Saw Palmetto for Hair Loss
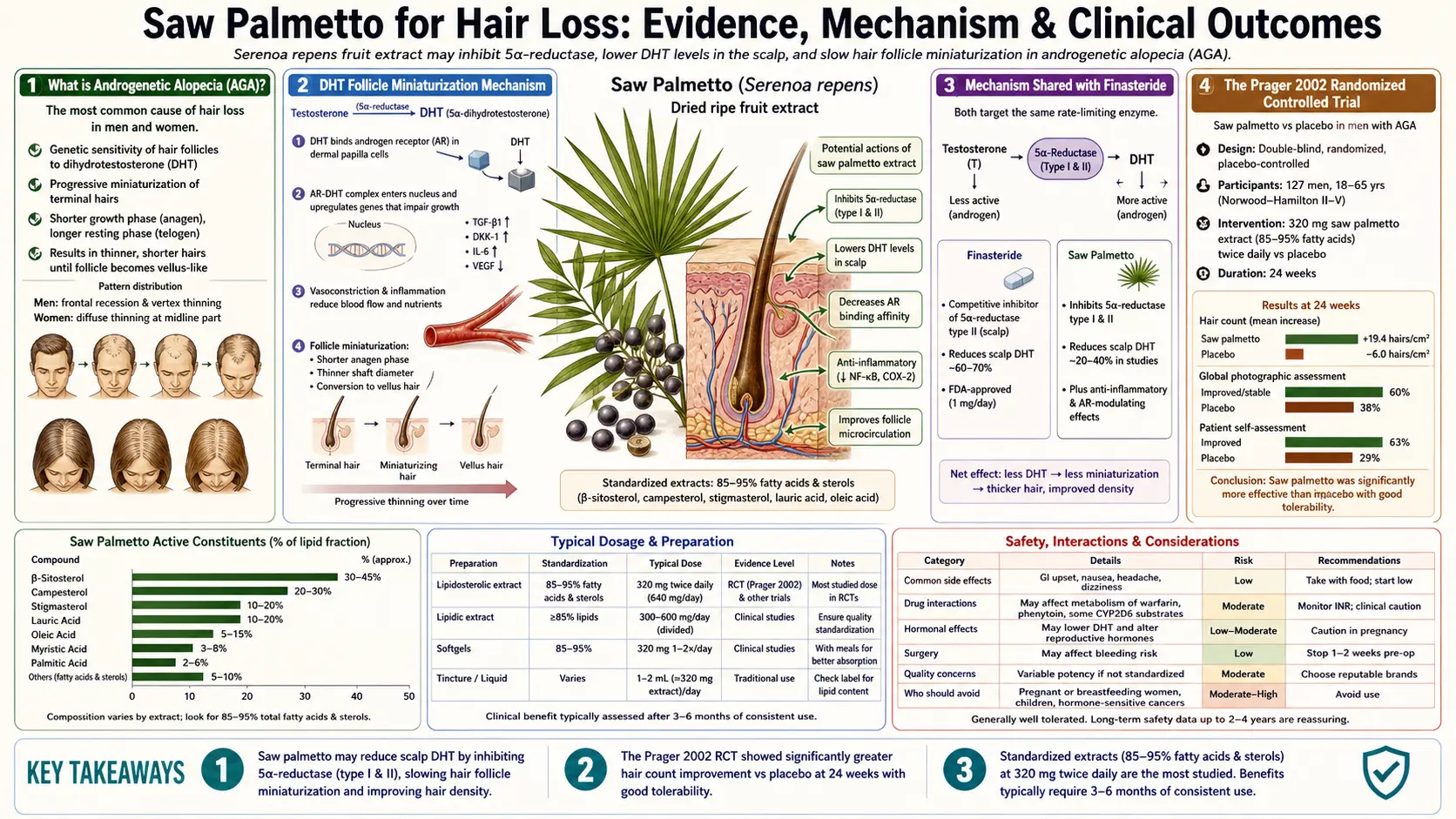
Androgenetic alopecia — male-pattern and female-pattern hair loss — is driven by the same dihydrotestosterone (DHT) mechanism that drives benign prostatic hyperplasia, just expressed in a different tissue. Genetically susceptible hair follicles in the temples, vertex, and crown produce 5-alpha-reductase locally and convert testosterone into DHT, which progressively miniaturizes those follicles over years to decades. The DHT-blocking logic that underlies the prescription standard finasteride is precisely the same logic that drives saw palmetto's use for hair loss. The randomized controlled evidence base is thinner than for BPH but more consistently positive — the Prager 2002 trial reported approximately 60% of saw palmetto users had visible improvement versus 11% in the placebo group, and subsequent open-label and observational studies have reported comparable findings. The honest framing for patients: saw palmetto produces perhaps 30-40% of the efficacy of oral finasteride for androgenetic alopecia, with a dramatically better tolerability profile and no recognized post-discontinuation persistent syndrome, taking 6-12 months to show benefit and requiring lifelong continuation.
