Thyme for Respiratory Health and Cough
Thyme (Thymus vulgaris) is the most-traditional cough and bronchitis remedy in European folk medicine, and one of the few medicinal herbs to have crossed from folk use into formal regulatory approval. The German Commission E — the most rigorous national herbal-medicine regulatory body in Europe — lists thyme as an approved treatment for symptoms of bronchitis, whooping cough, and upper respiratory catarrh, on the strength of pharmacological mechanism and modern clinical trials. The flagship modern product, Bronchipret (a fluid extract combining thyme with ivy leaf), has been studied in randomized placebo-controlled trials in over 1,200 acute-bronchitis patients and consistently produces faster cough resolution and fewer coughing episodes than placebo. The active mechanism is well-mapped: thymol stimulates ciliary beat frequency in respiratory epithelium, reduces the viscosity of bronchial mucus (the secretolytic / expectorant effect), and relaxes bronchial smooth muscle, while contributing antimicrobial activity against the bacterial superinfection pathogens that complicate viral bronchitis. This deep-dive walks through the Commission E indication, the Bronchipret evidence, the pharmacology, and the practical use of thyme tea, syrup, and steam inhalation for adults and children.
Table of Contents
- The German Commission E Approval
- The Bronchipret (Thyme + Ivy) Bronchitis Trials
- Secretolytic and Expectorant Mechanism
- Ciliary Beat Frequency and Mucociliary Clearance
- Bronchospasmolytic (Antispasmodic) Effect
- The European Cough Syrup Tradition
- Pediatric Use and the Thyme-Primrose Trials
- Preparation Forms: Tea, Tincture, Syrup, Steam, Essential Oil
- Adult Clinical Protocol for Acute Bronchitis
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
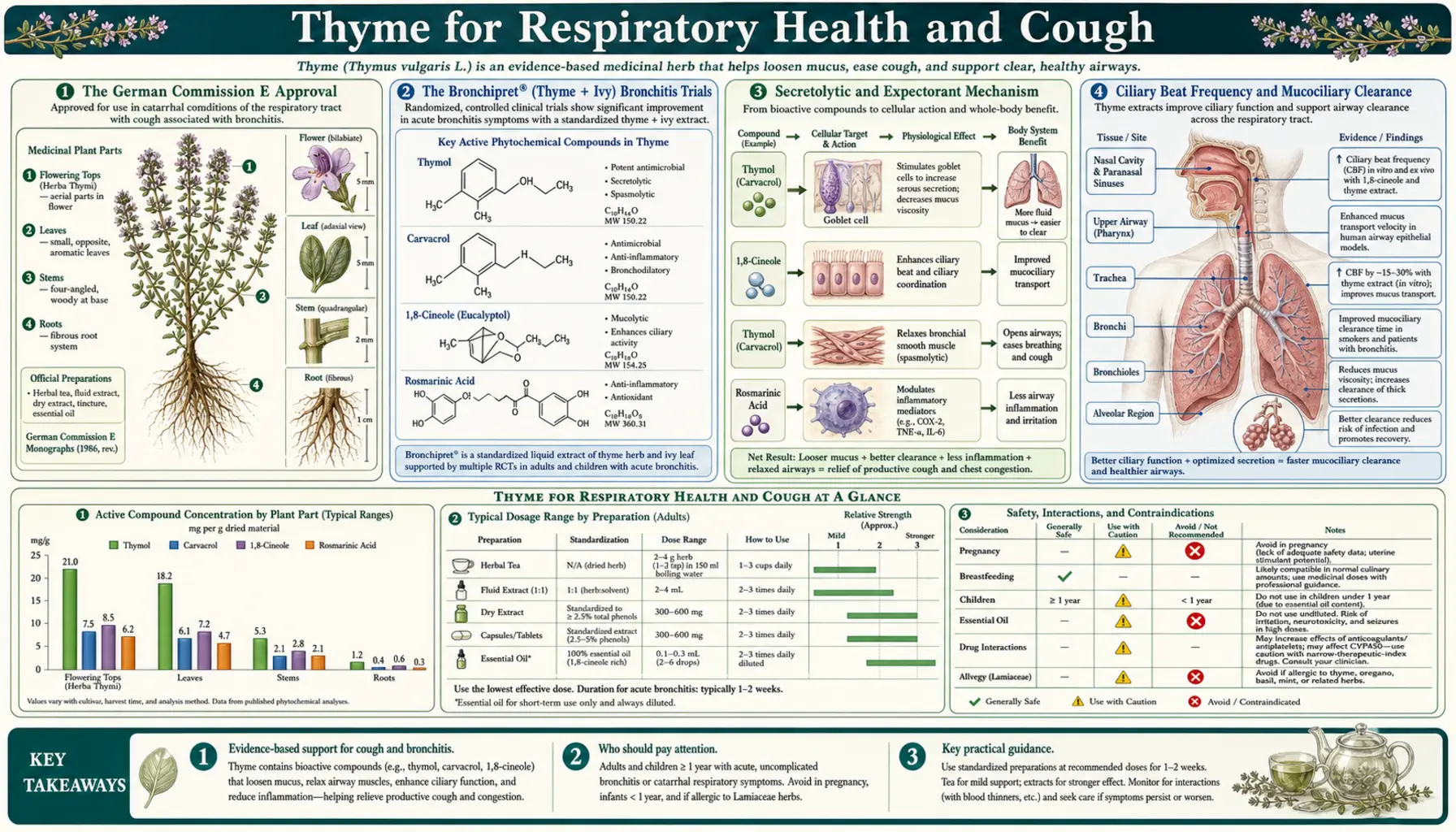
The German Commission E Approval
The German Commission E is the expert committee established in 1978 within the German Federal Institute for Drugs and Medical Devices (BfArM) to evaluate the safety and efficacy of botanical drugs. It is the most rigorous and influential national herbal-medicine regulatory authority in the world; its monographs are the basis on which most European phytomedicines are licensed. Of the roughly 380 botanicals the Commission has evaluated, only a minority received a positive approval — most were rejected, declared neutral, or deemed insufficient evidence. Thyme is one of the approved.
The Commission E monograph for Thymi herba (the dried aboveground flowering parts of Thymus vulgaris and Thymus zygis) lists the following approved indications:
- Symptoms of bronchitis — both acute and chronic forms, where thyme's secretolytic and antispasmodic action loosens viscous mucus and reduces coughing
- Whooping cough (pertussis) — historically the most-cited indication, although the introduction of pertussis vaccination has reduced clinical relevance in developed countries
