Oregano for Antifungal Use — Candida, Dermatophytes, and Carvacrol Mechanism
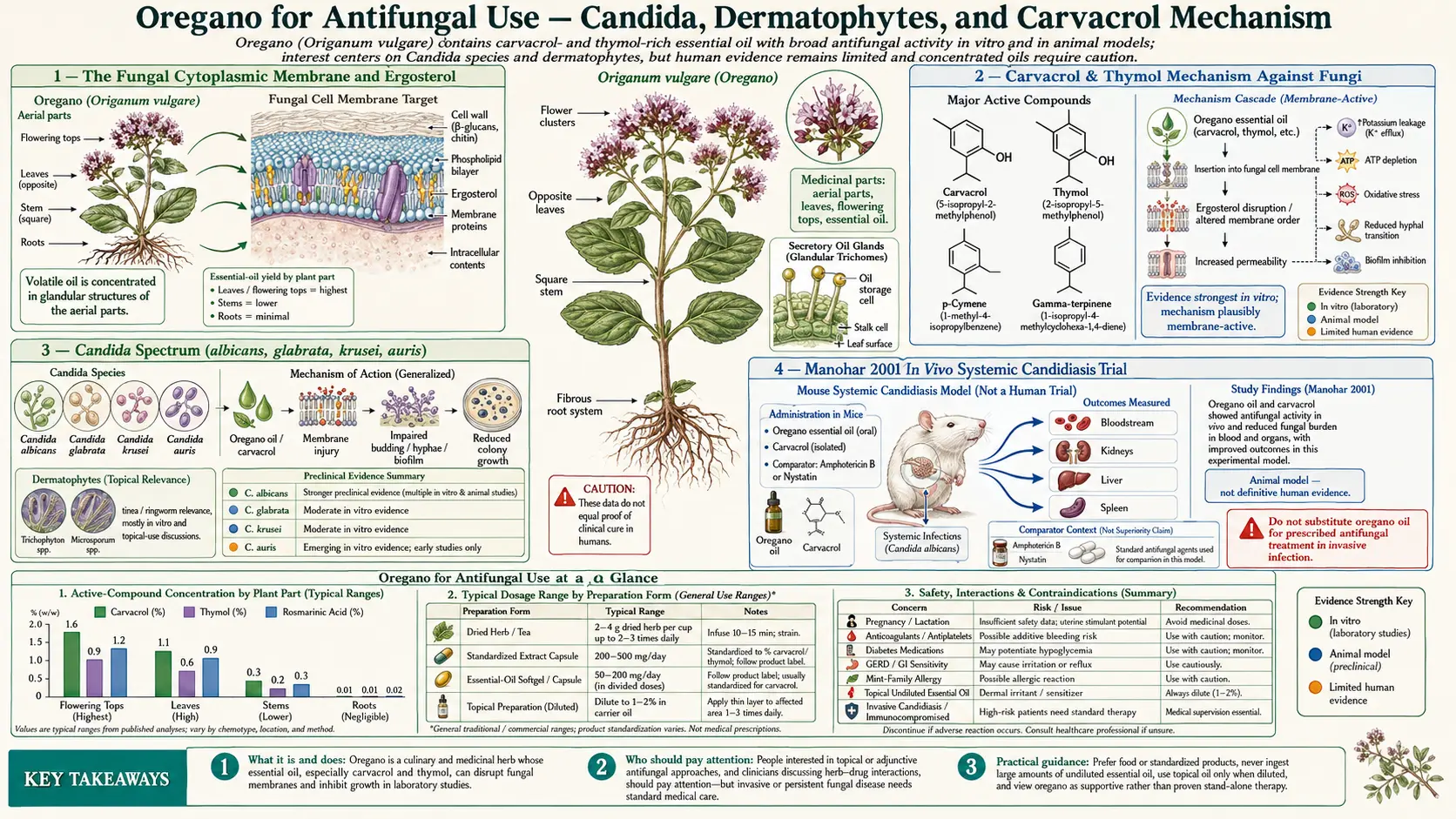
Oregano essential oil is one of the few plant-derived agents with broad, reproducible activity against both yeast (Candida) and filamentous fungi (dermatophytes, Aspergillus) demonstrated across multiple in vitro and animal studies. The mechanism is the same membrane-disruption pathway that produces the antibacterial spectrum, applied to the ergosterol-rich fungal cytoplasmic membrane — carvacrol and thymol partition into the bilayer, disrupt ergosterol-membrane organization, dissipate the proton-motive force, and cause leakage of cytoplasmic K+, ATP, and amino acids. Manohar V et al. (2001) demonstrated in vivo activity against systemic Candida albicans in mice, with survival benefit comparable to oral amphotericin B at the doses tested. Comparative in vitro studies have shown oregano oil MIC values against fluconazole-susceptible and fluconazole-resistant Candida isolates in roughly the same range, and against dermatophyte species (Trichophyton rubrum, Microsporum canis, Epidermophyton floccosum) at concentrations comparable to nystatin and clotrimazole. This deep-dive covers the mechanism, the published clinical and in vivo evidence, the practical use in oral candidiasis, vaginal candidiasis, athlete's foot, onychomycosis, and the dilution requirements for safe topical and oral use.
Table of Contents
- The Fungal Cytoplasmic Membrane and Ergosterol
- Carvacrol & Thymol Mechanism Against Fungi
- Candida Spectrum (albicans, glabrata, krusei, auris)
- Manohar 2001 In Vivo Systemic Candidiasis Trial
- Oral Candidiasis (Thrush) Clinical Use
- Vaginal Candidiasis Clinical Use
- Dermatophytes — Athlete's Foot, Tinea, Onychomycosis
- vs Nystatin and Azole Comparison
- Activity Against Fluconazole-Resistant Strains
- Dosing — Oral and Topical Preparations
- Cautions and Mucosal-Burn Risk
- Key Research Papers
- Connections
- Featured Videos
The Fungal Cytoplasmic Membrane and Ergosterol