Interactive Visualization Hair Growth & Loss — shrink a follicle with DHT, or shed on a three-month delay Cycle a scalp of follicles through anagen, catagen and telogen, then miniaturize them with DHT year by year — or dump them all into shedding three months after a stressor. Launch →
Table of Contents
- What is Androgenetic Alopecia
- The DHT Follicle Miniaturization Mechanism
- Mechanism Shared with Finasteride
- The Prager 2002 RCT
- Subsequent Observational and Open-Label Data
- Topical Saw Palmetto vs Oral
- Comparison to Finasteride
- Combination with Minoxidil
- Realistic Timeline and Expectations
- Female-Pattern Hair Loss
- Key Research Papers
- Connections
- Featured Videos
What is Androgenetic Alopecia
Androgenetic alopecia (AGA) is the most common cause of hair loss in both men and women. By age 50, approximately 50% of men show clinically evident male-pattern baldness; lifetime prevalence in men approaches 80%. In women, the corresponding female-pattern hair loss (FPHL) affects roughly 30% by age 70, typically with diffuse thinning of the central scalp rather than the receding hairline and crown balding seen in men.
The clinical pattern in men follows the Hamilton-Norwood scale: stage I (no recession) progressing through frontal-temporal recession, vertex thinning, and eventual confluent baldness sparing only the occipital horseshoe of permanent terminal hairs. The classification has prognostic and therapeutic value — early-stage AGA (Norwood I-III) is the population most likely to respond to medical therapy, while late-stage AGA (Norwood VI-VII) has too few viable miniaturized follicles remaining for medical therapy to restore meaningful hair.
The underlying biology is a genetically programmed sensitivity of follicles in the androgen-sensitive scalp regions (frontal, vertex) to dihydrotestosterone. The occipital follicles are genetically resistant to DHT — which is why hair transplants from the occipital donor area to the bald frontal region thrive permanently, and why DHT-blocking medications spare the occipital region from any effect, beneficial or otherwise.
The DHT Follicle Miniaturization Mechanism
Androgen-sensitive follicles in the scalp express 5-alpha-reductase (both type I and type II isoforms, with type I more abundant in scalp than in prostate) and androgen receptors. Circulating testosterone freely diffuses into the follicle, is locally converted to DHT, and binds to the androgen receptor. The DHT-AR complex then translocates to the nucleus and modifies the transcription of dozens of follicle-relevant genes.
The net effect on a susceptible follicle is progressive miniaturization across consecutive hair cycles. Each anagen (growth) phase becomes shorter, the resulting hair shaft becomes thinner and shorter, and the follicle eventually produces only a fine vellus hair instead of a terminal hair. Over years to decades, the affected scalp region transitions from full terminal-hair coverage to fine vellus hairs that are clinically invisible at conversational distance. The follicle is never actually destroyed (which is why medical therapy can produce some regrowth even years into AGA) — it is merely deactivated to vellus production.
