Oregano for Antibacterial Spectrum — Carvacrol, Thymol, and MRSA
Oregano essential oil is the most extensively studied antimicrobial culinary herb. Its two principal phenolic monoterpenoids — carvacrol (typically 50–80% of the essential oil) and thymol (typically 1–30%) — are small, lipophilic phenols that partition into microbial cell membranes, dissipate the proton-motive force, and at higher concentrations cause frank leakage of K+, ATP, and cytoplasmic contents. Because the target is the lipid bilayer itself rather than a specific enzyme, point mutations cannot easily confer resistance: oregano oil retains in vitro activity against methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), and multidrug-resistant Gram-negative pathogens including some Pseudomonas, Klebsiella, and E. coli isolates. The Nostro 2007 work, an oral candidiasis pilot, and the commercial "P73" carvacrol-standardized formulation are the touchstone references. This deep-dive covers the mechanism, the published in vitro and clinical evidence, the critical distinction between "oil of oregano" capsules and undiluted essential oil, and the dilution requirements that prevent mucosal burns at the concentrations needed for activity.
Table of Contents
- The Two Phenols: Carvacrol and Thymol
- Membrane-Disruption Mechanism in Detail
- Gram-Positive Spectrum (Staph, Strep, Enterococcus)
- MRSA — The Nostro 2007 Work and Follow-On Studies
- Gram-Negative Spectrum (E. coli, Salmonella, Pseudomonas, Klebsiella)
- Oral Candidiasis Pilot (Antibacterial Crossover)
- "Oil of Oregano" vs Essential Oil vs Culinary Oregano — Concentrations
- The P73 Carvacrol-Standardized Formulation
- Dosing and Dilution Requirements
- Cautions, Drug Interactions, and Mucosal-Burn Risk
- Key Research Papers
- Connections
- Featured Videos
The Two Phenols: Carvacrol and Thymol
