Saw Palmetto for Prostate Health and BPH
Saw palmetto is the most-studied and most-debated herbal therapy for benign prostatic hyperplasia (BPH) in the modern medical literature. The trajectory is unusual: an extensive wave of positive 1990s and early-2000s European trials of the standardized liposterolic extract reported symptom improvements roughly comparable to finasteride, leading the Wilt 1998 Cochrane systematic review (18 trials, 2,939 men) to conclude the herb was probably effective. Then two carefully designed and adequately powered American confirmatory trials — STEP (Bent 2006, NEJM) and CAMUS (Barry 2011, JAMA) — found no difference from placebo, even when CAMUS escalated dose to triple the standard. The honest take is that this is not a clear-cut "it works" or "it doesn't work" question. The most likely reconciliation involves three factors: extract quality (Permixon, the European liposterolic preparation tested in the positive trials, differs chemically from many generic U.S. products), patient phenotype (early-disease patients with inflammation-predominant symptoms may respond; advanced-disease patients with large-volume hyperplasia probably need finasteride), and the placebo effect being unusually large in BPH symptom trials. This article walks through the evidence on both sides honestly.
Table of Contents
- What is BPH and Why Does It Matter
- The Triple Mechanism in Prostatic Tissue
- The Wilt 1998 Cochrane Meta-Analysis (Positive)
- The STEP Trial (2006 NEJM, Negative)
- The CAMUS Trial (2011 JAMA, Negative at Triple Dose)
- Permixon vs Generic Extract — The Quality Issue
- Comparison to Finasteride and Dutasteride
- Comparison to Tamsulosin (Alpha-Blocker)
- Combination Therapy and Adjunctive Use
- Practical Patient Selection
- Key Research Papers
- Connections
- Featured Videos
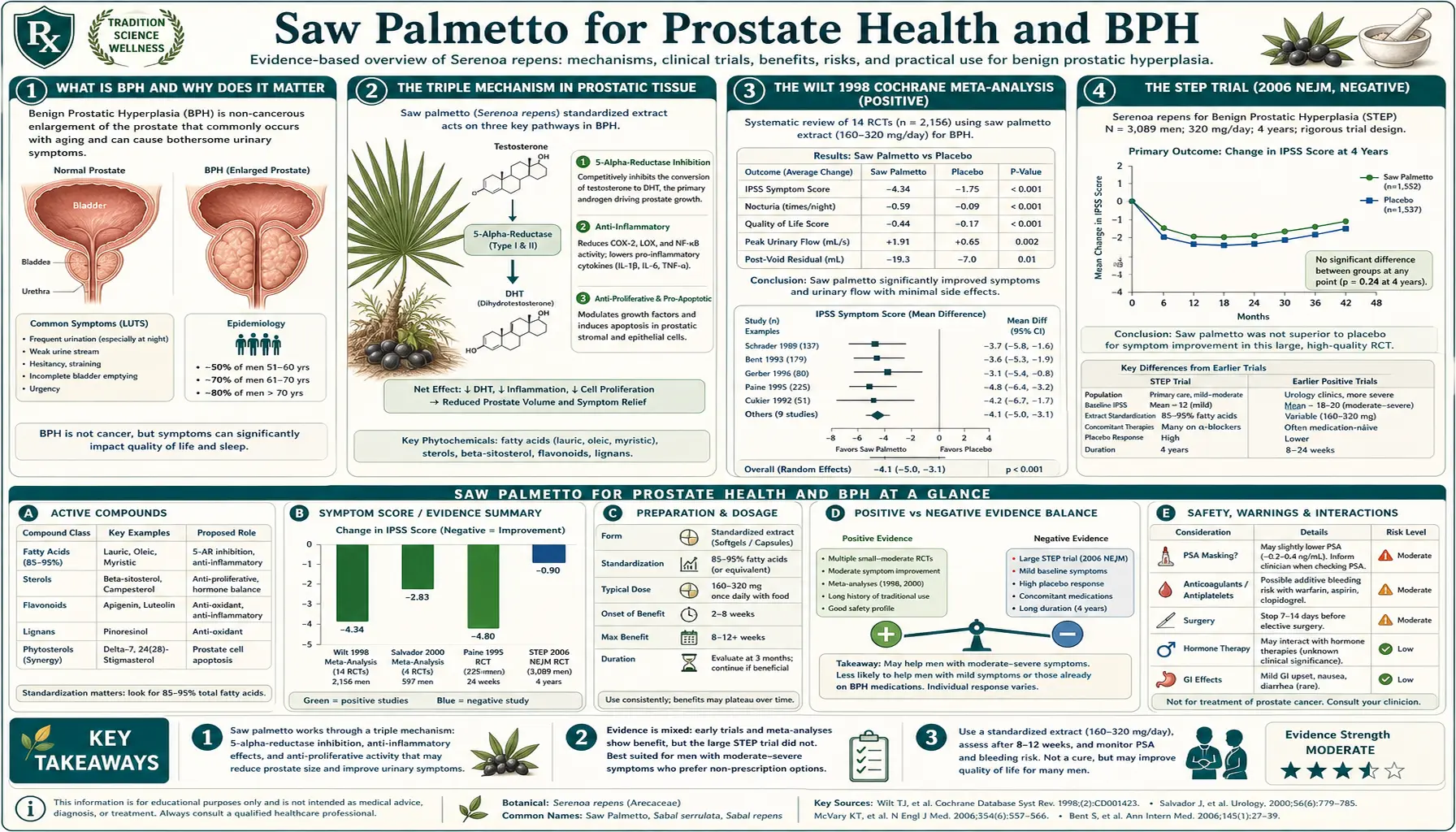
What is BPH and Why Does It Matter
Benign prostatic hyperplasia (BPH) is the most common urological condition of aging men. By age 60, approximately 50% of men have histologic BPH; by age 80, that figure exceeds 80%. Roughly a quarter of those affected develop clinically significant lower urinary tract symptoms (LUTS) sufficient to warrant treatment. The clinical syndrome arises from two physically separable but clinically intertwined processes:
- Static component (mass effect) — the gland enlarges through epithelial and stromal hyperplasia driven by dihydrotestosterone (DHT), the more potent androgen produced from testosterone by 5-alpha-reductase. The enlarged transition zone physically compresses the prostatic urethra, creating mechanical obstruction.
