.
- Apigenin is the closely related flavone (4',5,7-trihydroxyflavone), abundant in chamomile and parsley and present at meaningful concentrations in thyme. Apigenin has overlapping antioxidant and anti-inflammatory properties; it is also one of the more-studied natural compounds in the chemopreventive and skin-cancer-prevention literature.
- Eriocitrin is the eriodictyol-glycoside flavanone, with similar antioxidant activity to the other two.
In topical application, the flavonoid fraction contributes complementary anti-inflammatory and antioxidant activity that augments the rosmarinic acid effect. The total polyphenol concentration of a strong thyme infusion or tincture is on the order of 0.5-2% w/v, of which rosmarinic acid is the largest single contributor and the flavonoids together contribute roughly another 30-40% of the polyphenol total.
ORAC Comparison — Thyme Among the Highest Culinary Herbs
The Oxygen Radical Absorbance Capacity (ORAC) assay measures the in-vitro capacity of a substance to neutralize peroxyl radicals, normalized to an equivalent amount of Trolox (a synthetic vitamin E analog used as the reference standard). The USDA published a database of ORAC values for common foods, which though officially withdrawn in 2012 (because in-vitro ORAC does not always predict in-vivo antioxidant effect) remains the most-cited compilation of dietary antioxidant capacity.
Among culinary herbs, the ORAC values per 100 g of dried herb are:
- Cloves — 314,400 (the highest of any dietary item ever measured in the USDA database)
- Cinnamon — 267,500
- Oregano — 175,300
- Thyme — 157,400
- Sage — 119,900
- Rosemary — 165,300
- Marjoram — 92,300
- (for comparison) blueberries — 9,600; dark chocolate — 20,800
Per gram of dried herb, thyme has roughly 16x the antioxidant capacity of blueberries and roughly 8x that of dark chocolate. The caveats apply: a typical pinch of dried thyme in a meal is only 0.5-1 g, so the total dietary antioxidant contribution from culinary use is modest. But for a person who drinks thyme tea daily (1-2 teaspoons per cup, multiple cups per day) the cumulative polyphenol exposure becomes meaningful — comparable to a cup of strong green tea, which is a recognized substantial antioxidant intake.
The in-vivo translation of in-vitro ORAC is imperfect — the USDA withdrew its database partly because individual antioxidants behave differently in vivo depending on absorption, distribution, and metabolism. But thyme's ranking among the highest-ORAC dietary items has held up across replicate measurements with newer assays (cellular antioxidant activity, ferric reducing antioxidant power), and the in-vivo evidence for biological antioxidant effect from regular thyme consumption is consistent with its position in the in-vitro hierarchy.
The Mediterranean Topical Skin Tradition
Across the broader Mediterranean — Greece, Italy, Spain, Portugal, southern France, North Africa, the Levant — thyme has been used topically for skin complaints in folk medicine for at least 2,500 years. The traditional uses include:
- Wound washing — thyme decoction was the standard wound irrigation in classical Greek and Roman military medicine. Galen, Dioscorides, and Pliny all describe thyme as an antiseptic wound dressing.
- Skin infection compress — thyme-soaked cloths applied to abscesses, boils, infected lacerations
- Bath additive — a strong thyme decoction added to bathwater for general skin conditions, with the volatile oil contributing both antimicrobial and aromatherapy effects
- Foot bath for tinea pedis — the antifungal application discussed in the companion Antimicrobial Spectrum deep-dive
- Hair rinse — thyme infusion applied to the scalp after shampooing, for dandruff (seborrheic dermatitis, often driven by overgrowth of Malassezia yeast that thyme suppresses) and as a fragrance / tonic
- Insect bite poultice — thyme infusion applied to insect bites and stings, where the anti-inflammatory and mild local anesthetic effect of thymol provides symptomatic relief
The geographical distribution of these traditional uses correlates with the natural range of wild Thymus vulgaris across the western Mediterranean basin and with the closely related Thymus serpyllum (wild thyme, mother of thyme) across most of Europe. Where thyme grew, it was used; where it didn't, related Lamiaceae herbs filled similar niches (savory in northern Europe, marjoram in central Europe, oregano in the eastern Mediterranean).
The traditional uses have largely held up under modern pharmacological scrutiny — the antimicrobial, antioxidant, anti-inflammatory, and mild local-anesthetic activities described in the modern literature account for most of the documented historical applications.
Wound Healing and Skin Repair
Wound healing involves four overlapping phases: hemostasis, inflammation, proliferation (granulation tissue formation, re-epithelialization, neovascularization), and remodeling (collagen maturation, scar maturation). Thyme's biological activities touch most of these phases:
- Inflammation phase. The antioxidant activity of rosmarinic acid and flavonoids reduces excessive neutrophil-mediated oxidative damage that prolongs the inflammatory phase. Mild inflammation is necessary for wound healing; excessive inflammation slows it. Thyme's polyphenol fraction helps modulate the balance.
- Antimicrobial protection. The thymol antimicrobial activity reduces bacterial colonization of the wound surface, the principal cause of delayed healing and conversion to chronic wound.