The antimicrobial activity of oregano essential oil is concentrated in two structurally related phenolic monoterpenoids. Both are small lipophilic phenols (molecular weight 150 daltons) that differ only in the position of their hydroxyl group on the aromatic ring:
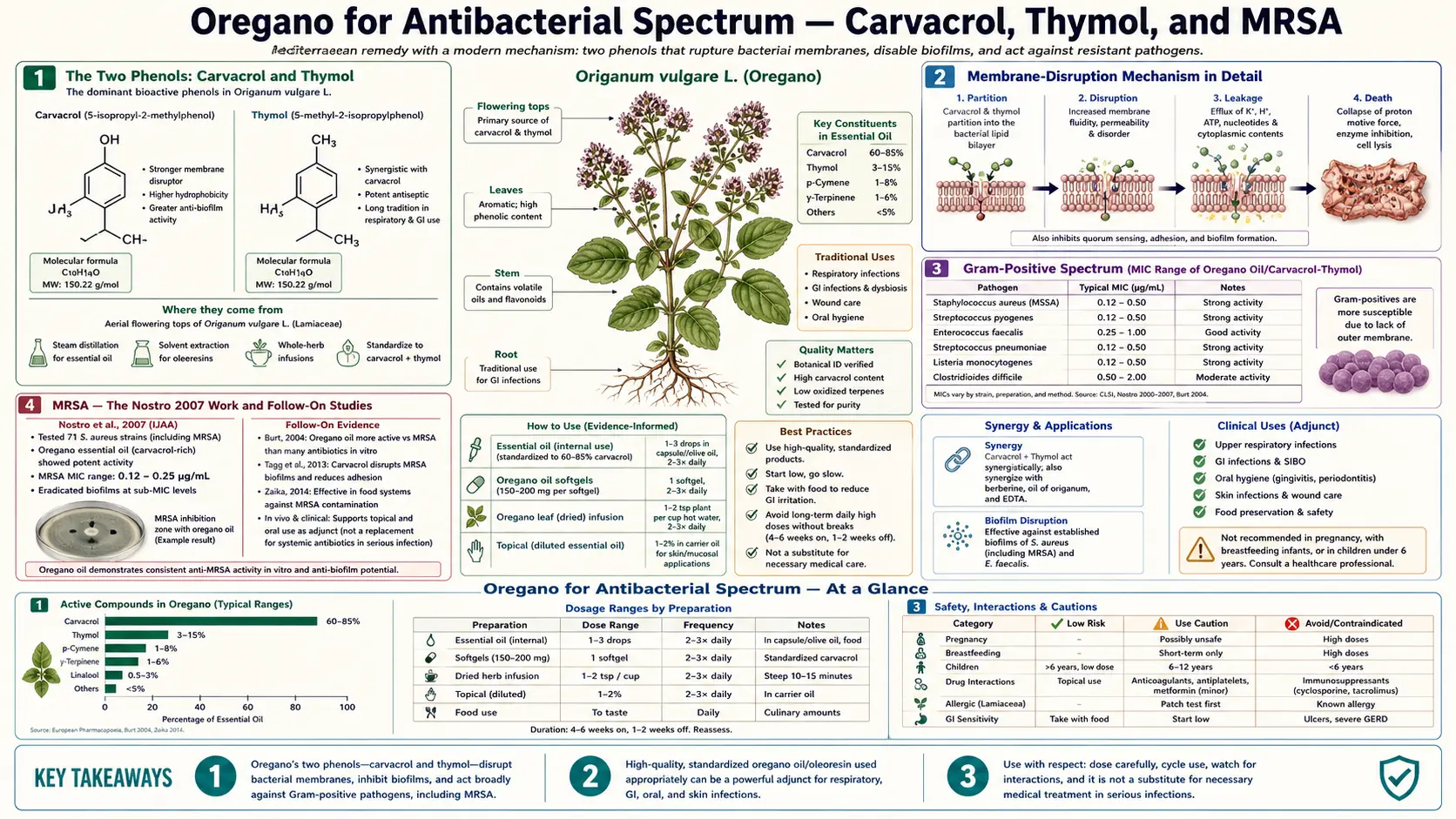
- Carvacrol (5-isopropyl-2-methylphenol) — the dominant compound, typically 50–80% of the essential oil of high-carvacrol chemotypes of Origanum vulgare ssp. hirtum (Greek oregano) and 60–75% of Origanum onites (Turkish oregano). The hydroxyl group is meta to the isopropyl. Carvacrol is the strongest of the two phenols in most in vitro activity assays.
- Thymol (2-isopropyl-5-methylphenol) — typically 1–30% of Origanum vulgare essential oil but the dominant compound in Thymus vulgaris (common thyme), where it can exceed 50%. The hydroxyl group is ortho to the isopropyl — the only structural difference from carvacrol. Activity is broadly comparable, with thymol slightly less potent than carvacrol against most Gram-positive bacteria.
The two compounds are typically present together and act synergistically — checkerboard MIC studies show fractional inhibitory concentration indices below 0.5 for many bacterial isolates when carvacrol and thymol are combined, indicating true synergy rather than mere addition. This is why the natural ratio in the essential oil tends to outperform purified single compounds at the same total phenolic concentration.
The total phenolic content varies dramatically by oregano source. Origanum vulgare ssp. hirtum (Greek oregano) and O. onites typically yield essential oils with 60–80% combined carvacrol-plus-thymol. The common European O. vulgare ssp. vulgare often has much lower phenolic content (10–30%) with non-phenolic monoterpenes like sabinene and beta-caryophyllene dominating, and correspondingly weaker antimicrobial activity. Mexican oregano (Lippia graveolens) is botanically distinct (in the Verbenaceae rather than Lamiaceae) but coincidentally produces a high-carvacrol essential oil with similar antimicrobial profile.
