Saw Palmetto for Urinary Function
Saw palmetto's urinary effects extend beyond the canonical benign prostatic hyperplasia (BPH) indication into several adjacent areas where the herb has accumulated meaningful clinical experience and small-trial data: overactive bladder syndrome (OAB), post-prostatectomy urinary symptoms, nocturia from mixed mechanisms, lower urinary tract symptoms (LUTS) in women with bladder dysfunction, and chronic prostatitis / chronic pelvic pain syndrome (CP/CPPS). The mechanistic basis is the same triple action that drives the BPH effect — partial alpha-1 adrenergic blockade reduces bladder neck smooth muscle tone, anti-inflammatory action reduces detrusor irritation, and the slower 5-alpha-reductase mechanism contributes through the prostatic urethra and detrusor androgen-receptor pathways. This page covers each of these adjacent urinary applications honestly, with the same emphasis on realistic effect size and patient selection that the BPH page applies, recognizing that several of these indications have far thinner published evidence than the BPH core indication.
Table of Contents
- The Multi-Mechanism Urinary Effect
- Nocturia Improvement Mechanism
- Overactive Bladder (OAB) Pilot Data
- Frequency and Urgency Reduction
- Post-Prostatectomy Use
- Chronic Prostatitis / CPPS
- Female Lower Urinary Tract Symptoms
- Combination with Anticholinergics and Beta-3 Agonists
- Why Workup Matters Before Empiric Therapy
- Practical Patient Guidance
- Key Research Papers
- Connections
- Featured Videos
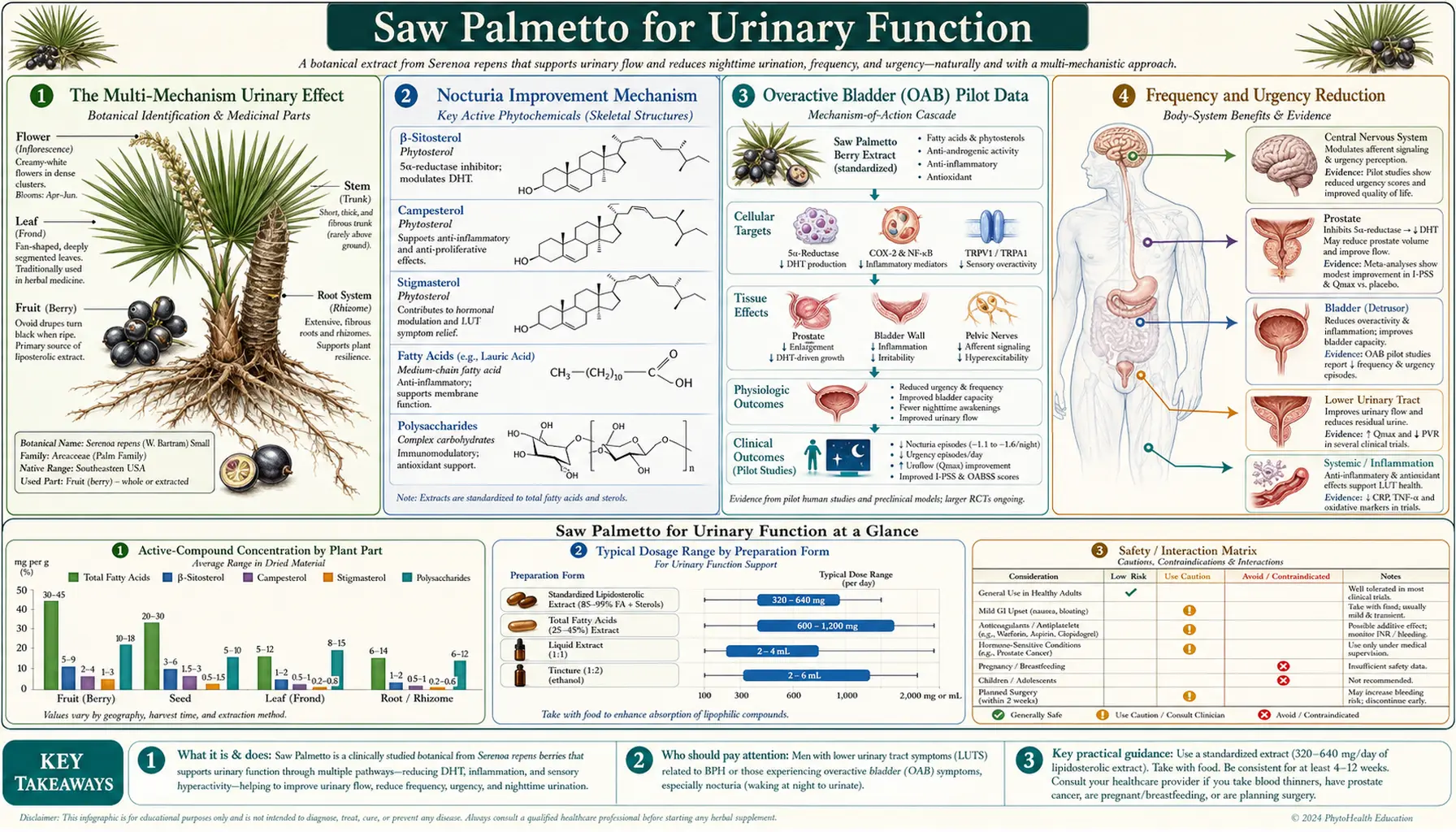
The Multi-Mechanism Urinary Effect
The lower urinary tract is composed of the bladder (smooth-muscle detrusor body, internal urethral sphincter), the prostate (in men, surrounding the prostatic urethra), the bladder neck (densely innervated by alpha-1 receptors), and the external striated sphincter (under voluntary control). Symptomatic urinary dysfunction in older men typically reflects a mix of contributions: prostate volume causing mechanical obstruction, alpha-1 mediated smooth muscle tone causing functional obstruction, detrusor overactivity causing urgency and frequency, detrusor underactivity causing incomplete emptying, and the central nervous system contribution from impaired bladder filling sensation in aging.
Saw palmetto's actions touch several of these components:
