Saw Palmetto — Benefits Deep Dive
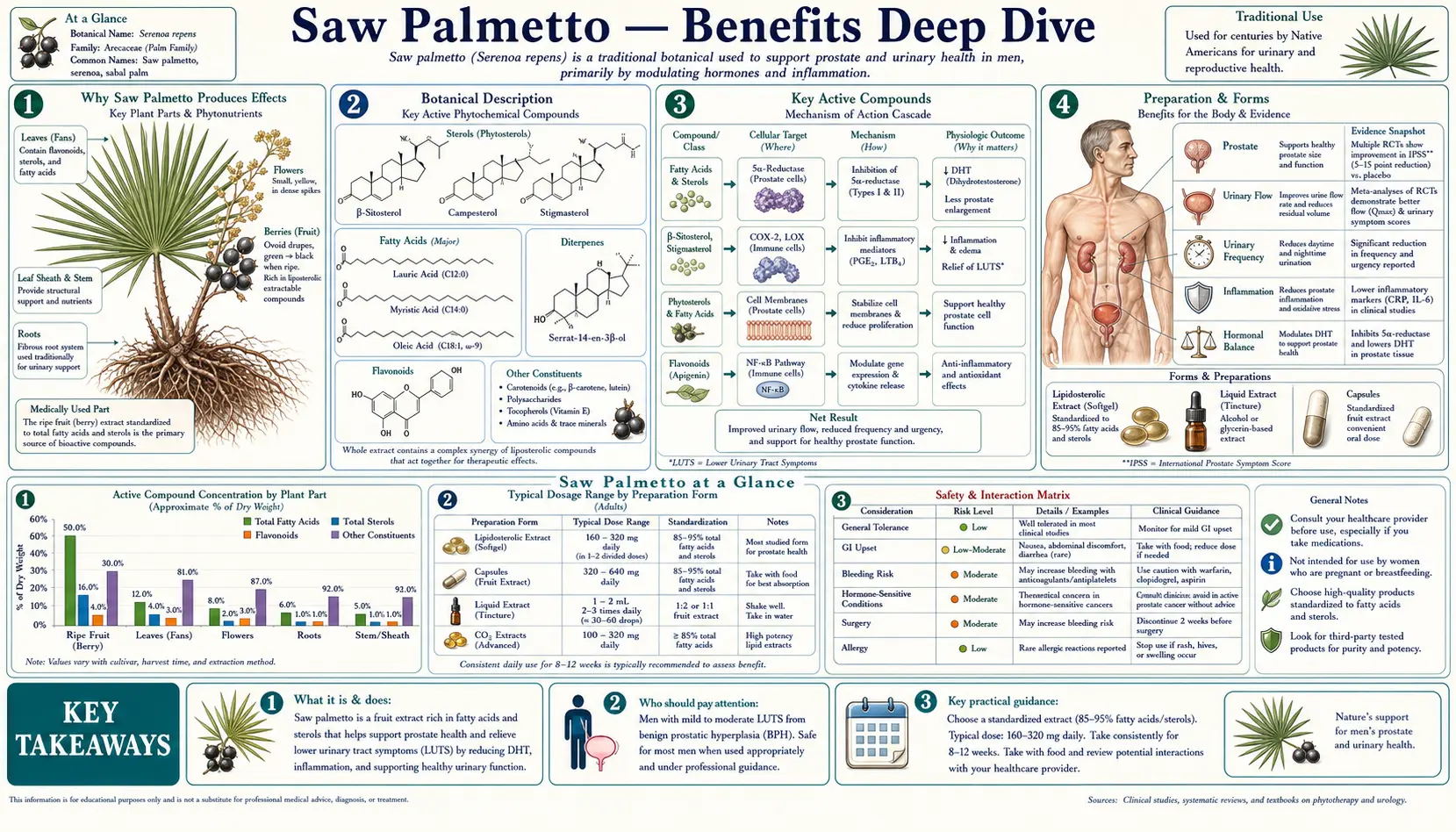
Saw palmetto (Serenoa repens) is a small fan-palm native to the southeastern United States whose ripe black berries have been used since pre-Columbian times by the indigenous Seminole and other Florida tribes for genitourinary complaints. It became the single most-popular men's herbal supplement in the West, driven by a wave of strongly positive 1990s-2000s European trials of the standardized liposterolic extract for benign prostatic hyperplasia (BPH). The therapeutically interesting fraction is roughly 85% free fatty acids (oleic, lauric, myristic, palmitic), plus 0.2-0.5% phytosterols (beta-sitosterol, campesterol, stigmasterol) and flavonoids. The mechanistic story is multi-pronged — non-competitive 5-alpha-reductase inhibition, alpha-1 adrenergic receptor blockade, anti-inflammatory COX/LOX modulation, and anti-edematous and pro-apoptotic effects in prostatic tissue. The clinical story is genuinely mixed and requires honest framing: the Wilt 1998 Cochrane meta-analysis (18 trials, 2,939 men) reported symptom improvements roughly comparable to finasteride with fewer sexual side effects, but the two methodologically rigorous American confirmatory trials — STEP (Bent 2006, NEJM) and CAMUS (Barry 2011, JAMA) — both found no difference from placebo, even at triple-dose. The reconciliation likely lies in extract quality (Permixon, the European liposterolic preparation, differs chemically from many generic U.S. extracts) and patient selection. The four pages below walk through the BPH evidence honestly, the androgenetic-alopecia hair-loss story (Prager 2002, plus DHT-blocking mechanism), urinary-function effects beyond BPH (overactive bladder, post-prostatectomy nocturia), and the hormonal and safety profile including the surprisingly good tolerability versus finasteride.