Membrane-Disruption Mechanism in Detail
The molecular mechanism of carvacrol and thymol against bacterial cells has been worked out in considerable detail and is one of the better-characterized natural-product antibacterial mechanisms. The sequence in a susceptible Gram-positive organism is:
- Partitioning into the lipid bilayer — carvacrol and thymol are sufficiently small and lipophilic to diffuse rapidly through the cell wall and partition into the phospholipid bilayer of the cytoplasmic membrane. They concentrate in the hydrocarbon-tail region near the membrane interior surface.
- Membrane fluidization and reorganization — the phenols disrupt the orderly packing of phospholipid acyl chains, increasing membrane fluidity and reducing the membrane's ability to maintain compositional asymmetry between inner and outer leaflets.
- Proton-motive force collapse — the disrupted membrane becomes leaky to protons. The cell can no longer maintain the transmembrane pH gradient and electrical potential that drive ATP synthesis by the membrane-bound F1F0-ATPase and most active transport. ATP levels fall rapidly.
- Ion and metabolite leakage — at higher phenol concentrations, the membrane becomes leaky to larger species. K+ and inorganic phosphate efflux is measurable within minutes. ATP itself begins to leak into the extracellular space.
- Death and lysis — the cell cannot maintain the osmotic gradient, the membrane can no longer support cell-wall biosynthesis, and the organism dies. In Gram-positives this typically proceeds to autolytic lysis as the dying cell's own murein hydrolases consume the cell wall.
In Gram-negative organisms an additional step is required: the outer membrane lipopolysaccharide layer must first be traversed. Carvacrol and thymol can do this, but less efficiently than they cross the inner membrane — this is the reason MIC values against Gram-negatives are typically 2- to 4-fold higher than against Gram-positives. The disrupting effect on the outer membrane LPS layer also sensitizes Gram-negatives to other agents that would normally be excluded; the well-documented synergy between oregano oil and conventional antibiotics in vitro is partly explained by this outer-membrane permeabilization.
The critical point is that no specific protein target is involved. The membrane lipid bilayer is the target, and there is no single-gene mutation that confers resistance the way that a single amino-acid substitution in a penicillin-binding protein, DNA gyrase, or fluoroquinolone target can confer resistance to conventional antibiotics. This is the mechanistic basis for oregano oil's continued activity against MRSA, VRE, and many multidrug-resistant Gram-negative organisms.
Gram-Positive Spectrum (Staph, Strep, Enterococcus)
Gram-positive bacteria are the most susceptible to oregano essential oil. Reported minimum inhibitory concentration (MIC) values for representative pathogens (high-carvacrol Greek oregano essential oil) cluster in the following ranges:
- Staphylococcus aureus (methicillin-sensitive) — MIC 0.025–0.05% v/v (~0.25–0.5 mg/mL)
- Staphylococcus aureus (methicillin-resistant, MRSA) — MIC 0.05–0.1% v/v (~0.5–1 mg/mL), only marginally higher than MSSA
- Staphylococcus epidermidis — MIC similar to S. aureus
- Streptococcus pyogenes — MIC 0.025–0.1% v/v
- Streptococcus pneumoniae — MIC 0.05–0.2% v/v
- Enterococcus faecalis (including vancomycin-resistant strains) — MIC 0.1–0.4% v/v
- Listeria monocytogenes — MIC 0.05–0.1% v/v
- Clostridium perfringens and C. difficile — MIC 0.1–0.4% v/v
- Bacillus cereus and B. subtilis — MIC 0.025–0.1% v/v
- Propionibacterium acnes (acne) — MIC 0.05–0.1% v/v
These values are bacteriostatic / bactericidal endpoints in artificial broth medium and do not translate directly to in vivo efficacy — oral oregano oil dilutes substantially in gut contents and is partly metabolized in the liver, and topical preparations face skin-barrier and biofilm penetration challenges. Nonetheless, the consistency of submilligram-per-milliliter MIC across Gram-positive pathogens is the empirical foundation for the use of oregano oil capsules in acne, in adjunct treatment of streptococcal pharyngitis, and in topical preparations for skin infections.