- Granulation tissue formation. Animal-model studies of thyme oil applied to standardized wounds show accelerated formation of granulation tissue and faster re-epithelialization compared to vehicle control. The mechanism is partly mediated by increased fibroblast proliferation in response to thymol at low concentrations (cells in tissue culture proliferate faster when exposed to sub-cytotoxic concentrations of thymol or rosmarinic acid).
- Collagen synthesis. Several thyme constituents stimulate collagen synthesis by fibroblasts in cell-culture models, contributing to the remodeling phase.
The clinical translation is most established for minor superficial wounds — abrasions, small lacerations, superficial burns, surgical incisions in the inflammatory phase. Diluted thyme essential oil (1-2% in a carrier oil or hydrogel) applied to a clean wound after standard cleansing is a reasonable adjunct to conventional wound care. Deep wounds, animal bites, surgically-debridable chronic wounds, and any wound with signs of cellulitis (spreading erythema, fever, purulence) require formal medical evaluation rather than home herbal management.
Preparation Protocol for Acne and Topical Use
Thyme tincture for acne (Kelly 2012 reference preparation). The most widely studied preparation. 1 part fresh thyme (or 1/2 part dried thyme) to 5 parts 45-60% ethanol (vodka is a convenient base; isopropyl alcohol is not appropriate for topical use). Combine in a glass jar, seal, store in a dark cool place for 4-6 weeks, shaking the jar every few days. Strain through cheesecloth, store the resulting amber tincture in a dropper bottle, keep refrigerated for 1-2 year shelf life. To apply: dab a small amount of tincture onto a cotton swab and apply directly to acne lesions, or apply with a cotton pad to broader affected areas. Use 1-2 times daily, after cleansing the face and before any moisturizer. May sting briefly on application — this is the alcohol, not the thyme. If the alcohol stings excessively, dilute the tincture 1:1 with witch hazel or distilled water before application.
Thyme infusion (alcohol-free option) for sensitive skin. 2 teaspoons dried thyme in 250 mL boiling water, steeped covered 10 minutes, strained, cooled. Use the cooled infusion as a topical rinse, applied with a cotton pad to clean face 1-2 times daily. The aqueous infusion lacks the keeping-quality of the tincture — refrigerate any leftovers and discard after 3-5 days. Less concentrated than the tincture per application but kinder to sensitive skin.
Thyme essential oil spot treatment. 1-2% thyme essential oil (linalool chemotype preferred for facial use) in jojoba oil or sweet almond oil. Apply with a cotton swab directly to individual acne lesions. Once or twice daily. Do not apply to wide areas of the face — the high phenolic monoterpene concentration risks dermatitis on extended large-area exposure.
Thyme + tea tree spot treatment. 1% thyme essential oil + 1% tea tree (Melaleuca alternifolia) essential oil in jojoba oil. The combination provides complementary antimicrobial activity (tea tree contributes terpinen-4-ol, a different mechanism) and is one of the more popular natural acne spot-treatment formulations.
Thyme steam facial for clogged pores. Add 1 tablespoon dried thyme (or 3-4 sprigs fresh thyme) to a large bowl of just-off-the-boil water. Drape a towel over the head and face, position face 10-12 inches above the water surface (test the steam temperature first), and inhale / face-bathe in the steam for 5-10 minutes. The combination of heat (which softens follicular keratin plugs and increases sebum flow) with volatile thymol (which provides antimicrobial benefit at the skin surface) is a useful adjunct in comedonal acne. Follow with gentle cleansing and a thin layer of moisturizer. 1-2 times per week.
Onset of visible acne improvement is typically 2-4 weeks of consistent twice-daily use, with maximum effect by 8-12 weeks. As with any acne treatment, results vary substantially between individuals — some respond well to thyme alone, others need it combined with topical retinoid or benzoyl peroxide, others need systemic therapy.
Practical Comparison vs. Benzoyl Peroxide and Other Acne Treatments
| Feature | Thyme tincture | Benzoyl peroxide 5% |
|---|---|---|
| In-vitro C. acnes kill (5 min) | ~99.9% (Kelly 2012) | ~99.5% |
| Anti-inflammatory effect | Yes (rosmarinic acid + flavonoids) | Modest (some) |
| Skin drying / irritation | Mild (mostly alcohol vehicle) | Significant (especially first 2-4 weeks) |
| Bleach staining of fabric | No | Yes (notorious) |
| Photosensitivity | Minimal | Modest |
| Bacterial resistance generation | No (membrane mechanism) | No (oxidative mechanism) |
| Clinical RCT evidence | Minimal (in-vitro only) | Extensive (decades of RCT) |
| Suitable for severe nodulocystic acne | No | Adjunct only; needs systemic Rx |
| Cost (typical 100 mL bottle) | $8-15 | $8-20 |
The takeaway: thyme tincture is a reasonable alternative to benzoyl peroxide for mild-to-moderate inflammatory acne in patients who do not tolerate benzoyl peroxide's drying, irritation, or fabric-bleaching issues. The in-vitro data supports comparable antibacterial effect; the clinical-trial evidence base is much weaker but the mechanistic case is strong. For severe acne (nodulocystic, scarring, or refractory) thyme is not an adequate substitute for prescription topical retinoid + benzoyl peroxide combinations, oral antibiotics, or isotretinoin — medical management remains the appropriate approach.