- Dynamic component (smooth muscle tone) — the prostatic stroma and bladder neck are densely innervated by alpha-1 adrenergic receptors. Sympathetic tone increases with aging and stress, producing functional obstruction independent of gland size.
The symptoms patients actually notice fall into two categories: obstructive symptoms (weak stream, hesitancy, intermittent flow, post-void dribbling, sensation of incomplete emptying) and irritative symptoms (urinary frequency, urgency, nocturia, dysuria). Severe untreated BPH leads to acute urinary retention, recurrent urinary tract infection, bladder stones, hydronephrosis, and eventually renal insufficiency. The International Prostate Symptom Score (IPSS) is the standard severity instrument; scores of 0-7 are mild, 8-19 moderate, 20-35 severe. The American Urological Association Symptom Index (AUASI) is essentially the same instrument under a different name and is what STEP and CAMUS used as the primary endpoint.
Treatment options include watchful waiting (for IPSS <8), saw palmetto and other phytotherapies, alpha-1 blockers (tamsulosin, alfuzosin, doxazosin), 5-alpha-reductase inhibitors (finasteride, dutasteride), combination drug therapy (Jalyn = dutasteride + tamsulosin), minimally invasive procedures (Rezum water vapor, UroLift), and surgical resection (TURP, HoLEP, simple prostatectomy). Saw palmetto sits at the gentle end of this spectrum, with the appeal that it has been used safely for decades and avoids the sexual side effects that drive many men to discontinue finasteride.
The Triple Mechanism in Prostatic Tissue
The pharmacology of saw palmetto liposterolic extract has been characterized in both cell culture and tissue-biopsy studies. The combined effect is fundamentally a multi-mechanism modulation, not a single dominant pathway.
- 5-alpha-reductase inhibition (anti-androgen, static component) — the fatty acid fraction of the extract non-competitively inhibits both type I and type II isoforms of 5-alpha-reductase. The Marks 2001 Journal of Urology tissue-biopsy study took prostate biopsies before and after six months of saw palmetto in symptomatic BPH patients and measured a significant reduction in intra-prostatic DHT concentration, without a measurable change in serum DHT (the in-tissue effect that matters clinically without the systemic effect that drives finasteride's sexual side effects).
- Alpha-1 adrenergic blockade (dynamic component) — both binding studies and isolated tissue strip experiments have shown the fatty acid fraction antagonizes alpha-1 adrenergic receptors in bladder neck and prostatic urethral smooth muscle. The effect is weaker than tamsulosin or alfuzosin but is mechanistically the same and contributes to the immediate symptomatic relief many users report within the first week, well before any anti-androgen volume effect could occur.