MRSA — The Nostro 2007 Work and Follow-On Studies
The most cited single paper on oregano oil and antibiotic-resistant Staphylococcus aureus is Nostro A et al. (2007) in Letters in Applied Microbiology, "Effects of Origanum vulgare essential oil on methicillin-resistant staphylococci." The Italian group tested commercially obtained Greek-oregano essential oil (~65% carvacrol, ~15% thymol) against panels of clinical MRSA isolates and reported:
- MIC values against MRSA clinical isolates fell in the 0.05–0.1% v/v range — essentially indistinguishable from MIC values against methicillin-sensitive S. aureus tested in parallel.
- Time-kill curves showed bactericidal activity (≥3 log10 CFU reduction) within 2–6 hours at concentrations of 1× to 2× MIC, consistent with rapid membrane disruption rather than slow growth inhibition.
- Pre-formed staphylococcal biofilms required 4- to 8-fold higher concentrations than planktonic cells for the same kill endpoint, reflecting the well-known biofilm resistance phenomenon, but the oil retained activity against biofilm at achievable concentrations.
- Sub-MIC concentrations of oregano oil reduced staphylococcal enterotoxin and hemolysin production, suggesting an additional anti-virulence effect beyond simple bactericidal activity.
Multiple follow-on studies have replicated the Nostro findings using oregano oils of varying chemotype, generally confirming that the carvacrol+thymol content predicts the anti-MRSA activity. Manohar V et al. (2001) had earlier reported in vivo activity in a murine systemic candidiasis model using a similar Greek oregano oil, providing the first in vivo confirmation that orally administered oregano oil reaches concentrations capable of antimicrobial activity in tissue.
The clinical limitation is that no large randomized controlled trial of oral oregano oil in human MRSA infection has been published. The available human evidence is limited to small case series, anecdotal reports, and the indirect evidence from the use of oregano oil capsules in chronic skin infections, recurrent boils, and as an adjunct to topical mupirocin in decolonization regimens. In vitro and in vivo animal data are robust; well-powered human RCT data are not. For more on MRSA and antibiotic resistance generally, see our Staphylococcus aureus / MRSA page and the Antibacterial Herbs overview.
Gram-Negative Spectrum (E. coli, Salmonella, Pseudomonas, Klebsiella)
Gram-negative organisms are less susceptible than Gram-positives because of the outer-membrane lipopolysaccharide barrier, but oregano essential oil retains useful activity against most Enterobacterales pathogens and against many Pseudomonas isolates. Representative MIC ranges:
- Escherichia coli (including enterotoxigenic and Shiga-toxin-producing strains) — MIC 0.1–0.4% v/v
- Salmonella enterica (typhimurium, enteritidis) — MIC 0.1–0.4% v/v
- Klebsiella pneumoniae — MIC 0.1–0.5% v/v, including some ESBL-producing strains
- Pseudomonas aeruginosa — MIC 0.2–0.8% v/v — less susceptible than Enterobacterales but still inhibited at achievable concentrations
- Helicobacter pylori — MIC 0.05–0.2% v/v, supporting the traditional use as adjunct to triple therapy
- Campylobacter jejuni — MIC 0.05–0.2% v/v
- Vibrio cholerae — MIC 0.1–0.2% v/v
- Yersinia enterocolitica — MIC 0.1–0.4% v/v
The combination of activity against both Gram-positive and Gram-negative gut pathogens is what underlies the broad traditional use of oregano oil for gastroenteritis and traveler's diarrhea in Mediterranean and Hispanic folk medicine. The in vitro evidence supports the empirical practice, though again no large human RCT in acute gastroenteritis has been published. See also the parallel coverage of intestinal parasites and SIBO in our Antiparasitic and SIBO deep-dive.