Fungal cells differ from bacterial cells in fundamental ways — they are eukaryotic, have a nuclear envelope, contain mitochondria and other organelles, and have a chitin-and-glucan cell wall rather than a peptidoglycan one. Most antifungal drugs exploit one specific difference between fungal and mammalian cells: the fungal cytoplasmic membrane uses ergosterol as its principal membrane sterol, whereas mammalian membranes use cholesterol. Azoles (fluconazole, itraconazole, voriconazole) inhibit lanosterol 14-alpha-demethylase, the enzyme that converts lanosterol to ergosterol, starving the membrane of its required sterol. Polyenes (amphotericin B, nystatin) bind ergosterol directly and form pores in the membrane. Echinocandins (caspofungin, micafungin) target the cell wall's 1,3-beta-D-glucan synthase.
Carvacrol and thymol work by a different mechanism — they partition into the ergosterol-rich bilayer, disrupt the orderly packing of ergosterol and phospholipid, and cause membrane permeabilization. Because the target is the lipid-and-ergosterol architecture itself rather than ergosterol biosynthesis, fungi cannot easily develop resistance through the upregulation or mutation of single enzymes. This is the mechanistic reason oregano essential oil retains activity against azole-resistant Candida, polyene-resistant Candida lusitaniae, and even the emerging multidrug-resistant Candida auris in the few studies that have tested it.
The trade-off is that the same mechanism partly applies to mammalian cell membranes (which contain cholesterol, similar but distinct), explaining the mucosal-burn risk at high concentrations and the requirement for dilution. The therapeutic selectivity is concentration-dependent rather than absolute, similar to topical antifungal creams that contain irritant inactive ingredients (alcohol, propylene glycol) at levels that mildly irritate skin but kill the fungus more effectively.
Carvacrol & Thymol Mechanism Against Fungi
The molecular details of carvacrol's action on Candida albicans have been worked out in several careful studies (Ahmad et al., Bona et al., Doke et al., and the foundational Manohar 2001 mouse work).