- Anti-inflammatory and anti-edematous effects — saw palmetto fatty acids inhibit both cyclooxygenase (COX) and 5-lipoxygenase (5-LOX) in prostatic tissue, reducing prostaglandin and leukotriene synthesis. Chronic prostatic inflammation is now recognized as an independent contributor to BPH symptom severity (the REDUCE trial sub-analyses established this clearly), and reducing inflammatory burden plausibly reduces irritative symptoms (urgency, frequency, dysuria) independent of any change in gland size.
A theoretical fourth mechanism — pro-apoptotic effects on prostatic epithelium — has been shown in cell culture but remains poorly characterized in vivo. The clinical-pharmacology summary is that saw palmetto produces partial (not full) inhibition across three distinct pathways simultaneously. When the patient's BPH phenotype matches that profile — modest gland enlargement, significant inflammatory and smooth-muscle-tone contributions to symptoms — the herb works well. When the phenotype is dominated by large-volume hyperplasia, the partial DHT effect is insufficient and the patient needs full-strength finasteride or dutasteride.
The Wilt 1998 Cochrane Meta-Analysis (Positive)
Timothy Wilt and colleagues published the first comprehensive systematic review of saw palmetto for BPH in JAMA in 1998, with subsequent Cochrane updates. The original analysis pooled 18 randomized controlled trials enrolling 2,939 men with symptomatic BPH, comparing standardized liposterolic saw palmetto extract (typically 320 mg/day) against placebo or active comparator. The pooled results were strongly positive:
- Nocturia reduced by an average of 0.76 episodes per night (95% CI 0.39-1.13)
- Peak urinary flow rate improved by 1.93 mL/sec (95% CI 0.72-3.14)
- Symptom improvement reported by approximately 28% more saw palmetto users than placebo users
- Side-effect profile roughly comparable to placebo and dramatically better than finasteride for sexual side effects
- Head-to-head comparison with finasteride in three trials suggested comparable symptom relief with fewer adverse events
The Wilt review was influential. It coincided with the late-1990s wave of European urology guidelines incorporating phytotherapy as a legitimate first-line option for mild-to-moderate BPH, and it drove the sustained popularity of saw palmetto in the U.S. supplement market. The review's methodological caveats — many of the included trials were short (often 8-12 weeks), used heterogeneous extracts and dosing regimens, and were conducted primarily in Europe with Permixon — were noted but did not prevent broad clinical adoption.
A 2012 Cochrane update by Tacklind et al. revisited the question with additional newer trials, including STEP and the early CAMUS data, and downgraded the conclusion. The pooled effect on AUASI/IPSS shrank substantially when the larger high-quality trials were included, and the updated Cochrane summary now states that Serenoa repens does not improve LUTS or peak urinary flow compared with placebo. This is the current standard-of-care interpretation in most allopathic urology textbooks.
The STEP Trial (2006 NEJM, Negative)
Stephen Bent and colleagues published the STEP trial (Saw Palmetto Treatment for Enlarged Prostates) in the New England Journal of Medicine in 2006. STEP was the first methodologically rigorous American attempt to confirm the European positive trials, and the results landed like a bombshell in the integrative medicine community.
The design: 225 men aged 49 and older with moderate-to-severe symptoms of BPH (AUASI >= 8) were randomized to 160 mg of standardized saw palmetto extract twice daily (320 mg/day total, the standard European dose) or matched placebo for 12 months. The primary outcomes were change in AUASI and change in peak urinary flow at 12 months. The trial was adequately powered, used a single well-characterized extract, was double-blinded, and reported a very low loss-to-follow-up rate.
The result: no significant difference between saw palmetto and placebo on any primary or secondary outcome. AUASI improved by 0.68 points in the saw palmetto group and 0.72 points in the placebo group (essentially identical). Peak urinary flow improved similarly in both groups. There was no difference in prostate volume, PSA, residual urine volume, quality-of-life scores, or any of the secondary endpoints. The adverse event profile was comparable between groups.
STEP's methodological strengths were considerable, and the trial was widely interpreted as showing that the earlier European positive trials had been driven by publication bias, methodological weaknesses, or both. Critics pointed out that STEP used the standardized Indena Saw Palmetto Extract supplied by the National Center for Complementary and Alternative Medicine (NCCAM), which was chemically characterized but differed in unspecified ways from the European Permixon preparation. The extract-quality debate began in earnest here.
