Garlic for Cardiovascular Health & Blood Pressure
The most clinically actionable use of garlic in modern medicine is the treatment of mild-to-moderate hypertension with standardized aged garlic extract (AGE). The flagship body of evidence is a series of randomized trials and meta-analyses by Karin Ried and colleagues at the University of Adelaide, conducted from 2008 to 2020, consistently showing approximately −8 mmHg systolic and −5 mmHg diastolic blood-pressure reduction at 480-960 mg per day of Kyolic-type AGE in hypertensive adults — an effect size that is genuinely comparable to a low-dose first-line antihypertensive drug. The mechanism is now well-mapped: allyl sulfur compounds in AGE donate hydrogen sulfide (H2S) and enhance nitric oxide (NO) bioavailability in the vascular endothelium, the two principal endogenous vasodilator gasotransmitters. This page walks through the trial evidence, the proper preparation and dosing, the realistic place of garlic in a hypertension treatment plan, and the meaningful cautions — especially the antiplatelet bleeding-risk interaction with prescription anticoagulants and with surgery.
Table of Contents
- How Garlic Lowers Blood Pressure — The Gasotransmitter Mechanism
- Nitric Oxide Donation and Endothelial Function
- Hydrogen Sulfide as the Third Vasodilator Gasotransmitter
- Karin Ried's Meta-Analyses (2008-2020)
- Effect Size vs First-Line Antihypertensives
- Aged Garlic Extract vs Fresh Garlic vs Powdered Tablets
- Practical Dosing — AGE for Hypertension
- Beyond Blood Pressure: Arterial Stiffness, Endothelial Function, Gut Microbiome
- Combining Garlic with Prescription Antihypertensives
- Cautions — Bleeding Risk, Surgery, Anticoagulant Interactions
- Key Research Papers
- Connections
- Featured Videos
How Garlic Lowers Blood Pressure — The Gasotransmitter Mechanism
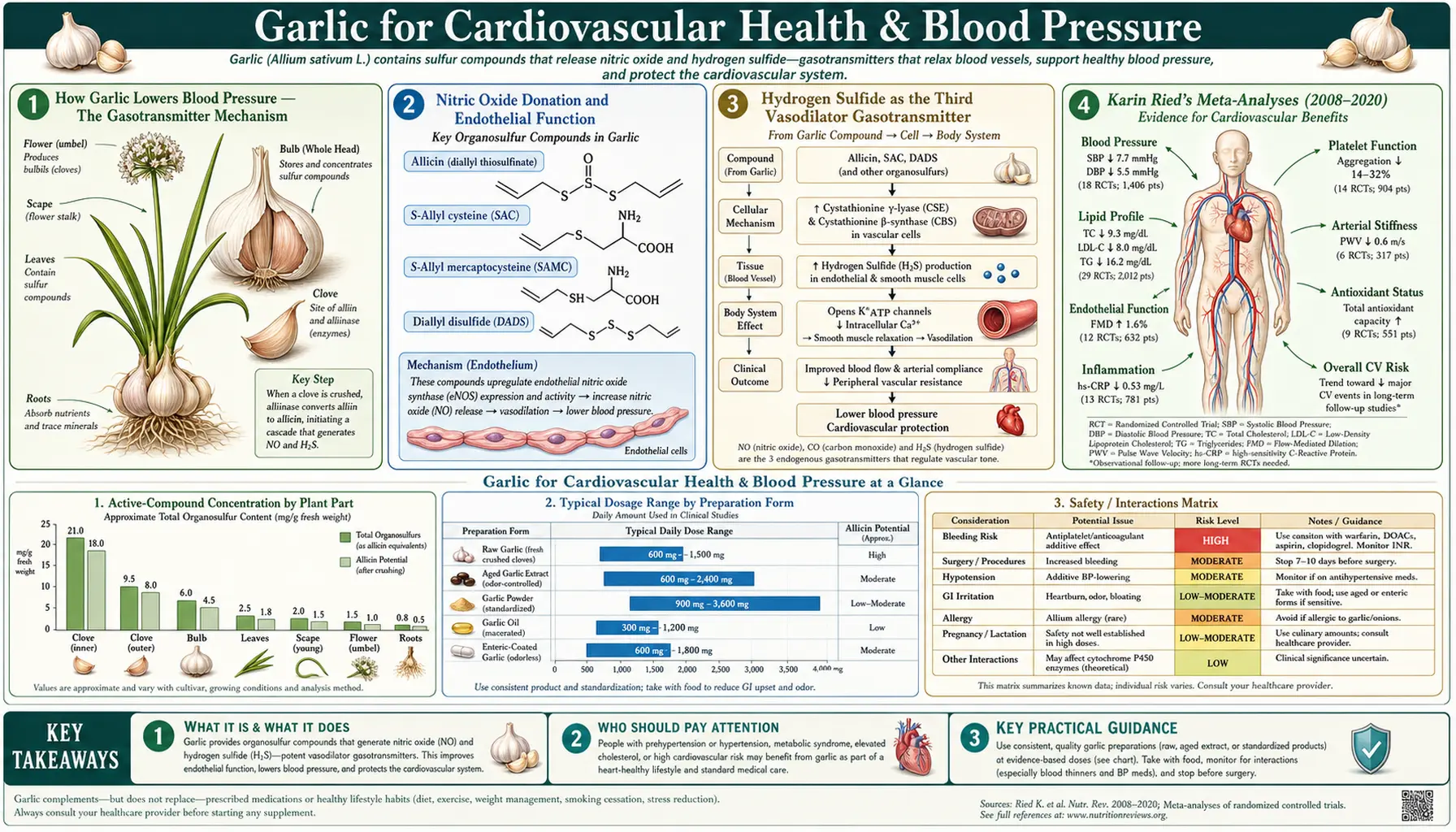