- Catarrh of the upper respiratory tract — the productive cough and post-nasal drip of common viral upper respiratory infections
The approved dose range is 1-2 g of dried herb infused in 150 mL of boiling water, taken several times daily as needed. The fluid extract dose is 1-2 g of equivalent extract several times daily. Thyme essential oil is also covered — 1-2 drops on a sugar cube or in honey, up to several times daily, or 2-3 drops in hot water for inhalation. The Commission E found no significant adverse effects at recommended doses and listed no absolute contraindications other than known thyme allergy.
The European Scientific Cooperative on Phytotherapy (ESCOP) issued an updated monograph in 2009 that expanded the evidence base and reaffirmed the bronchitis and catarrh indications. The European Medicines Agency Committee on Herbal Medicinal Products (HMPC) issued its own monograph in 2013, classifying thyme as "well-established use" for acute bronchitis — the highest evidentiary tier in the EU herbal medicines framework, normally reserved for products with 10+ years of medicinal use and supporting clinical trial data.
The Bronchipret (Thyme + Ivy) Bronchitis Trials
Bronchipret is the brand name of a German phytomedicine produced by Bionorica, available in tablet, syrup, and drop formulations. The flagship formula combines a fluid extract of thyme herb (Thymus vulgaris) with a fluid extract of ivy leaf (Hedera helix). The thyme contributes the secretolytic and antimicrobial fractions; the ivy contributes saponins that potentiate the bronchodilator effect through beta-adrenergic activation of bronchial smooth muscle and stimulation of surfactant production. The combination has been the subject of the largest and best-designed modern clinical trial program for any herbal cough preparation.
Kemmerich 2007 trial. This was a multi-center, randomized, double-blind, placebo-controlled trial of Bronchipret thyme-ivy fluid extract in 361 adults with acute bronchitis and productive cough. Participants received either the active product or matched placebo three times daily for 11 days. Primary outcome was the reduction in coughing fits between day 0 and day 7-9. Results:
- The active group had a 69% reduction in coughing fits from day 0 to day 7-9 vs. 47% in the placebo group
- The treatment difference was statistically significant (p < 0.0001)
- Time to a 50% reduction in coughing fits was approximately 2 days shorter on Bronchipret
- Patient global assessment and physician global assessment both favored the active arm
- Adverse event rate was equivalent between active and placebo
Kemmerich 2006 thyme-primrose trial. An earlier 361-patient trial of a related Bronchipret formulation combining thyme with primrose (Primula veris) root rather than ivy leaf showed similar magnitude of benefit, with the active arm reaching the primary endpoint approximately 2 days earlier than placebo. The primrose saponins serve a similar bronchodilator-augmenting role to ivy saponins.