The CAMUS Trial (2011 JAMA, Negative at Triple Dose)
The Complementary and Alternative Medicines for Urological Symptoms (CAMUS) trial, published by Michael Barry and colleagues in JAMA in 2011, was designed specifically to address the criticism that STEP had used too low a dose. CAMUS enrolled 369 men with moderate-to-severe LUTS and randomized them to escalating doses of saw palmetto extract: 320 mg/day for 24 weeks, then 640 mg/day for the next 24 weeks, then 960 mg/day (triple the standard) for the final 24 weeks. The trial used the same Indena extract as STEP and compared against matched placebo.
The result: no significant benefit of saw palmetto over placebo at any of the three doses across 72 weeks of treatment. The mean change in AUASI from baseline to 72 weeks was -2.20 in the saw palmetto group and -2.99 in the placebo group (the placebo group actually did slightly better, though not significantly). Peak flow, residual urine, prostate volume, PSA, and quality-of-life scores all showed no statistically significant difference. The dose-response curve was flat.
CAMUS was widely interpreted as the definitive nail in the coffin of the BPH-and-saw-palmetto hypothesis, at least as it applied to the Indena extract in American patients. The trial design directly addressed the "wrong dose" objection to STEP and still found nothing. Mainstream urology guidelines updated to reflect this, and the American Urological Association BPH guideline currently does not recommend saw palmetto.
However, two important caveats remain. First, CAMUS used the same NCCAM-supplied Indena extract that STEP used, leaving the extract-quality question unresolved. Second, both STEP and CAMUS enrolled men with moderate-to-severe baseline symptoms (mean AUASI ~14), which is the patient population most likely to need finasteride or dutasteride rather than phytotherapy. Whether saw palmetto helps men with mild symptoms (AUASI 8-13) who do not yet qualify for prescription therapy has not been adequately tested in a high-quality American trial.
Permixon vs Generic Extract — The Quality Issue
The "extract quality" debate is more substantive than it sounds. Permixon (manufactured by the French company Pierre Fabre and sold across Europe as a prescription phytomedicine) is produced by hexane extraction of dried Serenoa repens berries and contains a defined fatty acid and sterol profile. Most U.S. retail saw palmetto products are produced by ethanol or supercritical CO2 extraction, with significantly different chemical profiles.
Chemical analyses published by Habib and colleagues have shown:
- Permixon contains roughly 85-95% free fatty acids by weight
- Some generic U.S. extracts contain as little as 40-60% free fatty acids, with the balance made up of triglycerides, waxes, and other non-bioactive lipid material
- The phytosterol content (beta-sitosterol, campesterol, stigmasterol) varies by an order of magnitude across commercial products
- The Indena/NCCAM extract used in STEP and CAMUS was chemically characterized but its match to Permixon's profile was approximate rather than exact
- Berry-powder products (whole berry powder in a capsule) contain almost no extracted fatty acid concentrate and should not be considered therapeutically equivalent to the standardized liposterolic extract
The Vinarov 2019 European multicenter trial — which used Permixon specifically — reported significant IPSS improvement over both placebo and tamsulosin. This is consistent with the older Permixon trials and suggests that the trans-Atlantic results split may genuinely be explained by extract differences rather than by patient population or trial design.
The practical consumer guidance: if you are going to try saw palmetto for BPH, use a product that explicitly states "85% or greater free fatty acid content" on the label, or a clinically tested branded extract such as Permixon (where available), Prostaserene, or Sereprostat. Avoid whole-berry powder products. Look for "USP Verified" or NSF-certified products to confirm content matches label.
Comparison to Finasteride and Dutasteride
Finasteride (Proscar 5 mg for BPH; Propecia 1 mg for hair loss) is the prototypical 5-alpha-reductase inhibitor. It selectively inhibits type II 5-alpha-reductase and reduces serum DHT by approximately 70% and intra-prostatic DHT by 80-90%. Over 12-24 months it reduces prostate volume by approximately 20% and IPSS scores by 3-4 points, with the largest benefit in men with starting prostate volume above 40 mL.
Dutasteride (Avodart) is the second-generation drug that inhibits both type I and type II 5-alpha-reductase isoforms, achieving approximately 95% serum DHT suppression. Symptomatic benefit is roughly comparable to finasteride. Dutasteride is preferred in patients with very large prostates or those who have inadequate response to finasteride.