- Bladder neck and prostatic urethra alpha-1 antagonism — partial blockade of alpha-1 adrenergic receptors reduces smooth-muscle tone in the dynamic outflow component. The effect is weaker than tamsulosin or alfuzosin but acts at the same anatomic target.
- Prostatic anti-inflammatory effects — COX/LOX inhibition in inflamed prostatic tissue reduces irritative symptoms that arise from chronic prostatic inflammation (a contributor to LUTS independent of prostate volume).
- Detrusor effects (indirect) — chronic outflow obstruction produces secondary detrusor hypertrophy and instability. Reducing the outflow obstruction with saw palmetto's combined alpha-1 and anti-androgen effects may produce secondary improvement in detrusor function over months.
- Anti-edematous effects on bladder/prostate tissues — the empirical observation of rapid subjective "decompression" within days of starting saw palmetto suggests an immediate anti-edematous mechanism that improves outflow before any anti-androgen volume change could occur.
The net urinary effect in responders is improvement in both obstructive symptoms (weak stream, hesitancy, incomplete emptying) and irritative symptoms (frequency, urgency, nocturia). The relative balance of these two improvements varies by patient phenotype.
Nocturia Improvement Mechanism
Nocturia — awakening at night to urinate — is the symptom most consistently improved by saw palmetto across the published trial literature. The Wilt 1998 Cochrane meta-analysis found an average reduction of 0.76 nocturia episodes per night across pooled trials, a clinically meaningful change for patients whose sleep quality was the dominant motivation for seeking treatment.
Nocturia has multiple causes that contribute independently and additively:
- Reduced functional bladder capacity — either from detrusor overactivity (urgency at low fill volumes) or from poor emptying with elevated post-void residual. Saw palmetto's outflow effects modestly improve emptying, which over months reduces the residual urine that effectively shrinks functional capacity.
- Increased nocturnal urine production (nocturnal polyuria) — age-related loss of the circadian arginine vasopressin rhythm, which normally concentrates urine at night. Saw palmetto does not address this directly, so patients whose nocturia is primarily from nocturnal polyuria respond less well.