The mechanism by which garlic lowers blood pressure is now understood at the level of molecular pharmacology, and it is the same family of mechanisms that explains the clinical effects of organic nitrates (nitroglycerin, isosorbide mononitrate) and that explains the existence of nitric-oxide-mediated drug classes like sildenafil. Garlic-derived organosulfur compounds donate two distinct endothelium-derived vasodilator gases — nitric oxide (NO) and hydrogen sulfide (H2S) — in the vicinity of the vascular smooth muscle cell, triggering smooth-muscle relaxation, vasodilation, and a measurable drop in systemic arterial pressure.
The unique feature of garlic compared to the synthetic nitrate drugs is that it does not produce tachyphylaxis (tolerance) with sustained dosing the way nitroglycerin does, and that the effect is endothelium-dependent (it requires intact, functional endothelial cells), so it is a gentler, more physiologic stimulus to the same final pathway. The downside is that the effect is modest in magnitude (single-agent reductions in the range achievable by a single low-dose conventional antihypertensive), it requires sustained daily dosing for full effect (typically 8-12 weeks before maximum benefit), and the optimal preparation is aged garlic extract rather than the more familiar dietary forms.
The full cascade looks roughly like this: oral AGE delivers S-allyl cysteine (SAC) and small quantities of allyl polysulfides into systemic circulation. In the vascular endothelium, these compounds are metabolized in the presence of reduced glutathione to release hydrogen sulfide. H2S diffuses into adjacent vascular smooth-muscle cells, where it activates ATP-sensitive potassium channels (KATP), hyperpolarizes the cell, reduces calcium influx, and triggers smooth-muscle relaxation. In parallel, garlic compounds upregulate endothelial nitric oxide synthase (eNOS) activity and protect existing NO from oxidative inactivation, enhancing the NO arm of vasodilation. The net effect is reduced peripheral vascular resistance and a modest, sustained drop in arterial blood pressure.