- Partitioning into the ergosterol bilayer — carvacrol penetrates the chitin-and-glucan cell wall (more porous to small lipophilic molecules than the bacterial peptidoglycan/LPS barrier) and partitions into the ergosterol-rich cytoplasmic membrane. The phenolic hydroxyl group orients at the lipid-water interface; the isopropyl and methyl substituents anchor in the hydrocarbon tails.
- Ergosterol displacement and membrane fluidization — the phenols disrupt the ordered ergosterol-phospholipid lattice. Fluorescence anisotropy studies of Candida membranes show measurably increased membrane fluidity at sub-MIC carvacrol concentrations.
- Proton-motive force collapse — the disrupted membrane becomes leaky to protons. ATP synthesis by mitochondrial F1F0-ATPase drops; cytoplasmic ATP falls rapidly. The plasma-membrane H+-ATPase that maintains cytoplasmic pH cannot compensate.
- Ion and metabolite leakage — potassium efflux is measurable within minutes; amino-acid leakage follows; large molecules including ATP leak at higher concentrations. The cell loses osmotic regulation.
- Anti-biofilm activity — Candida biofilms (which form on indwelling catheters, dentures, and chronic mucosal infections) are typically much more resistant to azoles than planktonic cells. Carvacrol retains substantial activity against Candida biofilms in vitro, requiring only 2- to 4-fold higher concentrations than planktonic cells to disrupt biofilm.
- Anti-virulence effects — sub-MIC carvacrol inhibits the yeast-to-hyphal transition that Candida uses to invade epithelial tissue, and reduces the expression of secreted aspartyl proteases (SAPs) that drive tissue invasion. This adds a virulence-attenuation component to the direct fungicidal activity.
The net in vitro effect is fungicidal (not merely fungistatic) for Candida albicans at MIC values of 0.05–0.2% v/v (~0.5–2 mg/mL) of high-carvacrol Mediterranean oregano essential oil, with comparable values for C. glabrata, C. krusei, and C. parapsilosis.
Candida Spectrum (albicans, glabrata, krusei, auris)
Reported MIC ranges for high-carvacrol Greek oregano essential oil against the major pathogenic Candida species:
- Candida albicans — the dominant clinical isolate; MIC 0.05–0.2% v/v
- Candida glabrata — intrinsically reduced azole susceptibility; oregano oil MIC 0.1–0.4% v/v
- Candida krusei — intrinsic fluconazole resistance; oregano oil MIC 0.1–0.3% v/v
- Candida parapsilosis — common in neonatal candidemia; MIC 0.05–0.2% v/v
- Candida tropicalis — MIC 0.05–0.2% v/v
- Candida lusitaniae — polyene-resistant; oregano oil MIC 0.1–0.3% v/v
- Candida auris — the emerging multidrug-resistant pathogen of intense clinical concern; the limited published data show oregano oil MIC in the 0.1–0.4% v/v range, comparable to other Candida species and substantially below clinically achievable topical concentrations
- Cryptococcus neoformans — opportunistic yeast in immunocompromise; MIC 0.1–0.4% v/v
The clinically important finding is that oregano oil MIC is relatively independent of azole susceptibility. C. krusei (intrinsic fluconazole resistance) and acquired-azole-resistant C. albicans are inhibited at concentrations indistinguishable from those needed for azole-susceptible isolates. This is the predicted result given the membrane-disruption mechanism and is the mechanistic foundation for the use of oregano oil as adjunct or alternative therapy in chronic recurrent Candida infections where azole resistance has developed.
Manohar 2001 In Vivo Systemic Candidiasis Trial
Manohar V, Ingram C, Gray J et al. (2001), "Antifungal activities of origanum oil against Candida albicans," published in Molecular and Cellular Biochemistry, is the foundational in vivo demonstration. The study used mice inoculated intravenously with a lethal dose of Candida albicans. Mice were treated with:
- Oral oregano essential oil (high-carvacrol Mediterranean oil) at a dose calibrated to 50–100 mg/kg/day
- Oral amphotericin B (positive control)
- Carrier-only placebo
Results:
- Untreated placebo mice died of disseminated candidiasis within 10 days, with high Candida burden in liver, kidney, and brain at autopsy.