- Increased global urine production (24-hour polyuria) — from diabetes mellitus, diabetes insipidus, hypercalcemia, lithium, or excessive fluid intake. These require diagnostic workup and addressing the underlying cause.
- Sleep disorders — obstructive sleep apnea is a major cause of nocturia in older men. The mechanism is fragmented sleep producing increased awareness of bladder filling and apnea-driven atrial natriuretic peptide release driving nocturnal urine production. Treating the OSA often resolves the nocturia.
The implication: when saw palmetto reduces nocturia, the reduction is mediated primarily by improvement in functional bladder capacity through the outflow mechanisms. Patients whose nocturia is dominated by nocturnal polyuria or sleep apnea respond less well, which is why the workup of nocturia should distinguish causes before assuming a prostatic mechanism. A simple 24-hour voiding diary (recording time and volume of every void) reliably distinguishes the dominant mechanism and should always precede empiric saw palmetto therapy for nocturia.
Overactive Bladder (OAB) Pilot Data
Overactive bladder syndrome is characterized by urgency, with or without urge incontinence, usually accompanied by frequency and nocturia, in the absence of urinary tract infection or other obvious pathology. OAB affects approximately 16% of adults over age 40, with prevalence rising with age. The standard pharmacotherapy is anticholinergics (oxybutynin, tolterodine, solifenacin, darifenacin) or the beta-3 adrenergic agonist mirabegron, both of which suppress detrusor overactivity.
Saw palmetto for OAB is an investigational use with limited published evidence. The mechanistic logic is twofold: first, the alpha-1 antagonism may reduce bladder neck reflex stimulation of the detrusor; second, the anti-inflammatory mechanism may reduce neurogenic detrusor irritation arising from prostatic inflammation in men with both BPH and OAB symptoms.
Several small pilot studies have addressed this question:
- Wei 2018 reported improvement in OAB symptoms in 60% of men with mixed BPH and OAB treated with saw palmetto extract over 12 weeks, with reductions in frequency and urgency episodes per day.
- Lao 2007 reported small improvements in pediatric voiding dysfunction symptoms with saw palmetto, though the small sample size and heterogeneous population limit generalizability.
- Combination saw palmetto + anticholinergic therapy has been reported in observational case series as producing additive symptom relief without prohibitive side effects.
The honest summary: saw palmetto for isolated OAB (without coexisting BPH) is poorly studied and should not be used as first-line therapy. For men with combined BPH and OAB symptoms — a very common combination — saw palmetto may produce useful symptom relief and is a reasonable addition to anticholinergic or mirabegron therapy when the BPH component contributes meaningfully to the irritative symptoms.
Frequency and Urgency Reduction
Frequency (more than 8 voids per 24 hours) and urgency (a strong sudden need to void with inability to defer) are the irritative LUTS most consistently improved across saw palmetto trials. Mechanism: the combination of anti-inflammatory action in the prostatic tissue (reducing the neurogenic detrusor irritation that arises from inflamed prostatic afferents) and partial alpha-1 antagonism in the bladder neck.
The Vinarov 2019 Permixon multicenter trial reported significant reductions in frequency and urgency scores at 12 months versus baseline. The effect size was modest (approximately 30% reduction in irritative IPSS subscore) but clinically meaningful for patients whose urgency had become a quality-of-life issue. The Suter 2013 trial similarly reported improvements in urgency episodes and frequency in men with combined BPH and irritative symptoms.