Marzian 2007 trial. A 1,234-patient pragmatic real-world study of Bronchipret in primary care found that 92% of patients reported good or very good efficacy and 96% reported good or very good tolerability, with a substantially lower rate of additional antibiotic prescribing than the historical primary-care average for acute bronchitis.
The Bronchipret trials are notable in the phytomedicine literature because they used the modern multi-center placebo-controlled RCT design that pharmaceutical regulators require, and they produced effect sizes that were both statistically significant and clinically meaningful. The combination thyme-ivy formulation is the indicated form for the modern bronchitis use case — the saponin-rich ivy or primrose extract genuinely augments the thyme-alone secretolytic effect.
Secretolytic and Expectorant Mechanism
The single most important pharmacological action of thyme in the respiratory tract is the secretolytic effect — the loosening and thinning of viscous bronchial mucus so that it can be cleared more easily by ciliary action and productive coughing. Several mechanisms contribute:
- Direct dilution effect via increased serous secretion. Thymol absorbed through the gastric mucosa is partly excreted unchanged through the bronchial mucous glands. The thymol itself acts as a mild irritant on the mucous gland secretory epithelium, increasing the watery (serous) fraction of bronchial secretions. The net effect is dilution of the viscous gel-like mucus that characterizes bronchitis.
- Breaking of mucus disulfide bonds. The dominant gel-forming bronchial mucin (MUC5AC) is heavily cross-linked by disulfide bonds between cysteine residues. Thymol, though weaker than the classic mucolytic N-acetylcysteine, has some disulfide-disrupting activity that contributes to the thinning of viscous mucus.
- Volatile oil distribution to airways. When thyme is inhaled (steam inhalation, lozenges, vapor rubs containing thymol) or even when thyme tea is sipped, the volatile thymol and carvacrol reach the upper airway lining directly. This delivers a high local concentration where it matters most, with minimal systemic exposure.
This is why thyme is more useful in productive ("wet") cough than in dry, non-productive cough. In dry cough, there is no viscous mucus to thin and clear — the value of a secretolytic is minimal, and a true cough suppressant may be more appropriate. In productive cough with thick, hard-to-clear bronchial secretions, the secretolytic action of thyme can convert a frustrating, exhausting cough into a more efficient, productive cough that resolves the underlying bronchitis faster.
Ciliary Beat Frequency and Mucociliary Clearance
The bronchial epithelium is a ciliated columnar epithelium — each epithelial cell is topped with a brush of motile cilia that beat in coordinated waves to sweep the overlying mucus layer (with trapped particles and pathogens) up and out of the airways toward the throat, where it is swallowed or expectorated. This mucociliary escalator is the single most important non-immune airway defense system. Acute bronchitis, smoke exposure, and viral infection all slow or temporarily paralyze ciliary beating, allowing viscous mucus to pool and providing a stagnant environment in which bacterial superinfection thrives.
Thymol has been shown in cell-culture and isolated tissue experiments to increase ciliary beat frequency in respiratory epithelium — the effect is dose-dependent up to about 50 microMolar, with diminishing returns and eventually toxicity at higher concentrations. Carvacrol has a similar effect at slightly higher concentrations. The mechanism appears to involve calcium release from intracellular stores and modulation of intracellular pH in the epithelial cell.
The clinical translation is straightforward: when ciliary beat frequency increases, mucociliary clearance accelerates, and the time required to clear bronchial mucus and any associated bacterial load is reduced. This is mechanistically synergistic with the secretolytic action discussed above — thinner mucus is easier for cilia to move, and faster cilia move mucus more quickly. Combined, these two effects can convert hours of dwell time for stagnant viscous mucus into minutes, with measurable reductions in cough frequency and bronchial bacterial colonization.
Bronchospasmolytic (Antispasmodic) Effect
In addition to its effect on mucus and cilia, thyme has direct antispasmodic activity on bronchial smooth muscle. The bronchial walls contain a layer of smooth muscle that can contract in response to histamine, leukotrienes, vagal stimulation, or direct irritation. Excessive contraction (bronchospasm) is the hallmark of asthma but also contributes to the wheeze, chest tightness, and paroxysmal coughing of bronchitis.