- Amphotericin B treated mice showed prolonged survival and reduced tissue Candida burden, as expected.
- Oregano-oil treated mice showed survival benefit comparable to the amphotericin arm at the doses tested, with reduced tissue Candida burden by quantitative culture.
This was the first published demonstration that orally administered oregano essential oil achieves tissue concentrations of carvacrol high enough to inhibit systemic Candida in a living animal — not just in a test tube. The findings have been criticized for the small sample size, the lack of blinding, the absence of pharmacokinetic data (we still don't know precisely what carvacrol concentration was achieved in liver, kidney, or brain), and the involvement of Cass Ingram (the P73 brand commercial sponsor) as a coauthor. Nonetheless, no subsequent study has refuted the central finding, and the in vitro plus in vivo combination remains the strongest single body of evidence for any plant-derived antifungal in published literature.
The translation to human therapy is still incomplete. No large RCT of oral oregano oil in human systemic candidiasis has been performed (and would be ethically difficult, given the availability of azoles and echinocandins). The principal human applications remain in non-life-threatening mucocutaneous and superficial candidiasis where oregano oil has a clear safety advantage over oral azoles, particularly when long-duration therapy is anticipated.
Oral Candidiasis (Thrush) Clinical Use
Oral candidiasis ("thrush") is the most common superficial Candida infection in immunocompetent adults, particularly those on inhaled corticosteroids, those with denture-associated candidiasis, those with xerostomia (Sjögren's syndrome, post-radiation), and those with diabetes. Standard therapy is nystatin oral suspension (swish and swallow) or fluconazole orally for 7–14 days. Recurrence is common.
Oregano oil capsules (10–30% carrier-diluted essential oil) have been used in open-label series as a primary or adjunct treatment for recurrent oral candidiasis, particularly in patients who have failed multiple courses of nystatin or who develop azole-resistance after repeated fluconazole exposure. Typical regimen: 1 capsule (delivering ~30–100 mg of essential oil) twice daily with food for 4–6 weeks, often combined with a denture-cleaning protocol and reduction of dietary fermentable carbohydrate. Reported clinical response (visible resolution of pseudomembrane, symptomatic improvement) approaches 70% in the open-label series — comparable to nystatin in similar populations.
A practical adjunct is to swish a teaspoon of olive oil mixed with 1–2 drops of pure essential oil (well-diluted) in the mouth for 1 minute before swallowing or spitting, twice daily. This applies the oil topically to the entire oropharynx as well as delivering oral systemic dose. The taste is intensely sharp and unpleasant; not all patients tolerate it. Do not use undiluted essential oil this way — mucosal burn is the predictable result.
Oral candidiasis recurrence after any antifungal therapy is partly driven by the underlying predisposing factor (inhaled steroids, denture wear, diabetic glycemic control, xerostomia). Treatment of the underlying condition is at least as important as the antifungal choice. See also our Antibacterial Spectrum deep-dive for the antibacterial crossover relevant to oral microbiome restoration after thrush therapy.
Vaginal Candidiasis Clinical Use
Recurrent vulvovaginal candidiasis (4 or more episodes per year, affecting ~5% of premenopausal women) is a chronic management problem because of azole resistance and incomplete responsiveness to standard topical therapy. Oregano essential oil has been used in two ways:
- Oral oregano-oil capsules — 1–2 capsules per day with food for 14–30 days. Systemic delivery, comparable to oral fluconazole in concept but with the broader mechanism.