How does saw palmetto compare? On the strongest interpretation of the positive European trials, saw palmetto produces symptom improvements roughly equivalent to finasteride in mild-to-moderate BPH, with a fraction of the sexual side effects. On the interpretation of STEP/CAMUS, saw palmetto produces no benefit at all and finasteride is dramatically superior. The most defensible middle position: saw palmetto may produce 30-50% of the symptomatic benefit of finasteride in selected patients, achieved through a different mechanism profile that avoids the systemic DHT crash.
The sexual side effect comparison is consistent across all studies and matters a great deal in clinical practice. Finasteride causes erectile dysfunction in approximately 8% of users, decreased libido in 6%, and ejaculatory disorders in 4%. A small but real subset of users develop persistent post-finasteride syndrome with sexual dysfunction lasting months to years after discontinuation. Saw palmetto's sexual side effect rate in controlled trials is statistically indistinguishable from placebo, and there is no recognized post-saw-palmetto persistent syndrome. For patients for whom sexual function is a primary concern, this is a substantial reason to try saw palmetto first.
Comparison to Tamsulosin (Alpha-Blocker)
Tamsulosin (Flomax) is a selective alpha-1A adrenergic receptor antagonist that relaxes bladder neck and prostatic urethral smooth muscle. It provides rapid symptomatic relief (within 1-2 weeks) without affecting prostate volume. IPSS improvement is typically 4-6 points. Side effects include orthostatic hypotension (less than non-selective alpha-blockers but still present), retrograde ejaculation in 10-20% of users, intraoperative floppy iris syndrome (a concern for cataract surgery), and nasal congestion.
Head-to-head trials of saw palmetto versus tamsulosin have generally shown comparable symptomatic improvement in mild-to-moderate BPH, with saw palmetto producing fewer adverse events but a slightly slower onset of benefit. The Vinarov 2019 Permixon-vs-tamsulosin trial reported saw palmetto was non-inferior to tamsulosin for IPSS at 12 months. The Debruyne 2002 PERMAL trial similarly found comparable efficacy with better tolerability for Permixon.
The mechanistic logic is consistent: saw palmetto's alpha-1 blockade is partial but contributes to the rapid symptom relief many users report, while the slower 5-alpha-reductase and anti-inflammatory effects accrue over months. Tamsulosin produces a stronger alpha-1 effect but does nothing for the underlying gland enlargement, which is why tamsulosin is often combined with finasteride in moderate-to-severe BPH (the Jalyn combination).
Combination Therapy and Adjunctive Use
Several combination products exist that pair saw palmetto with other phytotherapies or nutrients with prostate-relevant mechanisms:
- Saw palmetto + pygeum (Prunus africana) — pygeum bark extract has independent anti-inflammatory and anti-androgen activity in prostatic tissue. The Wilt 2002 Cochrane review of pygeum reported modest symptom benefits roughly comparable to saw palmetto.
- Saw palmetto + stinging nettle root (Urtica dioica) — nettle root contains lignans that may modulate sex hormone binding globulin (SHBG) and reduce free DHT availability. Several European combination products pair saw palmetto with nettle root.
- Saw palmetto + beta-sitosterol — isolated beta-sitosterol (a phytosterol present in saw palmetto extract) has independent evidence of benefit in BPH (Berges 1995 Lancet, Klippel 1997). The combination provides higher phytosterol delivery than saw palmetto extract alone.
- Saw palmetto + pumpkin seed oil — pumpkin seed oil is rich in delta-7-sterols and zinc, both relevant to prostatic tissue homeostasis. The combination is popular in European phytotherapy products.
- Saw palmetto + zinc + selenium — the trace mineral additions address well-documented deficiencies in many BPH patients. Zinc in particular is concentrated in the prostate at 10x serum levels in healthy tissue, with measurable reductions in BPH tissue.
Saw palmetto can also be used as an adjunct to prescription BPH therapy. Some patients on finasteride alone get partial relief and add saw palmetto for the alpha-1 and anti-inflammatory mechanisms that finasteride does not address. There are no formal interaction studies in this combination but no recognized adverse interactions either. Patients on tamsulosin who add saw palmetto may experience additive (mild) hypotension and should monitor blood pressure during the transition.