Deep-Dive Articles
Prostate Health & BPH
The most-studied and most-debated herb for benign prostatic hyperplasia. Wilt's 1998 Cochrane meta-analysis (18 trials, 2,939 men) reported nocturia and peak-flow improvements comparable to finasteride; the rigorous American STEP (NEJM 2006) and CAMUS (JAMA 2011) confirmatory RCTs both found no difference from placebo. Triple mechanism — 5-alpha-reductase inhibition (both type I and II isoforms), alpha-1 adrenergic blockade, anti-inflammatory and anti-edematous effects. The Permixon vs generic extract quality issue may explain the trans-Atlantic results split.
Hair Loss (Androgenetic Alopecia)
The DHT-blocking mechanism shared with finasteride applied to the scalp follicle. The Prager 2002 small RCT (n=34) showed roughly 60% of saw palmetto users had improvement in male-pattern hair loss versus 11% placebo. Subsequent open-label data and head-to-head comparisons against finasteride and minoxidil. Topical vs oral formulations, realistic effect-size expectations, and why this is a 6-12 month commitment, not a quick fix.
Urinary Function
Beyond BPH per se — overactive bladder pilot data, frequency and urgency reduction, nocturia improvement mechanisms, and the emerging post-prostatectomy use for residual urinary symptoms. How the alpha-1 adrenergic effect on bladder neck and prostatic urethra smooth muscle complements the anti-androgen mechanism, and why some patients with mild lower urinary tract symptoms (LUTS) respond even when their PSA-driven prostate volume reduction is modest.
Hormonal Effects & Cautions
The 5-alpha-reductase inhibition makes saw palmetto theoretically an anti-androgen — relevant for women with PCOS, hirsutism, and acne, where small uncontrolled series suggest benefit. Critically, unlike finasteride, saw palmetto has not been associated with persistent post-finasteride syndrome, gynecomastia, or measurable systemic feminizing effects in controlled trials. Surgery: discontinue 2 weeks pre-operatively for theoretical antiplatelet effect. Pregnancy contraindication. Anticoagulant interaction.
Table of Contents
- Deep-Dive Articles
- Why Saw Palmetto Produces Effects
- Key Research Papers
- External Authoritative Resources
- Connections
- Featured Videos
Why Saw Palmetto Produces Effects
Most plant medicines acting on the prostate work through a single dominant mechanism. Saw palmetto is unusual in that the standardized liposterolic extract has been shown in cell-culture, animal, and tissue-biopsy work to act through at least five distinct mechanisms simultaneously, each one independently modest in effect size but collectively additive on the diseased prostatic and follicular tissue. Understanding why the multi-mechanism profile matters helps explain both the herb's clinical utility and the heterogeneous trial results.
- 5-alpha-reductase inhibition — the liposterolic extract non-competitively inhibits both type I (skin, scalp, sebaceous gland) and type II (prostate, hair follicle) isoforms of 5-alpha-reductase, the enzyme that converts testosterone to the more potent androgen dihydrotestosterone (DHT). The inhibition is partial and dose-dependent, far weaker than finasteride (which reduces serum DHT by ~70%) or dutasteride (~95%), but it does measurably reduce intra-prostatic DHT in tissue biopsy studies (Marks 2001) without producing the large systemic DHT drop that drives finasteride's sexual side effects.