Several therapeutic approaches address this mechanism at different steps:
- Reduce local DHT — the 5-alpha-reductase inhibitor approach. Finasteride (oral 1 mg, type II selective) and dutasteride (oral 0.5 mg, dual type I and II) reduce serum and follicular DHT. Saw palmetto produces partial inhibition of both isoforms.
- Block androgen receptor — spironolactone (oral, often used in women) and topical antiandrogens compete with DHT for binding to the receptor.
- Stimulate follicle metabolism directly — minoxidil (topical 2-5%) and oral low-dose minoxidil (0.25-2.5 mg) open potassium channels in follicle vasculature and prolong anagen. This works through a non-androgen mechanism and is complementary to DHT-blocking agents.
- Reduce inflammation — ketoconazole shampoo, low-level laser therapy, and others may contribute by addressing the perifollicular inflammation present in some AGA patients.
Mechanism Shared with Finasteride
Saw palmetto and finasteride share the 5-alpha-reductase inhibition mechanism but differ substantially in potency and selectivity:
- Finasteride — selective type II inhibitor (the dominant isoform in prostate; secondary in scalp). Oral 1 mg daily reduces serum DHT by approximately 70% and scalp DHT by approximately 60%. Effect persists for the lifetime of treatment; DHT rebounds within weeks of discontinuation.
- Dutasteride — dual type I and II inhibitor. Oral 0.5 mg daily reduces serum DHT by approximately 95%. Off-label for AGA in the U.S.; approved in some countries including South Korea and Japan.
- Saw palmetto — non-competitive inhibitor of both type I and type II, with modest potency. Oral 320 mg/day reduces measured intra-prostatic DHT (the Marks 2001 biopsy study) but produces little measurable change in serum DHT. Scalp-level effects have not been directly measured in biopsy studies but are inferred from clinical hair-density outcomes.
The relevant therapeutic insight: finasteride's 70% DHT reduction is far more than necessary to halt AGA progression in most patients. The dose-response curve flattens above approximately 40% DHT reduction. Saw palmetto's partial inhibition may be sufficient for many patients while remaining below the threshold at which systemic anti-androgen side effects (libido reduction, erectile dysfunction, ejaculatory disorders, gynecomastia) become clinically apparent.
This is the mechanistic basis for the consistent observation that saw palmetto produces hair-density improvement in a substantial fraction of users with essentially no recognized sexual side effects — in contrast to finasteride, which produces clear hair-density improvement in 80-90% of users at the cost of sexual side effects in 5-15% and persistent post-finasteride syndrome in a small but real subset.
The Prager 2002 RCT
The Prager 2002 trial published in the Journal of Alternative and Complementary Medicine is the foundational randomized controlled evidence for saw palmetto in androgenetic alopecia. The design was small but well-conducted:
- 34 men aged 23-64 with mild-to-moderate AGA (Norwood II-IV)
- Randomized to a botanical 5-alpha-reductase inhibitor combination containing 200 mg saw palmetto extract and 50 mg beta-sitosterol twice daily, or matched placebo
- Treatment duration of approximately 5 months
- Outcome assessed by blinded investigator photograph review using a 7-point change scale (very much worse to very much better) and by self-report
The results were striking for such a small trial: 60% of subjects in the active-treatment group were rated as improved by the blinded investigator, versus 11% in the placebo group (p = 0.02). Self-reported improvement was similar. No adverse events of consequence were reported in either group. Sexual function was not formally measured but no spontaneous reports of dysfunction emerged.
The trial has obvious limitations — small sample size, relatively short follow-up, combination product rather than saw palmetto alone, primary outcome based on photograph review rather than hair counts. But the magnitude of the effect and the alignment with the established DHT-blocking mechanism made it a watershed paper for the integrative dermatology community, and the conclusions have generally held up in subsequent larger studies.