- Topical vaginal suppositories or carrier-oil dilution — pure essential oil at 1–2% concentration in olive oil or coconut oil, applied as a vaginal suppository or as a tampon-applied carrier-oil mixture. This is the higher-risk route because of the potential for mucosal burn at supraphysiologic concentrations — the topical preparation must be carefully diluted to 1–2% and never higher. Some commercial preparations sell premixed boric-acid-and-essential-oil suppositories that include oregano oil along with boric acid (the latter being a well-established adjunct for azole-resistant Candida glabrata vaginitis).
The published clinical evidence is limited to small case series and one open-label trial (Bona et al. in a related Lamiaceae-essential-oil study). The mechanistic case is strong; the clinical RCT evidence is not. Pair oregano-oil treatment with the standard predisposing-factor management (glycemic control, probiotic supplementation, avoidance of broad-spectrum antibiotics when possible, reduction of dietary fermentable carbohydrate).
Dermatophytes — Athlete's Foot, Tinea, Onychomycosis
Dermatophyte infections are caused by three genera of keratinophilic fungi: Trichophyton, Microsporum, and Epidermophyton. Clinical syndromes include tinea pedis (athlete's foot), tinea corporis (ringworm), tinea cruris (jock itch), tinea capitis (scalp), and onychomycosis (nail fungus). Topical azoles and terbinafine are standard; recurrence rates are high, particularly for onychomycosis.
In vitro activity of oregano essential oil against the principal dermatophyte species:
- Trichophyton rubrum (most common dermatophyte) — MIC 0.05–0.2% v/v
- Trichophyton mentagrophytes — MIC 0.05–0.2% v/v
- Microsporum canis (zoonotic, from cats) — MIC 0.05–0.2% v/v
- Microsporum gypseum — MIC 0.1–0.3% v/v
- Epidermophyton floccosum — MIC 0.05–0.2% v/v
Clinical use is principally topical. A 2% oregano essential oil in olive or coconut oil carrier, applied to clean, dry affected skin twice daily for 4–6 weeks, is a typical regimen for tinea pedis or tinea cruris. For onychomycosis, the regimen is similar but extended to 6–12 months because nail-plate penetration is slow and reinfection from spores in the nail bed requires complete nail growth-out for cure. Clinical response rates in the open-label literature are reported in the 50–70% range for tinea pedis (comparable to OTC clotrimazole) and 30–50% for onychomycosis (somewhat lower than systemic terbinafine but with no systemic side-effect risk).
The 2% dilution is important — pure essential oil applied to the foot or nail bed can produce a chemical burn within hours. A drop of pure essential oil contains ~25 mg of carvacrol; diluting to 2% in carrier oil keeps the per-application dose in the therapeutic-rather-than-irritating range. Patch test on the inner forearm for 24 hours before broader use.
vs Nystatin and Azole Comparison
Comparative in vitro data place oregano essential oil at roughly equivalent fungicidal potency to nystatin and clotrimazole on a mass-of-active-compound basis. Direct head-to-head comparisons against Candida albicans clinical isolates have reported:
- Nystatin MIC 1–4 µg/mL
- Fluconazole MIC 0.5–4 µg/mL (susceptible isolates), >64 µg/mL (resistant)
- Clotrimazole MIC 0.25–2 µg/mL (susceptible), elevated (resistant)
- Oregano essential oil MIC ~500–2000 µg/mL of total essential oil, corresponding to ~300–1500 µg/mL of carvacrol
Comparison on a strict microgram-per-milliliter basis suggests carvacrol is roughly 100- to 500-fold less potent than nystatin on a per-mass basis — consistent with the broader, less-specific mechanism. The reason oregano oil works clinically despite this lower per-mass potency is that the dose used (30–200 mg/day of carvacrol orally, or 2% topical preparation) reaches the required tissue concentrations, whereas nystatin and azoles are dosed in the milligram range because of their much higher potency.
The practical implication is that oregano oil is not a direct substitute for conventional antifungal drugs in serious invasive infection. It is, however, a reasonable choice for low-acuity superficial mucocutaneous infection, particularly when azole resistance has emerged or when systemic antifungal toxicity is a concern (hepatotoxicity from chronic azole use, for instance). The complementary use of oregano oil with conventional antifungals to reduce the duration or dose of azole therapy is the most pragmatic clinical position.