Nitric Oxide Donation and Endothelial Function
Nitric oxide is the most thoroughly characterized of the three known gasotransmitters and is the dominant moment-to-moment regulator of vascular tone. It is produced in vascular endothelial cells by the enzyme endothelial nitric oxide synthase (eNOS) from the substrate L-arginine, in a reaction that requires the cofactor tetrahydrobiopterin (BH4). NO diffuses across the endothelial cell membrane to the adjacent vascular smooth muscle, where it activates soluble guanylate cyclase, raises intracellular cyclic GMP, and triggers smooth-muscle relaxation.
Endothelial dysfunction — the loss of normal NO-mediated vasodilator capacity — is one of the earliest measurable abnormalities in essentially all forms of cardiovascular disease, including hypertension, atherosclerosis, diabetes, and the metabolic syndrome. The Morihara 2002 (Life Sciences) and Williams 2005 (Phytotherapy Research) trials demonstrated that aged garlic extract enhances NO production both in cell culture (cultured human umbilical vein endothelial cells, HUVECs) and in vivo (men with established coronary artery disease, measured by brachial-artery flow-mediated dilation). The mechanism is twofold: AGE compounds upregulate eNOS mRNA and protein, increasing the enzymatic capacity to make NO; and they reduce oxidative inactivation of NO by superoxide (an effect attributable to the antioxidant capacity of S-allyl cysteine and related thiol-rich compounds).
This dual mechanism — more NO produced, less NO destroyed — is conceptually similar to the rationale for prescribing L-arginine or L-citrulline as cardiovascular supplements, though garlic has a stronger randomized-trial evidence base for the actual clinical endpoint of blood-pressure reduction. The Kim-Park / Ku 2000 study (Clinical and Experimental Pharmacology) provided one of the early animal-model demonstrations that garlic-induced vasorelaxation is endothelium-dependent and is abolished by NOS inhibitors, establishing the centrality of the NO mechanism.
Hydrogen Sulfide as the Third Vasodilator Gasotransmitter
The recognition of hydrogen sulfide as a physiologic gasotransmitter is more recent — the modern era of H2S vascular biology began in the late 1990s and early 2000s, well after NO and carbon monoxide had been established. H2S is produced endogenously by three enzymes (cystathionine-β-synthase, cystathionine-γ-lyase, and 3-mercaptopyruvate sulfurtransferase) using L-cysteine as the principal substrate. In the vasculature, H2S produces vasodilation primarily by activating ATP-sensitive potassium channels (KATP) in vascular smooth muscle, leading to hyperpolarization and reduced calcium-dependent contraction. It also enhances NO bioavailability through complex cross-talk with the NO pathway.
The Benavides et al. 2007 paper in PNAS was the breakthrough demonstration that garlic's organosulfur compounds — specifically diallyl polysulfides — act as H2S donors in vascular tissue, releasing H2S in the presence of reduced glutathione at biologically meaningful concentrations. The vasoactivity of garlic in isolated rat aortic ring preparations correlated tightly with H2S production, and blockade of KATP channels abolished the response. This was the first molecular-level explanation for the long-observed but mechanistically obscure vasodilator effect of garlic.
The clinical relevance is that aged garlic extract, by delivering both S-allyl cysteine (which feeds into endogenous H2S biosynthesis via the cysteine pool) and small quantities of allyl polysulfides (which directly donate H2S), provides sustained, low-grade H2S signaling without the toxicity that would result from acute high-dose exposure (H2S at high concentration is a well-known mitochondrial poison). The body's natural H2S pathway provides the safety margin that synthetic H2S donor drugs (currently in early development) have to demonstrate the hard way.
Karin Ried's Meta-Analyses (2008-2020)
The single most important investigator in modern garlic-and-blood-pressure research is Karin Ried at the University of Adelaide and the Australian National Institute of Integrative Medicine. Ried has published a series of randomized controlled trials and meta-analyses, summarized below in roughly chronological order:
- Ried 2008 (BMC Cardiovascular Disorders) — the first comprehensive meta-analysis of all available garlic-and-blood-pressure RCTs (11 trials, 553 hypertensive subjects). Garlic preparations reduced systolic BP by 8.4 mmHg and diastolic by 7.3 mmHg in hypertensives compared with placebo; the effect in normotensives was much smaller and non-significant. This is the headline finding that established garlic as a credible BP-lowering agent in the modern era.