Oral Candidiasis Pilot (Antibacterial Crossover)
A small open-label pilot study (Manohar 2001 and several subsequent open-label series) examined oregano oil capsules (typically 600–1200 mg/day of emulsified oil delivering 200–400 mg/day of carvacrol) for oral candidiasis (thrush) in immunocompetent and mildly immunocompromised adults. The pilot enrolled patients with culture-confirmed Candida albicans thrush, dosed oregano oil capsules orally for 30–60 days, and reported clinical resolution of visible thrush and symptomatic relief in the majority of patients, with mycological clearance documented in roughly 60–70% at the end of treatment.
While the principal target organism is fungal (covered in detail on the Antifungal deep-dive), the relevance to the antibacterial spectrum is that oral candidiasis frequently co-exists with shifts in the oral bacterial microbiome (overgrowth of Streptococcus mutans, Lactobacillus, anaerobes) that may contribute to recurrence after antifungal-only therapy. Oregano oil's combined antibacterial-plus-antifungal action is hypothesized to address both the Candida and the dysbiotic bacterial overgrowth simultaneously, possibly explaining why clinical response in the pilots appeared comparable to nystatin despite a less specific antifungal mechanism.
The pilot data are small, open-label, and without rigorous controls. They should be interpreted as hypothesis-generating rather than as definitive efficacy evidence. They do, however, demonstrate that the oral oregano-oil regimen used in commercial supplements (~600–1200 mg/day) can produce clinically detectable antimicrobial activity in human oropharyngeal tissue at a dose that is well tolerated.
"Oil of Oregano" vs Essential Oil vs Culinary Oregano — Concentrations
The three commercially available forms of oregano differ by 100- to 1000-fold in carvacrol content per dose, and confusion between them is the single most common cause of either ineffective treatment or accidental mucosal burn. The hierarchy:
- Culinary dried oregano leaf — ~1–3% essential oil by weight; carvacrol content perhaps 0.5–2% of leaf mass. A heaping teaspoon (~2 g) of dried leaf contains perhaps 10–40 mg of carvacrol. Pleasant culinary doses do not reach systemic antimicrobial concentrations — oregano leaf in food is a culinary herb, not a pharmacologic dose.
- "Oil of oregano" (carrier-diluted) — the dominant commercial supplement form, sold in soft-gel capsules or in dropper bottles. Composition is essential oil emulsified in a carrier oil (typically olive oil, MCT/coconut oil, extra-virgin olive oil), at concentrations ranging from 10–30% essential oil. Typical capsule contents 150–500 mg of mixture delivering 30–150 mg of essential oil per capsule, of which 20–100 mg is carvacrol+thymol. Standard dosing 1–3 capsules per day for short courses (5–14 days).
- Pure essential oil (undiluted) — the most concentrated form, sold as a steam-distilled essential oil at 60–80% carvacrol+thymol. A single drop contains ~20–30 mg of carvacrol — equivalent to a typical oil-of-oregano supplement capsule. This form is caustic to oral and esophageal mucosa and must never be taken neat by mouth. Standard practice is to dilute one drop in 1 teaspoon of olive or coconut oil before oral use, or to use the diluted preparation topically (on intact skin) only after a 1:4 or greater dilution in carrier oil.
The clinical translation: most published antimicrobial trials use the "oil of oregano" form (carrier-diluted, capsule or dropper) at doses delivering 30–200 mg/day of carvacrol. Culinary oregano does not reach this dose. Pure essential oil reaches it in one or two drops but cannot be safely consumed undiluted. The next section discusses the proprietary P73 formulation in detail.
The P73 Carvacrol-Standardized Formulation
P73 is a proprietary high-carvacrol wild Mediterranean oregano essential oil sourced and standardized by Cass Ingram's North American Herb & Spice company. The name "P73" originally referred to a specific wild oregano harvest from the Mediterranean, characterized by very high carvacrol content (typically 70–80% carvacrol) achieved by blending oils from Origanum vulgare ssp. hirtum with related wild Origanum species at carefully controlled ratios. The "P73" designation has subsequently been used both as the trademark name for the commercial product (sold as "Oreganol P73") and informally as a generic shorthand for any high-carvacrol Mediterranean oregano oil at this carvacrol fraction.