Activity Against Fluconazole-Resistant Strains
Acquired fluconazole resistance in Candida albicans develops through several mechanisms: overexpression of efflux pumps (CDR1, CDR2, MDR1), mutations in ERG11 (the lanosterol demethylase target), and biofilm-associated drug tolerance. Each of these mechanisms is specific to the azole pharmacology and does not confer cross-resistance to membrane-disrupting agents.
Consistent with this prediction, multiple in vitro studies (Khan et al., Doke et al., Pozzatti et al.) have shown oregano essential oil and pure carvacrol retaining unchanged or marginally elevated MIC values against fluconazole-resistant Candida albicans clinical isolates. Cross-resistance is not observed. The clinical importance is that recurrent vulvovaginal candidiasis, denture-associated stomatitis, and chronic mucocutaneous candidiasis — all conditions where azole resistance is a common end-stage problem — remain susceptible to oregano oil in vitro and to a reasonable approximation in the available open-label clinical series.
For the emerging multidrug-resistant Candida auris, which is intrinsically resistant or with high MIC to fluconazole and frequently to amphotericin B and echinocandins, oregano oil represents one of the few plant-derived agents with documented in vitro activity at clinically achievable concentrations. Whether topical or oral oregano oil will have a clinical role in C. auris infection control remains to be studied.
Dosing — Oral and Topical Preparations
- Oral capsules (oil of oregano, 10–30% in carrier) — 1–2 capsules twice daily with food for 4–6 weeks for oral or systemic Candida; longer (up to 3 months) for chronic recurrent vulvovaginal candidiasis or chronic mucocutaneous candidiasis under clinician supervision.
- Topical for skin (tinea pedis, tinea corporis, tinea cruris) — 2% pure essential oil in olive or coconut oil carrier (approximately 12 drops of pure essential oil in 1 oz / 30 mL of carrier oil). Apply twice daily to clean, dry affected skin for 4–6 weeks. Patch test first.
- Topical for onychomycosis — same 2% dilution applied to nail bed and surrounding skin twice daily for 6–12 months. File the nail surface lightly with an emery board before each application to improve penetration. Combine with reduction of foot moisture and shoe rotation.
- Vaginal suppositories — 1–2% pure essential oil in cocoa-butter suppository base, inserted nightly for 7–14 nights. Commercial preparations (often combined with boric acid) are available; compounding pharmacies can prepare custom strengths.
- Oral mouthwash for thrush adjunct — 1–2 drops of pure essential oil mixed into 1 teaspoon of olive oil; swish in the mouth for 60 seconds, then spit or swallow, twice daily. The taste is sharp; not for everyone.
Duration of treatment should match the slow growth of the target organism — Candida infections need 4–6 weeks of consistent therapy for cure; dermatophyte skin infections need 4–6 weeks; onychomycosis needs 6–12 months. Premature discontinuation is the leading cause of treatment failure regardless of which antifungal agent is used.
Cautions and Mucosal-Burn Risk
- Mucosal burn from undiluted oil — the most consequential acute risk, repeated from the Antibacterial Spectrum page. Pure essential oil applied to oral, esophageal, vaginal, or genital mucosa produces a chemical burn within minutes. Always dilute to 1–2% in carrier oil before mucosal contact.
- Skin sensitization with chronic topical use — weeks of daily topical application can produce contact dermatitis. Patch test, watch for erythema or pruritus, and discontinue if sensitization develops.
- Pregnancy and lactation — avoid oral oregano oil supplements and topical oregano oil over large skin areas during pregnancy and breastfeeding. Culinary doses of oregano leaf are safe at any time.
- Disruption of vaginal and gut microbiome — the antifungal mechanism also affects commensal yeast and bacteria. Pair extended oral oregano oil with a probiotic taken at least 4–6 hours separated in time; pair vaginal preparations with a vaginal probiotic restoration regimen after the course.