Patients should expect:
- Frequency improvement over the first 4-8 weeks — voids per day declining from approximately 10-12 toward 7-9
- Urgency episodes declining gradually over 8-12 weeks — the strong "need to go right now" sensation becomes less intense and more deferrable
- Concurrent reduction in nocturia (often the first improvement noticed because of its sleep-disruption impact)
- Less reliable improvement in urge incontinence, which usually requires anticholinergic or behavioral therapy
Post-Prostatectomy Use
Patients who have undergone radical prostatectomy for prostate cancer often have persistent or new lower urinary tract symptoms even after the prostate has been completely removed. The mechanisms are different from BPH but partially overlap:
- Anastomotic stricture or bladder neck contracture — mechanical obstruction at the surgical anastomosis
- Detrusor overactivity — from radiation or surgical bladder denervation
- Sphincter weakness causing stress incontinence — from surgical disruption of the external sphincter
- Pelvic floor dysfunction — from neuromuscular reorganization after surgery
- Persistent post-prostatectomy nocturia — one of the most common complaints, often multifactorial
Saw palmetto's post-prostatectomy use is poorly studied but has accumulated practitioner experience. The mechanistic logic that remains relevant after prostate removal: alpha-1 antagonism at the bladder neck (which remains innervated), anti-inflammatory effects on the urinary tract, and the anti-edematous mechanism that may help in the post-surgical inflammatory recovery period.
The 5-alpha-reductase mechanism becomes essentially irrelevant after radical prostatectomy because the target tissue (prostate) has been removed. Hair loss patients on saw palmetto who undergo prostatectomy can continue the medication without modification because the scalp 5-AR target remains.
For nocturia and irritative symptoms after prostatectomy, saw palmetto can be tried as a low-risk adjunct to standard post-prostatectomy management (pelvic floor physical therapy, behavioral retraining, anticholinergics for detrusor overactivity, possibly alpha-blockers for bladder neck contracture). It is not a substitute for urologic workup of new or worsening post-surgical symptoms, which should always be evaluated for treatable mechanical causes first.
Chronic Prostatitis / CPPS
Chronic prostatitis / chronic pelvic pain syndrome (CP/CPPS, NIH category III) is a heterogeneous condition characterized by pelvic pain and urinary symptoms in the absence of demonstrable bacterial infection. It accounts for approximately 90% of all chronic prostatitis presentations and is one of the most difficult urologic syndromes to treat reliably. The NIH-Chronic Prostatitis Symptom Index (NIH-CPSI) is the standard severity instrument.
Saw palmetto's anti-inflammatory mechanism makes it theoretically appealing for CP/CPPS. Several small trials have explored this:
- Kaplan 2004 randomized 64 men with CP/CPPS to saw palmetto or finasteride for 1 year; finasteride produced significant NIH-CPSI improvement while saw palmetto did not.
- Reissigl 2004 reported saw palmetto improvement in CP/CPPS in an open-label observational cohort.
- Several combination products pairing saw palmetto with other anti-inflammatory phytotherapies (quercetin, pollen extract, palmitoylethanolamide) have shown modest benefit in CP/CPPS pilot trials.
The honest summary: saw palmetto monotherapy for CP/CPPS has not shown clear benefit in the limited published trials. It may have a role as part of a multi-modal regimen that also addresses pelvic floor dysfunction (physical therapy), inflammation (NSAIDs, pollen extract), neurogenic pain (tricyclic antidepressants, gabapentinoids), and psychological factors (cognitive behavioral therapy). CP/CPPS is a syndrome where empiric single-agent herbal therapy is unlikely to produce dramatic results, and patients are better served by referral to a urology practice with experience in this difficult condition.
Female Lower Urinary Tract Symptoms
Saw palmetto in women is most familiar in the contexts of androgenetic hair loss, PCOS, and hirsutism (see the Hormonal Effects & Cautions page). Its use for female LUTS is less common but has been explored for several specific indications:
- Overactive bladder in postmenopausal women — the alpha-1 antagonism and anti-inflammatory effects could theoretically reduce detrusor irritation. Small open-label observational data suggest modest benefit; controlled trials are lacking.
- Recurrent urinary tract infection prevention — some practitioners use saw palmetto adjunctively in women with recurrent UTI, on the rationale that urinary stasis from poor emptying may contribute. The evidence is anecdotal.
- Interstitial cystitis / bladder pain syndrome — the anti-inflammatory mechanism is theoretically relevant but there are no published trials. Several combination phytotherapy products marketed for IC contain saw palmetto.