Subsequent Observational and Open-Label Data
Subsequent studies have generally supported the Prager findings:
- Rossi 2012 — 100 male AGA patients randomized to oral saw palmetto 320 mg/day or finasteride 1 mg/day for 2 years. Both treatments produced significant improvement; finasteride was superior (approximately 38% improvement vs 33% for saw palmetto in the frontal region; 68% vs 60% in the vertex), but saw palmetto produced statistically significant benefit. Side effects were more common in the finasteride group.
- Wessagowit 2016 — small Thai study of topical saw palmetto extract showed improvement in hair shaft thickness in men with AGA over a 24-week period.
- Murugusundram 2009 — open-label study using a combination saw palmetto/biotin/copper product reported improvement in hair density and shedding in both men and women.
- Verdolini 2002, Sinclair 2011 — observational case series suggesting benefit for AGA in clinical practice when combined with topical minoxidil.
- Evron 2020 — systematic review of botanical 5-alpha-reductase inhibitors for AGA concluded saw palmetto has the strongest evidence base among herbal options, though substantially weaker than for pharmaceutical 5-alpha-reductase inhibitors.
The cumulative evidence picture: saw palmetto produces measurable improvement in androgenetic alopecia in a substantial fraction of users (probably 40-60% on the most defensible interpretation), with effect sizes smaller than oral finasteride but achieved with a far more favorable tolerability profile. The evidence base is admittedly thin compared to the dense randomized-trial evidence for finasteride, but it is internally consistent across multiple study designs and aligns with the established DHT-blocking mechanism.
Topical Saw Palmetto vs Oral
Saw palmetto is available in both oral capsule and topical (lotion, shampoo, scalp serum) formulations. The relative merits:
- Oral 320 mg/day — the dose used in essentially all the published clinical trials. Produces measurable intra-prostatic DHT reduction in biopsy studies (Marks 2001), inferred to produce comparable scalp DHT reduction. Six to twelve months to clinically visible effect on hair. Side effect profile essentially comparable to placebo in controlled trials. Cost roughly $0.30-$0.80 per day for verified high-quality 85%+ free fatty acid product.
- Topical (typically 1-5% saw palmetto extract in lotion or scalp serum) — the theoretical advantage is targeted delivery to scalp follicles without systemic absorption. The practical reality is that the published evidence base is much thinner than for oral, several topical products have proprietary formulations that are not chemically characterized, and the question of whether the active fatty acids actually penetrate the scalp barrier to reach the follicle target depth has not been rigorously answered.
- Saw palmetto shampoo (typically 0.5-2%) — the contact time of shampoo with scalp is far too brief (1-3 minutes) for meaningful absorption of fatty acid actives. Shampoos may have some adjunctive value through ketoconazole-like anti-inflammatory effects on the scalp but should not be relied on as primary therapy.
The most defensible recommendation: if you choose saw palmetto for AGA, use the oral 320 mg/day standardized liposterolic extract that has been studied in the published trials. Add topical minoxidil 5% once or twice daily for additive non-androgen effect. Topical saw palmetto products may be adjunctive but should not replace oral.
Comparison to Finasteride
Finasteride 1 mg/day (the FDA-approved dose for AGA, marketed as Propecia) remains the most extensively evidenced oral medical therapy for AGA. The trade-offs between finasteride and saw palmetto:
- Efficacy — finasteride: approximately 80-90% of users show improvement or stabilization at 1 year, with the strongest response in the vertex. Saw palmetto: approximately 40-60% show improvement, with somewhat smaller magnitude per responder. Rossi 2012 head-to-head suggested finasteride was modestly superior but not dramatically so.
- Sexual side effects — finasteride: 5-10% report decreased libido, 5-8% report erectile dysfunction, 2-4% report ejaculation disorders, <1% develop persistent post-finasteride syndrome. Saw palmetto: rates in controlled trials are statistically indistinguishable from placebo. No recognized persistent syndrome.
- Gynecomastia risk — finasteride: approximately 0.4% develop palpable breast tissue enlargement, occasionally requiring discontinuation. Saw palmetto: no reported cases in the controlled literature.