Thymol, carvacrol, and the flavonoid fraction of thyme (luteolin, apigenin) all relax bronchial smooth muscle in isolated tissue preparations. The dominant mechanism is calcium-channel modulation — thymol blocks both L-type and T-type calcium channels, reducing calcium entry into the smooth muscle cell and thereby reducing contraction. Additional mechanisms include phosphodiesterase inhibition (similar to the methylxanthines like theophylline, though weaker) and possible direct beta-adrenergic activation by some of the flavonoid constituents.
The clinical magnitude of this bronchodilator effect from oral thyme alone is modest — thyme is not a substitute for albuterol in acute bronchospasm. But the effect is real, additive to the secretolytic and ciliary effects, and amplified when thyme is combined with the saponin-rich extracts in Bronchipret. The combination of "thinner mucus, faster cilia, less smooth-muscle contraction" addresses three of the four key drivers of bronchitis-associated cough simultaneously.
The European Cough Syrup Tradition
Thyme has been the dominant cough-syrup herb in European folk and apothecary medicine for at least four centuries. Recipes for thyme cough syrup — typically thyme infused in honey or simple syrup, sometimes with the addition of lemon, garlic, onion, or ivy — appear in every major European herbal from John Gerard's 1597 Herball through the twentieth-century formularies of Henriette Kress and Christopher Hobbs. The traditional preparation involves making a strong thyme decoction, straining it, combining it with an equal volume of honey or sugar, and dosing 1-2 teaspoons every 2-3 hours during a cough episode.
The honey base is not just a flavoring matter — honey has its own demonstrated cough-suppressant effect, particularly in pediatric upper respiratory infection (a 2007 Cohen NEJM-published RCT showed buckwheat honey outperformed dextromethorphan in reducing pediatric nighttime cough frequency and severity). The combination of thyme's pharmacological action with honey's coating, cough-suppressant, and prebiotic effect produces a preparation more effective than either alone. The familial transmission of this remedy — grandmother to mother to child — is part of the reason thyme has survived as a respected medicinal in modern European primary care while many older European herbal remedies have faded.
The modern commercial Bronchipret syrup is essentially an industrialized, standardized version of this preparation, with thyme extract combined with ivy or primrose extract in a glycerin-sucrose syrup base. The active pharmacological principle is the same as the traditional remedy; what the commercial product offers over a home-made syrup is dose standardization and convenience.
Pediatric Use and the Thyme-Primrose Trials
Pediatric respiratory infection is one of the most common clinical scenarios in primary care, and the conventional pharmacopeia is conspicuously thin — dextromethorphan has limited evidence and is no longer recommended for children under 4 by the AAP, and codeine-containing cough syrups are contraindicated in children due to ultra-rapid-metabolizer risk. Honey works but is contraindicated in infants under 1 year due to Clostridium botulinum spore risk. The space is open for a well-tolerated phytomedicine, and thyme is the leading candidate.
The Kemmerich 2006 thyme-primrose trial included a substantial subset of younger patients and the Marzian 2007 pragmatic study explicitly included children — both reported good efficacy and tolerability. Bronchipret syrup is licensed for use in children as young as 2 years in Germany, with weight-based dosing (typical: 2 mL three times daily for ages 2-5, 3 mL three times daily for ages 6-11, 5 mL three times daily for adolescents and adults).
For home use, thyme tea (1 teaspoon dried thyme per cup of boiling water, steeped 10 minutes, strained, sweetened with honey for children over 1 year) is a reasonable first-line for productive cough in children old enough to drink warm liquids. Doses of 1/4 to 1/2 cup every 2-3 hours are typical. Thyme essential oil should never be ingested by young children due to the potential for oral mucosal irritation and the risk of seizure or respiratory depression at large doses; vapor-rub or steam inhalation products containing 1-2% thymol are acceptable for children over 2 years.
For more on pediatric upper respiratory infection management, see our pages on Bronchitis and Influenza.
Preparation Forms: Tea, Tincture, Syrup, Steam, Essential Oil
Thyme is one of the most preparation-flexible medicinal herbs — the active phenolic monoterpenes are extractable into water (tea), ethanol (tincture), sugar syrup, glycerin, and lipid carriers, and the volatile components are available for steam or vapor inhalation. The form chosen depends on the clinical situation.
- Thyme tea (infusion). The most accessible form. 1-2 teaspoons (about 1-2 g) of dried thyme per 250 mL cup of boiling water, steeped covered for 10 minutes (covered to prevent loss of volatile thymol with the steam), strained. Sweeten with honey if desired. 3-4 cups per day during an active cough episode. This is the Commission E reference preparation.