- Ried 2013 dose-response trial (European Journal of Clinical Nutrition) — a head-to-head comparison of 240, 480, and 960 mg/day of Kyolic AGE in uncontrolled hypertensives over 12 weeks. The 480 and 960 mg doses produced significant systolic BP reduction of 11.5 mmHg and 11.8 mmHg respectively over placebo; 240 mg was not different from placebo. This established 480 mg/day as the effective floor.
- Ried 2016 ("GarGIC" trial) — an extended trial showing that 12 months of AGE in hypertensives also improved arterial stiffness (pulse-wave velocity) and produced favorable shifts in the gut microbiome, suggesting effects beyond direct vasodilation.
- Ried 2020 review (Experimental and Therapeutic Medicine) — the most recent comprehensive review, summarizing 12 years of trials and pooling 17 RCTs in hypertensives. Mean systolic BP reduction of 8.3 mmHg, mean diastolic reduction of 5.5 mmHg, with consistent effects across multiple AGE preparations and dosing regimens. The review also documents improvements in arterial stiffness, endothelial function, and the gut microbiome.
The pattern across the Ried series is striking in its consistency: the effect is robust in hypertensives, much smaller in normotensives, dose-dependent above a threshold of approximately 300-400 mg/day of AGE, and replicated with multiple preparations from multiple manufacturers. The 2012 Cochrane review by Stabler and colleagues was more cautious in its conclusions, emphasizing the methodological weaknesses of many of the included trials, but the more recent updates incorporating higher-quality RCTs have moved the consensus toward acceptance of a real, modest, clinically useful BP-lowering effect.
Effect Size vs First-Line Antihypertensives
An 8-mmHg systolic blood-pressure reduction sounds small until it is put in context with what the first-line conventional antihypertensive drug classes achieve as single agents in similar populations. A representative comparison from the JNC-8 and subsequent hypertension trial literature:
- Thiazide diuretics (hydrochlorothiazide 25 mg/day, chlorthalidone 12.5-25 mg/day) — approximately 8-12 mmHg systolic reduction as monotherapy
- ACE inhibitors (lisinopril 10-40 mg/day, ramipril 5-10 mg/day) — approximately 8-12 mmHg systolic reduction as monotherapy
- Angiotensin receptor blockers (ARBs) (losartan 50-100 mg/day, valsartan 80-320 mg/day) — approximately 8-13 mmHg systolic reduction
- Calcium channel blockers (amlodipine 5-10 mg/day) — approximately 8-15 mmHg systolic reduction
- Aged garlic extract (Kyolic 480-960 mg/day) — approximately 8-12 mmHg systolic reduction in the Ried trials
This is not to suggest that aged garlic extract is interchangeable with a thiazide or an ACE inhibitor in a patient with stage-2 hypertension or with established cardiovascular disease — the prescription drugs have decades of randomized morbidity-and-mortality outcome data behind them (HOPE, ALLHAT, ONTARGET, etc.) and garlic does not. What the comparison does establish is that for a patient with mild (stage-1) hypertension who wants to try lifestyle and non-pharmaceutical interventions first — weight loss, DASH diet, sodium restriction, exercise — the addition of standardized aged garlic extract is a legitimate evidence-based component of that strategy and is one of the few herbal interventions with effect sizes that approach those of single-agent prescription drugs.
The patient population most likely to benefit, per the Ried trial inclusion criteria, is the adult with baseline systolic BP in the 140-160 range, no compelling indication for a specific drug class (such as proteinuric diabetes or post-MI status), and a preference for non-pharmaceutical management. For more on the management of high blood pressure as a whole, see our Hypertension page.