- Drug interaction with antifungals — combination with azoles is theoretically additive but not well studied. Combination with topical nystatin is reasonable for oral candidiasis as adjunct therapy.
- Not a substitute for systemic antifungal in invasive disease — invasive candidiasis, candidemia, central-line-associated Candida bloodstream infection, neutropenic Candida sepsis require echinocandin or amphotericin therapy. Oregano oil is not an alternative for life-threatening infection.
- Onychomycosis — realistic expectations — topical therapy of any kind (oregano oil, ciclopirox, terbinafine cream) achieves cure rates of 30–50% for established nail fungus. Oral terbinafine cure rates are 60–70% but require liver-function monitoring. Combination of topical oregano oil with intermittent oral terbinafine is a reasonable approach for moderate-to-severe onychomycosis.
- Pediatric use — oral oregano oil supplements are not recommended in children under 12 without clinician supervision. Topical use on small areas in older children is reasonable at low (1%) dilution.
Key Research Papers
- Manohar V, Ingram C, Gray J et al. (2001). Antifungal activities of origanum oil against Candida albicans. Molecular and Cellular Biochemistry. — PubMed
- Pozzatti P et al. (2008). In vitro activity of essential oils extracted from plants used as spices against fluconazole-resistant and fluconazole-susceptible Candida spp. Canadian Journal of Microbiology. — PubMed
- Bona E et al. (2016). Sensitivity of Candida albicans to essential oils: are they an alternative to antifungal agents? Journal of Applied Microbiology. — PubMed
- Ahmad A et al. (2011). In vitro synergy of eugenol and methyleugenol with fluconazole against clinical Candida isolates. Journal of Medical Microbiology. — PubMed
- Doke SK, Raut JS, Dhawale S, Karuppayil SM (2014). Sensitization of Candida albicans biofilms to fluconazole by terpenoids of plant origin. Journal of General and Applied Microbiology. — PubMed
- Chami N, Chami F, Bennis S, Trouillas J, Remmal A (2004). Antifungal treatment with carvacrol and eugenol of oral candidiasis in immunosuppressed rats. Brazilian Journal of Infectious Diseases. — PubMed
- Inouye S, Uchida K, Nishiyama Y, Hasumi Y, Yamaguchi H, Abe S (2007). Combined effect of heat, essential oils and salt on fungicidal activity against Trichophyton mentagrophytes. Nippon Ishinkin Gakkai Zasshi. — PubMed
- Khan MS, Ahmad I (2011). Antifungal activity of essential oils and their synergy with fluconazole against drug-resistant strains of Aspergillus fumigatus and Trichophyton rubrum. Applied Microbiology and Biotechnology. — PubMed
- Cleff MB et al. (2010). In vitro activity of Origanum vulgare essential oil against Candida species. Brazilian Journal of Microbiology. — PubMed
- Nostro A et al. (2009). Candida albicans susceptibility to oregano essential oil and carvacrol. Journal of Applied Microbiology. — PubMed
- Salgueiro LR et al. (2003). Chemical composition and antifungal activity of the essential oil of Origanum vulgare. Phytotherapy Research. — PubMed
- Stringaro A, Colone M, Angiolella L (2018). Antioxidant, antifungal, antibiofilm, and cytotoxic activities of Mentha spp. essential oils — carvacrol comparison. Medicines. — PubMed
PubMed Topic Searches
- PubMed: Oregano and Candida albicans
- PubMed: Carvacrol and ergosterol antifungal
- PubMed: Oregano and dermatophytes
- PubMed: Oregano and onychomycosis
- PubMed: Oregano and fluconazole-resistant Candida
Connections
- Oregano Overview
- Oregano Benefits Hub
- Oregano Antibacterial Spectrum
- Oregano Antiparasitic & SIBO
- Oregano Antioxidant & Respiratory
- Antibacterial Herbs
- Thyme
- Tea Tree (antifungal)
- Neem
- Olive Leaf
- Garlic (antifungal)
- Gut Healing
- Parasites
- Acne
- All Herbs