- Alpha-1 adrenergic receptor blockade — the same fatty acid fraction has been shown to antagonize alpha-1 adrenergic receptors in the bladder neck and prostatic urethra smooth muscle. This is the same mechanism by which prescription drugs tamsulosin (Flomax) and alfuzosin work, providing immediate symptomatic relief of obstructive urinary symptoms while the slower anti-androgen mechanism reduces prostate volume.
- Anti-inflammatory COX and LOX modulation — saw palmetto fatty acids inhibit both cyclooxygenase (COX, prostaglandin synthesis) and 5-lipoxygenase (5-LOX, leukotriene synthesis) in prostatic tissue. Histologic studies of BPH have established that chronic prostatic inflammation contributes to symptom severity independently of prostate volume, and reducing prostaglandin/leukotriene burden plausibly reduces irritative urinary symptoms (urgency, frequency, dysuria).
- Anti-edematous effects — both clinical observation and ultrasound studies suggest saw palmetto reduces prostatic tissue edema. The mechanism is incompletely understood but may relate to the COX/LOX inhibition (reducing inflammatory exudate) and to a direct effect on prostatic capillary permeability. The clinical correlate is the often-reported subjective sense of "decompression" within days of starting treatment, well before any measurable prostate-volume change.
- Pro-apoptotic effects on prostatic epithelium — in vitro work has shown saw palmetto extract induces apoptosis in cultured prostatic epithelial cells and modulates expression of Bcl-2 family proteins. This mechanism is more theoretical than clinically established but could contribute to the modest prostate-volume reductions seen in some long-term trials.
The catch is that none of these mechanisms is strong on its own. Finasteride is a far more potent 5-alpha-reductase inhibitor; tamsulosin is a far more selective alpha-1 antagonist; ibuprofen is a stronger COX inhibitor. The therapeutic logic for saw palmetto, when it works, is that partial action across all five pathways in the same patient produces an effect roughly comparable to full action on any single pathway via a prescription drug — with a dramatically better tolerability profile because no single pathway is being fully suppressed.
This logic also explains the mixed trial results. Patients whose BPH is driven primarily by tissue inflammation or smooth-muscle tone may respond robustly to saw palmetto. Patients whose BPH is driven primarily by large prostate volume and severe DHT-mediated hyperplasia probably need full-dose finasteride or dutasteride and will perceive saw palmetto as ineffective. The two American confirmatory trials (STEP, CAMUS) enrolled patients with moderate-to-severe symptoms and likely overrepresented the latter group; the European Permixon trials enrolled patients earlier in the disease course and likely captured more of the former. The honest take is that saw palmetto is a reasonable first-line trial for early BPH or for patients who cannot tolerate finasteride's side effects, with the explicit understanding that 30-50% of users will perceive no benefit and should escalate to prescription therapy.
Key Research Papers
- Wilt TJ et al. (1998). Saw palmetto extracts for treatment of benign prostatic hyperplasia: a systematic review. JAMA. — PubMed
- Bent S et al. (2006). Saw palmetto for benign prostatic hyperplasia. STEP trial. NEJM. — PubMed
- Barry MJ et al. (2011). Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms (CAMUS trial). JAMA. — PubMed
- Marks LS et al. (2001). Effects of a saw palmetto herbal blend in men with symptomatic benign prostatic hyperplasia (tissue biopsy intra-prostatic DHT). Journal of Urology. — PubMed
- Prager N et al. (2002). A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. Journal of Alternative and Complementary Medicine. — PubMed
External Authoritative Resources
- NCCIH — Saw Palmetto — the U.S. National Center for Complementary and Integrative Health summary
- NIH Office of Dietary Supplements — Botanical and Dietary Supplement Fact Sheets
- MedlinePlus — Saw Palmetto (drug interactions, dose, evidence ratings)
- Cochrane Database — Serenoa repens for benign prostatic hyperplasia (Tacklind 2012 update)
- PubMed — All research on Serenoa repens / saw palmetto (~2,000+ papers)
Connections
- Saw Palmetto (Main Page)
- Saw Palmetto for Prostate Health & BPH
- Saw Palmetto for Hair Loss
- Saw Palmetto for Urinary Function
- Hormonal Effects & Cautions
- Benign Prostatic Hyperplasia (BPH)
- Prostate Conditions
- Erectile Dysfunction
- Low Testosterone & TRT
- Polycystic Ovary Syndrome (PCOS)
- Alopecia (Hair Loss)
- Hair Loss
- PSA Test
- Testosterone Test
- Hormone Panel
- Zinc
- All Herbs