Aged Garlic Extract vs Fresh Garlic vs Powdered Tablets
One of the most common patient questions is: "Can I just eat fresh garlic instead of taking the supplement?" The honest answer is "probably not for the blood-pressure indication, and here is why." The Ried trials and the bulk of the modern cardiovascular literature have used standardized Kyolic-type aged garlic extract for specific reasons:
- Standardization — AGE is standardized to a defined content of S-allyl cysteine (typically 0.6-1.0 mg per 600 mg capsule). Fresh garlic varies dramatically in allicin-yielding potential by cultivar, growing region, time since harvest, and storage conditions.
- Stability — SAC and S-allyl mercaptocysteine in AGE are stable in storage for years. Allicin from fresh garlic decomposes within days at room temperature and within hours once dissolved in saliva or gastric fluid.
- Tolerability — AGE is essentially odorless. Fresh garlic at the dose required to deliver an equivalent amount of allyl sulfur compounds (estimated at roughly four to five cloves per day) produces severe halitosis, body odor, and gastrointestinal irritation in most users, making sustained compliance unrealistic.
- Trial evidence — the randomized cardiovascular evidence is almost exclusively from AGE, with smaller and more inconsistent evidence from powdered garlic tablets and very little from fresh garlic.
Powdered garlic tablets (Kwai, Garlique, and similar) occupy an intermediate position. They contain dried, powdered garlic in a coated tablet that is designed to release allicin upon contact with intestinal fluid (the alliinase enzyme survives the drying process if it is not over-heated). The clinical evidence for powdered tablets is mixed, in part because the actual allicin yield varies dramatically from tablet to tablet and from brand to brand — the Sobenin 2008 trial of a time-released powdered garlic tablet did show meaningful lipid-lowering, but most negative garlic trials in the literature have used powdered preparations of uncertain real-world allicin yield.
Garlic oil (the steam-distilled lipid-soluble fraction) is concentrated in diallyl disulfide and diallyl trisulfide. The animal evidence for cardiovascular effects with garlic oil is strong, but the human cardiovascular trial data are limited and most garlic-oil capsules on the consumer market are sold for general "heart health" without specific BP claims or standardization.
The pragmatic recommendation: for the specific indication of blood-pressure management, use standardized aged garlic extract (Kyolic or equivalent), 480-960 mg/day in divided doses, for at least 12 weeks before judging effect. Continue dietary fresh garlic for its culinary value and general phytochemical contribution to the diet but do not rely on it as the BP intervention.
Practical Dosing — AGE for Hypertension
For mild-to-moderate hypertension in an adult who wants to try aged garlic extract as part of a non-pharmaceutical or pharmaceutical-sparing strategy:
- Starting dose: 480 mg of standardized AGE (typically two 240-mg or 250-mg capsules of Kyolic or equivalent) per day, taken with food.
- Maintenance dose: 480-960 mg/day in divided doses (morning and evening). The 960-mg dose is supported by the Ried dose-response data; some patients tolerate splitting into three daily doses better than two.
- Time to effect: initial BP reduction is typically seen at 4 weeks; maximum effect at 8-12 weeks. Do not judge effect before 8 weeks of consistent daily use.
- Monitoring: home BP monitor, twice-daily readings averaged over 7 days before and at the 8-week mark. This is the same regimen recommended for evaluating any new antihypertensive intervention.
- What to expect: a typical responder will see a sustained 6-10 mmHg drop in average systolic BP and a 3-5 mmHg drop in diastolic. Non-responders (no measurable change at 12 weeks) exist; about one in four hypertensives does not respond meaningfully to AGE.
For a patient already on a prescription antihypertensive, do not stop the prescription drug without consultation with the prescribing physician. Garlic added on top of a prescription drug can produce additive BP-lowering — appropriate if there is room to lower BP further, potentially problematic if it produces symptomatic hypotension or orthostasis. The standard approach is to add AGE to an existing regimen, monitor BP at 8-12 weeks, and if BP is now too low or borderline-too-low, request the prescriber to step down the prescription drug dose rather than discontinue the garlic.