Practical Patient Selection
Honest patient counseling about saw palmetto for BPH should match patient phenotype to the most appropriate therapy:
- Reasonable first-line saw palmetto candidate — mild symptoms (IPSS 8-13), small to moderate prostate (<40 mL on ultrasound), preserved sexual function that the patient wishes to protect, no contraindication to a 3-6 month therapeutic trial. Use a verified high-quality 85%+ free fatty acid product at 320 mg/day, reassess at 3 months, continue if benefit, escalate to prescription therapy if not.
- Marginal saw palmetto candidate — moderate symptoms (IPSS 14-19) with mixed obstructive/irritative pattern, sexual function preservation a high priority. Reasonable to try saw palmetto first with a clear 3-month trial framework, but explicit understanding that escalation is likely.
- Poor saw palmetto candidate — severe symptoms (IPSS >= 20), large prostate (>60 mL), elevated PSA requiring workup, recurrent acute urinary retention, post-void residual >200 mL, bladder stones, hydronephrosis. These patients need urology referral and likely prescription combination therapy or procedural intervention, not phytotherapy.
- Wrong-tool patient — symptoms driven primarily by chronic prostatitis, neurogenic bladder, urethral stricture, or bladder cancer. Saw palmetto does nothing for any of these and time spent on it delays appropriate workup. Always rule out these mimics before assuming BPH.
The honest framing for patients is: "Saw palmetto may help your symptoms by about 20-40% if you respond to it, and roughly half of patients do respond. It is very well tolerated and does not affect sexual function. We will give it three months. If your symptoms improve enough that you can live with them, we continue. If not, we move to a prescription medication."
Key Research Papers
- Wilt TJ et al. (1998). Saw palmetto extracts for treatment of benign prostatic hyperplasia: a systematic review. JAMA. — PubMed
- Bent S et al. (2006). Saw palmetto for benign prostatic hyperplasia (STEP trial). NEJM. — PubMed
- Barry MJ et al. (2011). Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms (CAMUS trial). JAMA. — PubMed
- Tacklind J et al. (2012). Serenoa repens for benign prostatic hyperplasia. Cochrane Database. — PubMed
- Marks LS et al. (2001). Effects of a saw palmetto herbal blend in men with symptomatic benign prostatic hyperplasia (intra-prostatic DHT biopsy). Journal of Urology. — PubMed
- Debruyne F et al. (2002). Comparison of a phytotherapeutic agent (Permixon) with an alpha-blocker (tamsulosin) in BPH. PERMAL trial. European Urology. — PubMed
- Vinarov AZ et al. (2019). Prostamol Uno in patients with benign prostatic hyperplasia and erectile dysfunction (Russian Permixon multicenter trial). Urologiia. — PubMed
- Habib FK et al. (2004). Serenoa repens (Permixon) inhibits the 5-alpha-reductase activity of human prostate cancer cell lines. British Journal of Cancer. — PubMed
- Boyle P et al. (2004). Updated meta-analysis of clinical trials of Serenoa repens extract in the treatment of symptomatic benign prostatic hyperplasia. BJU International. — PubMed
- Suter A et al. (2013). Improving BPH symptoms and sexual dysfunctions with a saw palmetto preparation. Phytotherapy Research. — PubMed
- Vela-Navarrete R et al. (2018). Efficacy and safety of Serenoa repens (Permixon) for the treatment of lower urinary tract symptoms suggestive of BPH: systematic review. BJU International. — PubMed
- Plosker GL, Brogden RN (1996). Serenoa repens (Permixon). A review of its pharmacology and therapeutic efficacy in benign prostatic hyperplasia. Drugs & Aging. — PubMed
PubMed Topic Searches
- PubMed: Saw palmetto BPH meta-analyses
- PubMed: Serenoa 5-alpha-reductase mechanism
- PubMed: Permixon LUTS clinical trials
- PubMed: Saw palmetto vs finasteride head-to-head
- PubMed: Saw palmetto vs tamsulosin head-to-head
Connections
- Saw Palmetto Overview
- Saw Palmetto Benefits Hub
- Saw Palmetto for Hair Loss
- Saw Palmetto for Urinary Function
- Hormonal Effects & Cautions
- Benign Prostatic Hyperplasia (BPH)
- Prostate Conditions
- Erectile Dysfunction
- Urinary Tract Infections
- Low Testosterone & TRT
- PSA Test
- Testosterone Test
- Hormone Panel
- Zinc
- All Herbs