For women, the relevant cautions are the theoretical anti-androgen mechanism (which is the basis for saw palmetto's use in PCOS and hirsutism but could theoretically affect other androgen-dependent processes) and the absence of safety data in pregnancy and lactation. Premenopausal women considering saw palmetto for any indication should consult their physician, particularly regarding interactions with hormonal contraception.
Combination with Anticholinergics and Beta-3 Agonists
Patients with combined BPH and overactive bladder — a common combination, sometimes called "mixed LUTS" — often need combination therapy. Saw palmetto can be combined with:
- Anticholinergics (oxybutynin, tolterodine, solifenacin, darifenacin, fesoterodine, trospium) — these suppress detrusor overactivity through muscarinic receptor blockade. Combining with saw palmetto addresses both the bladder (urgency, frequency) and the prostate/outflow (weak stream, hesitancy) sides of mixed LUTS. The combination is generally well tolerated. Watch for additive dry mouth, constipation, and (in older patients) cognitive effects from the anticholinergic component. Anticholinergic burden is now a recognized risk factor for dementia in older adults; this should be weighed against benefit.
- Mirabegron or vibegron (beta-3 adrenergic agonists) — these suppress detrusor overactivity through a non-anticholinergic mechanism, avoiding the cognitive concerns. Combining with saw palmetto provides bladder + outflow coverage with a cleaner side effect profile, particularly for older patients. Cost is higher than anticholinergics.
- Tamsulosin or other alpha-blockers — combining saw palmetto with a prescription alpha-blocker is mechanistically redundant on the alpha-1 axis but adds the 5-AR and anti-inflammatory components. The combination is generally well tolerated but can produce additive orthostatic hypotension — monitor blood pressure, especially during the first 2-4 weeks.
Combination therapy should be approached with the same patient selection logic as monotherapy: confirm the diagnosis, identify the dominant symptom mechanism, choose agents that target that mechanism, and use the minimum effective doses to minimize cumulative side effect burden.
Why Workup Matters Before Empiric Therapy
The most consequential mistake patients make with saw palmetto for urinary symptoms is empiric self-treatment without ruling out treatable underlying causes. The differential diagnosis of LUTS in older men includes several conditions that demand specific therapy:
- Prostate cancer — can present with LUTS identical to BPH. A baseline PSA and digital rectal exam should be performed before empiric BPH therapy. Saw palmetto produces minimal PSA effect (unlike finasteride which halves PSA), so PSA screening remains interpretable on saw palmetto.
- Urinary tract infection — can produce acute LUTS that resolve with appropriate antibiotic therapy. A urinalysis and urine culture should be done if symptoms are new or worsening, particularly with dysuria or hematuria.
- Bladder cancer — can produce irritative LUTS, particularly with microhematuria. Any hematuria warrants imaging (CT urogram) and cystoscopy regardless of urinary symptoms.
- Urethral stricture — from prior infection, trauma, or instrumentation. Produces obstructive symptoms not responsive to medical therapy.
- Neurogenic bladder — from spinal cord pathology, diabetes, or multiple sclerosis. Requires urodynamic evaluation for proper management.
- Bladder stones — can produce intermittent obstruction and irritative symptoms. Diagnosed by imaging.
- Acute urinary retention — a urologic emergency requiring catheterization, not waiting for herbal therapy to take effect.
The recommended approach: any man over 50 with new or worsening urinary symptoms should have at minimum a directed history, IPSS or AUASI scoring, digital rectal exam, urinalysis, PSA, and a measurement of post-void residual urine (bladder scan or in-office ultrasound) before empiric medical therapy. This brief workup distinguishes BPH from competing diagnoses in the great majority of cases and provides the baseline values needed to track response to therapy.
Practical Patient Guidance
Putting the urinary-function evidence together into practical patient guidance:
- Nocturia as dominant symptom — first do a 24-hour voiding diary to distinguish nocturnal polyuria from reduced functional capacity. If reduced capacity (most nocturia volume in daytime range, urgency-driven nighttime voiding), saw palmetto is a reasonable trial. If nocturnal polyuria (large nighttime urine volume), saw palmetto is unlikely to help and the workup should look for sleep apnea, leg edema, peripheral venous insufficiency, late-day diuretic dosing, or cardiac dysfunction.