Beyond Blood Pressure: Arterial Stiffness, Endothelial Function, Gut Microbiome
The Ried 2016 GarGIC trial and the broader Ried 2020 review document several effects of sustained AGE supplementation that go beyond the simple blood-pressure number:
- Arterial stiffness — pulse-wave velocity (PWV), an independent cardiovascular risk marker, improves modestly over 12 months of AGE supplementation in hypertensives. This implies a structural or vasomotor benefit to the large conduit arteries, not just a smooth-muscle tone effect.
- Endothelial function — flow-mediated dilation of the brachial artery, an established surrogate for endothelial health, improves with AGE in patients with coronary artery disease (Williams 2005). This is the functional readout of the NO and H2S mechanisms described above.
- Gut microbiome — AGE in the GarGIC trial produced a shift toward greater microbial diversity and a small increase in Lactobacillus and Clostridia clusters known to produce short-chain fatty acids. Whether this is a primary mechanism of the BP effect or an epiphenomenon is unresolved; the AGE-microbiome-vascular-tone axis is an active research area.
- Coronary artery calcium (CAC) progression — documented in the related Budoff 2009 trial, in which AGE plus B-vitamins / folate / L-arginine slowed CAC accumulation over one year (covered in detail in the Cholesterol & Atherosclerosis page).
- Glycemic control — some evidence for modest improvement in fasting glucose and HbA1c in metabolic-syndrome patients, of unclear clinical magnitude but consistent direction.
Combining Garlic with Prescription Antihypertensives
Aged garlic extract is generally well tolerated in combination with the major classes of conventional antihypertensive drugs. The principal interaction to anticipate is additive BP-lowering, which is usually the desired effect but occasionally requires dose adjustment of the prescription drug:
- ACE inhibitors and ARBs — additive BP-lowering, no specific pharmacokinetic interaction documented. Monitor for symptomatic hypotension and orthostatic symptoms.
- Calcium channel blockers — additive BP-lowering, no documented pharmacokinetic interaction.
- Thiazide diuretics — additive BP-lowering. AGE does not appear to potentiate the diuretic effect or alter electrolytes.
- Beta-blockers — additive BP-lowering; no documented heart-rate interaction.
- Aldosterone antagonists (spironolactone, eplerenone) — additive BP-lowering; no known potassium interaction.
- Vasodilators (hydralazine, minoxidil) — additive BP-lowering, more likely to produce symptomatic hypotension when combined; titrate cautiously.
The unambiguous interaction to manage is with antiplatelet and anticoagulant drugs — see the Cautions section below.
Cautions — Bleeding Risk, Surgery, Anticoagulant Interactions
- Antiplatelet / anticoagulant interaction — this is the headline safety concern with garlic at therapeutic doses. Allicin and especially ajoene inhibit platelet aggregation in vitro and in vivo. Patients on warfarin, clopidogrel, prasugrel, ticagrelor, dabigatran, apixaban, rivaroxaban, or chronic high-dose aspirin should consult their physician before adding garlic supplements. The interaction is not absolute — many patients on aspirin or warfarin take garlic supplements safely — but the bleeding risk requires individual assessment and possibly INR monitoring (for warfarin) or evaluation of bleeding/bruising trends.
- Surgery — discontinue all garlic supplements at least 7 days before any planned surgical or dental procedure with bleeding risk. This is the same time frame used for fish oil and ginkgo. The American Society of Anesthesiologists includes garlic on its standard list of supplements to discontinue pre-operatively.
- Childbirth — the same discontinuation principle applies; many obstetric protocols recommend stopping garlic supplements by 36 weeks gestation in anticipation of possible delivery-related bleeding.
- Gastrointestinal irritation — fresh garlic at high doses can produce heartburn, esophagitis, and nausea. AGE is much better tolerated; gastrointestinal complaints with AGE are uncommon at standard doses.
- Hypotension at the lower end of normal BP — patients with baseline BP under approximately 110/70 should be cautious about adding AGE; the additive effect is small in normotensives but real, and a few patients have reported symptomatic orthostasis after starting garlic supplements.