- Prostate cancer interaction — finasteride lowers PSA by approximately 50%, requiring physicians to double the measured PSA when interpreting cancer screening tests. Finasteride may shift detected cancers toward higher Gleason grades (the PCPT debate). Saw palmetto produces minimal PSA effect and does not complicate prostate cancer screening.
- Cost — finasteride: generic 1 mg costs approximately $0.30-$1.00/day depending on source. Saw palmetto: approximately $0.30-$0.80/day for verified high-quality product. Both are affordable.
- Discontinuation pattern — both medications require continuous lifetime use to maintain benefit; both produce hair loss reversion to baseline within 12 months of discontinuation. Persistent post-finasteride syndrome is a minority outcome but is the most serious dealbreaker for some patients.
The honest framing for patients: finasteride produces more reliable and somewhat stronger benefit, but at the cost of a meaningful sexual side effect risk that scares many men away from initiating or continuing therapy. Saw palmetto produces somewhat less reliable benefit but with essentially no sexual side effect risk. For patients who decline finasteride for any reason, or who tried finasteride and discontinued for side effects, saw palmetto is a reasonable alternative that often produces sufficient benefit to satisfy the patient's goals.
Combination with Minoxidil
Minoxidil (topical Rogaine 2% or 5%) and oral low-dose minoxidil (0.25-2.5 mg) work through a non-androgen mechanism — potassium channel opening, follicle vascular bed dilation, and prolongation of the anagen growth phase. The mechanism is entirely complementary to DHT-blocking agents, and the combination of minoxidil with finasteride or saw palmetto is generally superior to either monotherapy.
The standard practice in AGA management is to use minoxidil and a DHT-blocker together from the start, on the rationale that the two address different aspects of the underlying pathology. For patients choosing saw palmetto over finasteride, the combination is saw palmetto 320 mg/day oral + minoxidil 5% topical once or twice daily (or oral minoxidil 0.25-1.25 mg/day for those who cannot tolerate topical).
The realistic timeline with combination therapy: minoxidil produces visible effects faster (3-6 months) than saw palmetto (6-12 months), so the early benefit is largely from minoxidil and the late stabilization and longer-term maintenance is largely from saw palmetto. Some patients see a transient increase in shedding (telogen effluvium) during the first 4-8 weeks of minoxidil — this is the cycle synchronization effect of pushed-into-anagen follicles, not a sign that the treatment is failing, and resolves spontaneously.
Realistic Timeline and Expectations
Saw palmetto for AGA is a long-term commitment, not a quick fix. The realistic patient expectation should be:
- Months 0-3 — no visible change. Don't expect any. The therapeutic effect is mediated by changes in follicle cycle behavior over multiple cycles, and visible hair shaft changes lag the underlying biology by months. If you abandon treatment at month 2 because "it's not working," you have not given it a fair trial.
- Months 3-6 — possible reduction in shedding, possible early sense of slightly thicker hair. Reduced shedding is often the first noticeable change. Reduced shedding without visible regrowth is a real treatment response — it means the follicle cycle is normalizing.
- Months 6-12 — visible hair density improvement in responders. This is when the photograph or in-mirror evaluation should show stabilization at minimum and modest regrowth in many users. Take baseline standardized photographs (well-lit, same camera angle and distance, dry hair) at month 0 and compare honestly at months 6 and 12.
- Months 12-24 — continued slow improvement plateauing toward stable maintenance. The maximum benefit is usually achieved by 18-24 months and is maintained as long as treatment continues.
- Discontinuation — benefit reverses over 6-18 months back to the trajectory the patient would have been on without treatment. Saw palmetto is not curative; it is maintenance therapy that requires lifetime continuation.
Patient expectations should be calibrated to "modest improvement and stabilization" rather than "thick full head of hair." AGA medical therapy at its best stops or modestly reverses miniaturization. It does not bring back hair that has been gone for years; for that, hair transplantation is the only effective option.