The published research that has used the P73 product (or similar high-carvacrol Mediterranean oils) is the basis for much of the modern English-language oregano-oil literature, including Manohar V et al. (2001) on Candida albicans, the Force 2000 enteric parasite trial (covered on the Antiparasitic and SIBO deep-dive), and several open-label clinical series on chronic sinusitis, recurrent skin infections, and gut dysbiosis. The clinical relevance is that any oregano oil supplement claiming to match the P73 evidence should specify a carvacrol content of at least 60–70% on the label or in the COA — lower-carvacrol oregano oils (common from European O. vulgare ssp. vulgare) will not replicate the published efficacy.
Cautionary note: the P73 brand and Cass Ingram's broader work have at times been associated with promotional claims that exceed the published evidence (treatment of viral infections, severe systemic disease, and so on). The mechanistic and in vitro evidence for broad antimicrobial activity is solid; the clinical evidence for serious systemic infection is anecdotal and should not displace conventional antimicrobial therapy in life-threatening disease. For more on the broader debate over antibiotic stewardship and alternatives, see our Antibacterial Herbs overview.
Dosing and Dilution Requirements
Recommended dosing depends on the form:
- Oil of oregano capsules (10–30% essential oil in carrier) — 1–3 capsules per day with food, for 5–14 days for acute infection. Each capsule typically delivers 30–100 mg of essential oil. Taking with food reduces nausea and reflux.
- Liquid oil-of-oregano (10–30% in dropper bottle) — 2–4 drops in a teaspoon of olive oil or in a vegetable capsule, 2–3 times per day. The taste is intensely sharp and pepperish; mixing into a carrier oil improves tolerability.
- Pure essential oil (60–80% carvacrol) — dilute one drop in a teaspoon of olive or coconut oil before any oral use. Do not exceed 1–2 drops twice daily for short courses. For topical use, dilute at minimum 1:4 in carrier oil (one drop essential oil to four drops carrier).
- Culinary leaf — no specific dose; routine culinary use (sprinkling on tomato dishes, lamb, Mediterranean salads) contributes dietary polyphenols and a small carvacrol dose, but is not a pharmacologic intervention.
Duration of use should generally be limited to 14 days at a time for systemic antimicrobial purposes — longer continuous use risks disrupting commensal gut flora in ways comparable to broad-spectrum antibiotics. Cycling 14 days on / 14 days off, or pulsing for 5 days at a time, is a common practical approach.
Cautions, Drug Interactions, and Mucosal-Burn Risk
- Mucosal burn from undiluted essential oil — the most consequential acute risk. Undiluted carvacrol applied to oral, esophageal, or gastric mucosa produces a chemical burn comparable to undiluted clove or cinnamon oil. Always dilute pure essential oil at minimum 1:4 in carrier oil before any oral or mucosal contact. Inadvertent neat ingestion has produced esophageal ulceration in case reports.
- Skin sensitization — topical pure essential oil can produce contact dermatitis, particularly with repeated use. Patch test on the inner forearm before broader application. Avoid use on broken, eczematous, or burned skin.
- Pregnancy and lactation — oral oregano oil supplements should be avoided in pregnancy due to limited safety data and theoretical uterine-stimulant effect of high-dose carvacrol. Culinary doses of oregano leaf are safe; supplemental doses are not.
- Anticoagulant and antiplatelet interaction — oregano oil has documented in vitro platelet-inhibitory effects. Caution with concurrent warfarin, apixaban, rivaroxaban, clopidogrel, aspirin. Avoid for two weeks before scheduled surgery.
- Diabetes medications — carvacrol has mild hypoglycemic activity in some animal studies; monitor blood glucose if combining with insulin or sulfonylureas.
- Iron absorption — phenolic compounds bind nonheme iron and may reduce absorption. Take iron supplements at least 2 hours separated from oregano oil.