- HIV protease inhibitor interaction (saquinavir specifically) — garlic supplements have been documented to reduce saquinavir plasma concentrations meaningfully. Patients on antiretroviral therapy should consult their HIV specialist before using high-dose garlic supplements.
- Pregnancy — dietary garlic is safe and traditional in cuisines worldwide. High-dose garlic supplements have not been specifically studied in pregnancy; caution is reasonable, particularly in the third trimester given the bleeding-risk concern.
- Children — garlic as food is appropriate at any age. High-dose garlic supplements for blood-pressure indications are not standard in pediatric practice; pediatric hypertension should be evaluated by a pediatric nephrologist or cardiologist.
Key Research Papers
- Ried K, Frank OR, Stocks NP, Fakler P, Sullivan T (2008). Effect of garlic on blood pressure: a systematic review and meta-analysis. BMC Cardiovascular Disorders 8:13. — PubMed
- Ried K, Frank OR, Stocks NP (2013). Aged garlic extract reduces blood pressure in hypertensives: a dose-response trial. European Journal of Clinical Nutrition 67:64-70. — PubMed
- Ried K (2016). Garlic lowers blood pressure in hypertensive individuals, regulates serum cholesterol, and stimulates immunity: an updated meta-analysis and review. Journal of Nutrition. — PubMed
- Ried K (2020). Garlic lowers blood pressure in hypertensive subjects, improves arterial stiffness and gut microbiota: A review and meta-analysis. Experimental and Therapeutic Medicine 19(2):1472-1478. — PubMed
- Stabler SN, Tejani AM, Huynh F, Fowkes C (2012). Garlic for the prevention of cardiovascular morbidity and mortality in hypertensive patients. Cochrane Database of Systematic Reviews. — PubMed
- Benavides GA, Squadrito GL, Mills RW et al. (2007). Hydrogen sulfide mediates the vasoactivity of garlic. PNAS 104:17977-17982. — PubMed
- Morihara N, Sumioka I, Moriguchi T, Uda N, Kyo E (2002). Aged garlic extract enhances production of nitric oxide. Life Sciences 71:509-517. — PubMed
- Williams MJA, Sutherland WHF, McCormick MP, Yeoman DJ, de Jong SA (2005). Aged garlic extract improves endothelial function in men with coronary artery disease. Phytotherapy Research 19:314-319. — PubMed
- Wang HP, Yang J, Qin LQ, Yang XJ (2015). Effect of garlic on blood pressure: a meta-analysis. Journal of Clinical Hypertension 17:223-231. — PubMed
- Kim-Park S, Ku DD (2000). Garlic elicits a nitric oxide-dependent relaxation and inhibits hypoxic pulmonary vasoconstriction in rats. Clinical and Experimental Pharmacology and Physiology 27:780-786. — PubMed
- Ginter E, Simko V (2010). Garlic (Allium sativum L.) and cardiovascular diseases. Bratislava Medical Journal 111(8):452-456. — PubMed
- Ashraf R, Khan RA, Ashraf I (2013). Garlic (Allium sativum) supplementation with standard antidiabetic agent provides better diabetic control in type 2 diabetes patients. Pakistan Journal of Pharmaceutical Sciences. — PubMed
PubMed Topic Searches
- PubMed: Garlic and blood pressure
- PubMed: Aged garlic extract / Kyolic and hypertension
- PubMed: Allicin and hydrogen sulfide vasodilation
- PubMed: Garlic and nitric oxide / endothelial function
- PubMed: Garlic / warfarin / antiplatelet interaction
Connections
- Garlic Overview
- Garlic Benefits Hub
- Garlic for Cholesterol & Atherosclerosis
- Garlic for Immune Function & Cold
- Garlic Antimicrobial Spectrum
- Hypertension
- Cardiovascular Disease
- Atherosclerosis
- Stroke
- Homocysteine
- Magnesium (BP)
- Potassium (BP)
- Hawthorn
- DASH Diet
- All Herbs