Female-Pattern Hair Loss
Female-pattern hair loss (FPHL) shares the DHT-driven follicle miniaturization mechanism with male AGA but typically presents as diffuse central scalp thinning rather than the temporal recession and vertex balding of men. The Ludwig classification (stages I-III) is the standard severity instrument. Postmenopausal women are particularly affected, as the loss of ovarian estrogen production unmasks the underlying androgen sensitivity.
Saw palmetto's use in FPHL is less well-studied than in male AGA but follows the same logic. The herb is appealing for women because oral finasteride is generally avoided in women of reproductive potential (teratogenicity concern; not approved by FDA for women) and finasteride's efficacy in postmenopausal women is mixed. Spironolactone (oral, off-label) is the most-used pharmaceutical alternative for FPHL but has its own side effect profile.
Saw palmetto 320 mg/day combined with topical minoxidil 2-5% is a reasonable initial regimen for women with FPHL who decline or cannot use spironolactone. The Hugo Perez 2004 small open-label study reported improvement in approximately 70% of treated postmenopausal women with FPHL over 18 months. Larger controlled trials are lacking.
Critically, premenopausal women should consult their physician before using saw palmetto for hair loss, both because the underlying cause of FPHL in premenopausal women is more likely to require workup (PCOS, thyroid disease, iron deficiency) and because the anti-androgen effects of saw palmetto have theoretical though not documented implications for hormonal contraception. See the Hormonal Effects & Cautions page for the full safety discussion in women, including PCOS and hirsutism applications.
Key Research Papers
- Prager N et al. (2002). A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. Journal of Alternative and Complementary Medicine. — PubMed
- Rossi A et al. (2012). Comparative effectiveness of finasteride vs Serenoa repens in male androgenetic alopecia: a two-year study. International Journal of Immunopathology and Pharmacology. — PubMed
- Wessagowit V et al. (2016). Treatment of male androgenetic alopecia with topical products containing Serenoa repens extract. Australasian Journal of Dermatology. — PubMed
- Murugusundram S (2009). Serenoa repens: does it have any role in the management of androgenetic alopecia? Journal of Cutaneous and Aesthetic Surgery. — PubMed
- Evron E et al. (2020). Natural hair supplement: friend or foe? Saw palmetto, a systematic review in alopecia. Skin Appendage Disorders. — PubMed
- Sinclair R et al. (2011). The role of hair colour in scalp hair preservation. Australasian Journal of Dermatology. — PubMed
- Dhariwala MY, Ravikumar P (2019). An overview of herbal alternatives in androgenetic alopecia. Journal of Cosmetic Dermatology. — PubMed
- Hagino T et al. (2023). Effects of an oral hair growth supplement containing saw palmetto and other plant-derived ingredients. Journal of Cosmetic Dermatology. — PubMed
- Trueb RM (2009). Pharmacologic interventions in aging hair. Clinical Interventions in Aging. — PubMed
- Hugo Perez BS (2004). Ketoconazole as an adjunct to finasteride in the treatment of androgenetic alopecia in men. Medical Hypotheses. — PubMed
- Olsen EA et al. (1991). Topical minoxidil in early male pattern baldness. Journal of the American Academy of Dermatology. — PubMed
- Kaufman KD et al. (1998). Finasteride in the treatment of men with androgenetic alopecia. Journal of the American Academy of Dermatology. — PubMed
PubMed Topic Searches
- PubMed: Saw palmetto AGA
- PubMed: Serenoa 5-alpha-reductase hair
- PubMed: Botanical 5-AR inhibitor hair loss
- PubMed: Topical saw palmetto scalp
- PubMed: Finasteride vs herbal AGA
Connections
- Hair Growth, Thinning & Why Hair Falls Out — interactive animation
- Saw Palmetto Overview
- Saw Palmetto Benefits Hub
- Saw Palmetto for Prostate & BPH
- Saw Palmetto for Urinary Function
- Hormonal Effects & Cautions
- Alopecia
- Hair Loss
- Polycystic Ovary Syndrome (PCOS)
- Testosterone Test
- Hormone Panel
- Zinc
- All Herbs