- Disruption of commensal gut microbiome — the same broad antimicrobial spectrum that inhibits pathogens also inhibits commensal Lactobacillus, Bifidobacterium, and other beneficial gut bacteria. Pair extended oral oregano oil use with a probiotic taken at least 4–6 hours separated in time, and consider a structured gut-healing protocol after a course.
- Allergy — cross-reactivity is possible in patients with documented allergy to other Lamiaceae family herbs (basil, mint, sage, thyme, rosemary, marjoram).
- Children — oral oregano oil supplements are not recommended for children under 12 except under clinician supervision. Culinary leaf is safe at any age.
- Not a substitute for conventional antibiotics in serious infection — despite the in vitro MRSA activity, oregano oil should not displace appropriate antibiotic therapy for life-threatening or invasive bacterial infection. Its evidence base supports adjunctive and limited primary use in low-acuity settings (skin infection, gut dysbiosis, mild oropharyngeal infection); it does not yet support primary monotherapy for systemic disease.
Key Research Papers
- Nostro A et al. (2007). Effects of Origanum vulgare essential oil on methicillin-resistant staphylococci. Letters in Applied Microbiology. — PubMed
- Manohar V et al. (2001). Antifungal activities of origanum oil against Candida albicans. Molecular and Cellular Biochemistry. — PubMed
- Burt S (2004). Essential oils: their antibacterial properties and potential applications in foods — a review. International Journal of Food Microbiology. — PubMed
- Lambert RJW et al. (2001). A study of the minimum inhibitory concentration and mode of action of oregano essential oil, thymol and carvacrol. Journal of Applied Microbiology. — PubMed
- Ultee A et al. (2002). The phenolic hydroxyl group of carvacrol is essential for action against Bacillus cereus. Applied and Environmental Microbiology. — PubMed
- Friedman M, Henika PR, Mandrell RE (2002). Bactericidal activities of plant essential oils and some of their isolated constituents against Campylobacter jejuni, Escherichia coli, Listeria monocytogenes, and Salmonella enterica. Journal of Food Protection. — PubMed
- Chouhan S, Sharma K, Guleria S (2017). Antimicrobial activity of some essential oils — present status and future perspectives. Medicines. — PubMed
- Si W et al. (2006). Antimicrobial activity of essential oils and structurally related synthetic food additives towards selected pathogenic and beneficial gut bacteria. Journal of Applied Microbiology. — PubMed
- Helander IM et al. (1998). Characterization of the action of selected essential oil components on Gram-negative bacteria. Journal of Agricultural and Food Chemistry. — PubMed
- Preuss HG et al. (2005). Minimum inhibitory concentrations of herbal essential oils and monolaurin for Gram-positive and Gram-negative bacteria. Molecular and Cellular Biochemistry. — PubMed
- Sienkiewicz M et al. (2012). The antibacterial activity of oregano essential oil against clinical strains of Escherichia coli and Pseudomonas aeruginosa. Medycyna Doswiadczalna i Mikrobiologia. — PubMed
- Cui H et al. (2019). Antibacterial activity and mechanism of Chuzhou chrysanthemum essential oil. Journal of Functional Foods — carvacrol mechanism comparison. — PubMed
PubMed Topic Searches
- PubMed: Origanum vulgare antimicrobial
- PubMed: Carvacrol MRSA
- PubMed: Oregano oil Gram-negative
- PubMed: Carvacrol/thymol membrane disruption
- PubMed: Oregano oil and antibiotic resistance
Connections
- Oregano Overview
- Oregano Benefits Hub
- Oregano Antifungal
- Oregano Antiparasitic & SIBO
- Oregano Antioxidant & Respiratory
- Antibacterial Herbs
- Thyme (thymol)
- Garlic
- Olive Leaf
- Berberine
- Neem
- Staphylococcus aureus / MRSA
- Acne (P. acnes)
- Urinary Tract Infections
- Pneumonia
- Gut Healing
- All Herbs