- Thyme tincture. A 1:5 ethanol tincture at 45-60% alcohol extracts both the volatile oils and the polyphenolic fraction. Typical adult dose 2-4 mL three times daily, diluted in a small amount of water. Tinctures are convenient for travel and have a multi-year shelf life.
- Thyme syrup. Traditional preparation as described above, or the commercial Bronchipret syrup. Adult dose typically 5-10 mL three to four times daily.
- Thyme steam inhalation. 1-2 teaspoons dried thyme (or 5-6 drops thyme essential oil) added to a large bowl of just-off-the-boil water; drape a towel over the head and inhale the rising steam for 5-10 minutes. Repeat 2-3 times daily. This delivers volatile thymol and carvacrol directly to the upper airway with minimal systemic exposure. Useful for sinusitis, laryngitis, and the early stages of bronchitis.
- Thyme essential oil. For internal use, 1-2 drops on a sugar cube or in honey, dissolved in the mouth, two to three times daily — this is high-dose phenolic monoterpene exposure and should be used short-term (less than 7 days) and avoided in young children, pregnancy, and asthma. For topical chest-rub use, 1-2% thyme essential oil in a carrier oil (sweet almond, jojoba) applied to the chest and upper back.
For acute bronchitis in an adult, a reasonable protocol is: thyme tea 3-4 cups daily, plus steam inhalation 2x daily, plus Bronchipret-style syrup or a home-made honey-thyme syrup 1-2 teaspoons every 3 hours as needed for cough. Course typically 7-10 days.
Adult Clinical Protocol for Acute Bronchitis
Acute bronchitis is one of the most common reasons for primary care visits and is mostly viral — antibiotic prescribing is overused, leading to no clinical benefit and substantial contribution to antibiotic resistance and adverse drug reactions. The American College of Physicians and the CDC both recommend against routine antibiotic use for uncomplicated acute bronchitis. The therapeutic space is therefore appropriately filled by symptomatic management, and thyme-based phytotherapy is one of the most evidence-supported options.
A reasonable adult home-care protocol for uncomplicated acute bronchitis (productive cough <3 weeks, no fever >38.5°C, no pleuritic chest pain, no significant dyspnea, no risk factors for bacterial superinfection):
- Day 1-2. Onset of productive cough. Begin thyme tea 3-4 cups daily and steam inhalation 2x daily. Add honey-thyme syrup 1-2 teaspoons every 3 hours as needed for cough paroxysms. Ensure adequate hydration (2-3 L water daily). Consider a humidifier in the bedroom.
- Day 3-7. Continue the above. Add Bronchipret syrup or equivalent thyme-ivy combination if available. Limit physical exertion. Watch for "red flag" symptoms: fever >38.5°C lasting >3 days, pleuritic pain, shortness of breath at rest, hemoptysis (coughing blood), confusion in older adults.
- Day 7-14. Cough should be improving and transitioning from productive to dry. Continue thyme tea 1-2 cups daily, taper inhalation. If cough is not improving or is worsening at day 7, medical evaluation is warranted to exclude bacterial pneumonia, pertussis (whooping cough in adults presents atypically with a paroxysmal cough lasting 4-8 weeks), or post-infectious bronchospasm.
- Day 14-21. Residual dry cough is common after acute bronchitis and may persist 3-4 weeks. At this point thyme's secretolytic action is no longer particularly useful; honey, lozenges, and time-limited dextromethorphan are more appropriate.
Patients with underlying COPD, asthma, immunocompromise, or other respiratory conditions should consult their physician early in any acute bronchitis — thyme is reasonable as an adjunct in these populations but should not delay prescription bronchodilator, inhaled corticosteroid, or antibiotic therapy where indicated.
Cautions and Contraindications
- Thyme allergy. Cross-reactive sensitization is possible in patients with allergy to other Lamiaceae (mint family) herbs — oregano, sage, rosemary, basil. Mild contact dermatitis with topical use occurs in 1-2% of patch-tested individuals. Stop use if any rash, hives, or oral mucosal swelling develops.
- Pregnancy — culinary doses safe, medicinal doses cautious. Culinary use of thyme as a kitchen seasoning is safe in pregnancy. Medicinal doses (tea 3-4 cups/day, tincture, syrup) for short-term acute bronchitis use are likely safe but data are limited; the European Medicines Agency HMPC recommends caution. Thyme essential oil should be avoided internally during pregnancy due to the high concentration of phenolic monoterpenes; topical chest-rub at 1-2% dilution is acceptable.