- Urgency and frequency as dominant symptoms — saw palmetto can be tried, alone or with mirabegron or an anticholinergic. Reasonable 8-12 week trial with reassessment.
- Obstructive symptoms (weak stream, hesitancy) as dominant — saw palmetto for mild cases; tamsulosin or alfuzosin for moderate-to-severe cases; combination of alpha-blocker and finasteride/dutasteride for advanced cases or large prostate volume.
- Mixed LUTS with both obstructive and irritative components — combination therapy from the start. Saw palmetto + anticholinergic or mirabegron is reasonable as a low-risk first combination.
- Post-prostatectomy symptoms — urologic evaluation first to rule out treatable mechanical causes (stricture, contracture). Saw palmetto as adjunct to pelvic floor PT and standard post-surgical management.
- Chronic prostatitis / CPPS — multidisciplinary approach. Saw palmetto can be one component but should not be expected to produce dramatic monotherapy benefit.
Key Research Papers
- Wilt TJ et al. (1998). Saw palmetto extracts for treatment of benign prostatic hyperplasia: a systematic review (nocturia outcomes). JAMA. — PubMed
- Vinarov AZ et al. (2019). Prostamol Uno in patients with benign prostatic hyperplasia and erectile dysfunction. Urologiia. — PubMed
- Suter A et al. (2013). Improving BPH symptoms and sexual dysfunctions with a saw palmetto preparation. Phytotherapy Research. — PubMed
- Kaplan SA et al. (2004). A prospective, 1-year trial using saw palmetto versus finasteride in the treatment of category III prostatitis/chronic pelvic pain syndrome. Journal of Urology. — PubMed
- Reissigl A et al. (2004). The use of phytotherapy for therapy of chronic abacterial prostatitis (Permixon observational data). European Urology Supplements. — PubMed
- Debruyne F et al. (2002). Comparison of a phytotherapeutic agent (Permixon) with an alpha-blocker (tamsulosin) in BPH (PERMAL trial, IPSS outcomes). European Urology. — PubMed
- Bayne CW et al. (2000). Serenoa repens (Permixon): a 5-alpha reductase types I and II inhibitor (mechanism for irritative LUTS). Prostate. — PubMed
- Goepel M et al. (2001). Saw palmetto extracts potently and noncompetitively inhibit human alpha-1 adrenoceptors in vitro. Prostate. — PubMed
- Paubert-Braquet M et al. (1996). Effect of the lipidic lipidosterolic extract of Serenoa repens on leukotriene B4 production by human neutrophils. Prostaglandins Leukotrienes and Essential Fatty Acids. — PubMed
- Glemain P et al. (2002). Tamsulosin with or without Serenoa repens in BPH: the OCOS trial. Progres en Urologie. — PubMed
- Stewart KL, Lephart ED (2023). Phytotherapy for the treatment of urinary disorders: a systematic review of clinical evidence. International Journal of Molecular Sciences. — PubMed
- Carraro JC et al. (1996). Comparison of phytotherapy (Permixon) with finasteride in the treatment of benign prostatic hyperplasia: a randomized international study of 1,098 patients. Prostate. — PubMed
PubMed Topic Searches
- PubMed: Saw palmetto nocturia
- PubMed: Serenoa overactive bladder
- PubMed: Saw palmetto chronic prostatitis
- PubMed: Post-prostatectomy urinary
- PubMed: Serenoa alpha-1 bladder neck
Connections
- Saw Palmetto Overview
- Saw Palmetto Benefits Hub
- Saw Palmetto for Prostate & BPH
- Saw Palmetto for Hair Loss
- Hormonal Effects & Cautions
- Benign Prostatic Hyperplasia (BPH)
- Prostate Conditions
- Urinary Tract Infections
- Erectile Dysfunction
- Low Testosterone & TRT
- PSA Test
- Testosterone Test
- Hormone Panel
- Zinc
- All Herbs