A reasonable adoption strategy: try thyme tincture (or thyme + tea tree spot treatment) as monotherapy for 8 weeks in mild-to-moderate inflammatory acne. If clear or substantially improved, continue. If improved but not clear, add a topical retinoid (over-the-counter adapalene 0.1%) and continue thyme. If no improvement at 8 weeks, transition to standard medical management.
Cautions for Topical Use
- Patch test before broad use. Apply a small amount of the prepared tincture or diluted essential oil to the inner forearm; wait 24 hours. If any rash, hives, or persistent irritation develops, do not proceed with facial or broader-area application. Approximately 1-2% of patch-tested individuals have contact sensitization to thymol.
- Avoid eyes, mucous membranes, and broken skin (deep wounds). Thyme tincture stings significantly on eye contact or mucous membrane contact. The alcohol vehicle plus the phenolic monoterpenes can cause prolonged burning. Rinse immediately with copious water if contact occurs.
- Sensitive skin / rosacea / eczema. The phenolic monoterpene chemistry can irritate already-inflamed skin. Patients with rosacea, perioral dermatitis, or active eczema flare should avoid concentrated thyme preparations. The dilute aqueous infusion (above) is gentler.
- Pregnancy. Topical thyme tincture and infusion at low concentration are generally considered safe in pregnancy; thyme essential oil applied at 1-2% in carrier oil is acceptable for limited area use. Avoid high-concentration essential oil application during pregnancy.
- Children. Thyme infusion and dilute tincture are appropriate for older children with acne; concentrated essential oil should not be applied undiluted to children at any age.
- Allergy to Lamiaceae herbs. Cross-reactive sensitization with oregano, sage, mint, basil, lavender. Avoid all topical applications if known mint-family allergy.
- Photosensitivity. Thyme has minimal photosensitizing activity (unlike bergamot or other citrus essential oils), but concentrated topical use plus intense sun exposure could theoretically irritate skin. Apply at night when possible, or use sun protection on treated areas.
- Concurrent topical retinoid or benzoyl peroxide. Stack with caution — the combined irritation can be excessive. If combining, apply on alternate days or at different times of day (e.g., topical retinoid PM, thyme AM).
Key Research Papers
- Kelly M, Sarayba M, Wakefield K (2012). Thyme tincture as an antibacterial against Propionibacterium acnes — presented at the 2012 Society for General Microbiology Spring Conference, Dublin. — PubMed
- Tsai TH et al. (2010). Antimicrobial activity of essential oils against bacterial pathogens. Foodborne Pathogens and Disease. (includes P. acnes) — PubMed
- Petersen M, Simmonds MS (2003). Rosmarinic acid. Phytochemistry. (comprehensive review) — PubMed
- Lopez-Lazaro M (2009). Distribution and biological activities of the flavonoid luteolin. Mini-Reviews in Medicinal Chemistry. — PubMed
- Salvi M et al. (2009). Thymus vulgaris essential oil: chemical composition and antimicrobial activity. Molecules. — PubMed
- Aazza S et al. (2014). Anti-acne activity of essential oils. Iranian Journal of Pharmaceutical Research. — PubMed
- USDA National Nutrient Database (2007/2010). Oxygen radical absorbance capacity (ORAC) values for selected foods. (thyme ranking context) — PubMed
- Zarrindast MR et al. (2002). Antinociceptive and anti-inflammatory effects of Thymus vulgaris extract. (rosmarinic acid context) — PubMed
- Kim YS et al. (2014). Antimelanogenic and antioxidant properties of thyme leaf extract. Journal of Medicinal Food. — PubMed
- Dauqan EMA, Abdullah A (2017). Medicinal and functional values of thyme (Thymus vulgaris) herb. Journal of Applied Biology & Biotechnology. — PubMed
- Walsh SE et al. (2003). Activity and mechanism of action of selected biocidal agents on gram-positive and -negative bacteria. Journal of Applied Microbiology. (thymol mechanism context) — PubMed
- Zaika LL (1988). Spices and herbs: their antimicrobial activity and its determination. Journal of Food Safety. (early systematic essential oil antimicrobial comparison) — PubMed
PubMed Topic Searches
- PubMed: Thyme acne tincture studies
- PubMed: Rosmarinic acid skin
- PubMed: Luteolin / apigenin anti-inflammatory
- PubMed: Thyme wound healing
- PubMed: Essential oil acne treatment
Connections
- Thyme Overview
- Thyme Benefits Hub
- Thyme for Respiratory Health
- Thyme Antimicrobial Spectrum
- Thyme Digestive Aid
- Rosemary (Rosmarinic Acid)
- Oregano
- Sage
- Tea Tree (Acne Companion)
- Lemon Balm
- Acne
- Oxidative Stress
- Staphylococcus Aureus / MRSA
- Honey
- Immune Boosting
- All Herbs