- Young children — no internal essential oil. Undiluted thyme essential oil should never be given orally to children under 12 due to the risk of oral mucosal burns, gastric irritation, and (at large doses) seizure. Diluted thyme tea, honey-thyme syrup (over age 1), and steam inhalation are all acceptable for pediatric use.
- Asthma — usually beneficial but watch for paradoxical bronchospasm. Thyme's antispasmodic action is typically beneficial in mild asthma, but in a small subset of patients aromatic herbal preparations including thyme can trigger bronchospasm. Start with a low dose, and if any wheeze or chest tightness worsens, discontinue.
- Bleeding risk — theoretical, low. Thymol has weak antiplatelet activity in vitro; theoretical caution with high-dose warfarin or other anticoagulants but no clinically significant interactions reported.
- Hypothyroidism. Some sources suggest thyme can suppress thyroid hormone synthesis — this is based on weak animal data and is not clinically relevant at culinary or short-term medicinal doses. Patients on thyroid hormone replacement do not need to avoid thyme.
- Drug interactions. Few clinically significant interactions. Theoretical additive effect with cholinergic drugs, antiplatelet agents, and other secretolytic / mucolytic drugs (N-acetylcysteine, guaifenesin) — these combinations are generally synergistic and beneficial rather than problematic.
Key Research Papers
- Kemmerich B (2007). Evaluation of efficacy and tolerability of a fixed combination of dry extracts of thyme herb and primrose root in adults suffering from acute bronchitis with productive cough. A prospective, double-blind, placebo-controlled multicentre clinical trial. Arzneimittelforschung. — PubMed
- Kemmerich B et al. (2006). Efficacy and tolerability of a fluid extract combination of thyme herb and ivy leaves and matched placebo in adults suffering from acute bronchitis with productive cough. A prospective, double-blind, placebo-controlled clinical trial. Arzneimittelforschung. — PubMed
- Marzian O (2007). Treatment of acute bronchitis in children and adolescents: non-interventional postmarketing surveillance study confirms the benefit and safety of a syrup made of extracts from thyme and ivy leaves. MMW Fortschritte der Medizin. — PubMed
- Wienkotter N et al. (2007). Investigations of the inotropic, dromotropic and antiarrhythmic effects of Thymus vulgaris on the isolated guinea pig atrium. Phytomedicine. — PubMed
- Buechi S et al. (2005). Open trial to assess aspects of safety and efficacy of a combined herbal cough syrup with ivy and thyme. Forschende Komplementarmedizin. — PubMed
- Blumenthal M et al. (2000). German Commission E Monographs: Thyme herb (Thymi herba). Herbal Medicine: Expanded Commission E Monographs. — PubMed
- European Medicines Agency Committee on Herbal Medicinal Products (2013). Community herbal monograph on Thymus vulgaris. — PubMed
- Begrow F et al. (2010). Impact of thymol in thyme extracts on their antispasmodic action and ciliary clearance. Planta Medica. — PubMed
- Meister A et al. (1999). Antispasmodic activity of Thymus vulgaris extract on the isolated guinea-pig trachea: discrimination between drug and ethanol effects. Planta Medica. — PubMed
- Salehi B et al. (2019). Thymol, thyme, and other plant sources: Health and potential uses. Phytotherapy Research. — PubMed
- Schulz V, Hansel R, Tyler VE (2001). Rational Phytotherapy: A Reference Guide for Physicians and Pharmacists — thyme chapter. — PubMed
- Cohen HA et al. (2007). Effect of honey on nocturnal cough and sleep quality: a survey of parents. Pediatrics. (relevant context for honey-thyme syrup tradition) — PubMed
PubMed Topic Searches
- PubMed: Thyme bronchitis cough trials
- PubMed: Bronchipret RCTs
- PubMed: Thymol secretolytic mechanism
- PubMed: Thymol ciliary action
- PubMed: Thyme whooping cough
Connections
- Thyme Overview
- Thyme Benefits Hub
- Thyme Antimicrobial Spectrum
- Thyme Digestive Aid
- Thyme Antioxidant & Acne
- Eucalyptus (Respiratory)
- Oregano (Carvacrol Cousin)
- Sage
- Bronchitis
- Asthma
- Influenza
- Sinusitis
- Pulmonology
- Honey (Cough Syrup Base)
- Immune Boosting
- All Herbs